中国组织工程研究 ›› 2019, Vol. 23 ›› Issue (20): 3117-3123.doi: 10.3969/j.issn.2095-4344.1192
• 人工假体 artificial prosthesis • 下一篇
直接前侧入路全髋关节置换是否导致髋臼前壁偏心磨挫?
苏联彬1,2,冯尔宥1,张怡元1,2,卓有光1,2,肖莉莉1,王武炼1,林飞太1
- 1厦门大学附属福州第二医院关节外科,福建省福州市 350007;2厦门大学医学院,福建省厦门市 361005
-
出版日期:2019-07-18发布日期:2019-07-18 -
通讯作者:张怡元,主任医师,教授,硕士生导师,厦门大学附属福州第二医院关节外科,福建省福州市 350007;厦门大学医学院,福建省厦门市 361005 -
作者简介:苏联彬,男,1992年生,福建省人,汉族,厦门大学在读硕士。 -
基金资助:福建省自然科学基金(2017J01333),项目负责人:冯尔宥
Whether direct anterior approach for total hip arthroplasty is a risk factor of eccentric reaming to the anterior column of the acetabulum?
Su Lianbin1, 2, Feng Eryou1, Zhang Yiyuan1, 2, Zhuo Youguang1, 2, Xiao Lili1, Wang Wulian1, Lin Feitai1
- 1Department of Joint Surgery, FuZhou Second Hospital of Xiamen University, Fuzhou 350007, Fujian Province, China; 2Medical College of Xiamen University, Xiamen 361005, Fujian Province, China
-
Online:2019-07-18Published:2019-07-18 -
Contact:Zhang Yiyuan, Chief physician, Professor, Master’s supervisor, Department of Joint Surgery, FuZhou Second Hospital of Xiamen University, Fuzhou 350007, Fujian Province, China; Medical College of Xiamen University, Xiamen 361005, Fujian Province, China -
About author:Su Lianbin, Master candidate, Department of Joint Surgery, FuZhou Second Hospital of Xiamen University, Fuzhou 350007, Fujian Province, China; Medical College of Xiamen University, Xiamen 361005, Fujian Province, China -
Supported by:the Natural Science Foundation of Fujian Province, No. 2017J01333 (to FEY)
摘要:
文题释义:
中图分类号:
引用本文
苏联彬,冯尔宥,张怡元,卓有光,肖莉莉,王武炼,林飞太. 直接前侧入路全髋关节置换是否导致髋臼前壁偏心磨挫?[J]. 中国组织工程研究, 2019, 23(20): 3117-3123.
Su Lianbin, Feng Eryou, Zhang Yiyuan, Zhuo Youguang, Xiao Lili, Wang Wulian, Lin Feitai. Whether direct anterior approach for total hip arthroplasty is a risk factor of eccentric reaming to the anterior column of the acetabulum?[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(20): 3117-3123.
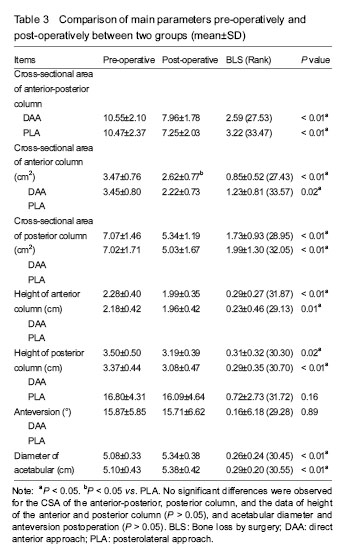
Comparison of perioperative parameters between PLA or DAA groups
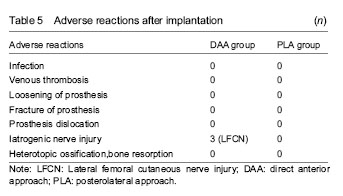
Adverse reactions
| [1] Moretti V, Post Z. Surgical approaches for total hip arthroplasty Indian J Orthop. 2017;51(4):368-376.[2] Jordan J, Helmick J, Renner B, et al. Prevalence of hip symptoms and radiographic and symptomatic hip osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project. J Rheumatol. 2009;36(4):809-815. [3] Maradit Kremers H, Larson DR, Crowson CS, et al. Prevalence of total hip and knee replacement in the United States. J Bone Joint Surg Am. 2015;97(17):1386-1397.[4] Singh JA. Epidemiology of knee and hip arthroplasty: a systematic review. Open Orthop J. 2011;16(5):80-85. [5] Petis S, Howard JL, Lanting BL, et al. Surgical approach in primary total hip arthroplasty: anatomy, technique and clinical outcomes. Can J Surg. 2015;58(2):128-139. [6] Connolly KP, Kamath AF. Direct anterior total hip arthroplasty: literature review of variations in surgical technique.World J Orthop. 2016;7(1):38-43. [7] Ji W, Stewart N. Fluoroscopy assessment during anterior minimally invasive hip replacement is more accurate than with the posterior approach. Int Orthop. 2016;40(1):21-27. [8] Zhang YJ, Li J, Qi K, et al. Comparison of efficacy and safety between the anterior and the posterior approaches to total hip arthroplasty. Beijing Da Xue Xue Bao. 2017;49(2):201-205. [9] Lin TJ, Bendich I, Ha AS, et al. A comparison of radiographic outcomes after total hip arthroplasty between the posterior approach and direct anterior approach with intraoperative fluoroscopy. J Arthroplasty. 2017;32(2):616-623. [10] Post ZD, Orozco F, Diaz-Ledezma C,et al. Direct anterior approach for total hip arthroplasty: indications, technique, and results. J Am Acad Orthop Surg. 2014;22(9):595-603. [11] Radoicic D, Zec V, Elassuity WI, et al. Patient's perspective on direct anterior versus posterior approach total hip arthroplasty. Int Orthop. 2018;42(12):2771-2775. [12] Nistor DV, Caterev S,. Bolboaca SD, et al. Transitioning to the direct anterior approach in total hip arthroplasty. Is it a true muscle sparing approach when performed by a low volume hip replacement surgeon? Int Orthop. 2017;41(11):2245-2252. [13] Seng BE, Berend KR, Ajluni AF, et al. Anterior-supine minimally invasive total hip arthroplasty: defining the learning curve. Orthop Clin North Am. 2009;40(3):343-350. [14] Kobayashi H, Homma Y. Surgeons changing the approach for total hip arthroplasty from posterior to direct anterior with fluoroscopy should consider potential excessive cup anteversion and flexion implantation of the stem in their early experience. Int Orthop.2016;40(9):1813-1819. [15] Barton C, Kim PR. Complications of the direct anterior approach for total hip arthroplasty. Orthop Clin North Am. 2009;40(3):371-375. [16] Chechik O, Khashan M, Lador R, et al. Surgical approach and prosthesis fixation in hip arthroplasty world wide. Arch Orthop Trauma Surg. 2013;133(11):1595-600.[17] Holst DC, Yang CC. Surgical anatomy of the direct anterior approach for total hip arthroplasty. Ann Joint. 2018;3:23-23.[18] Uemura K, Takao M. Sakai T, et al. Volume increases of the gluteus maximus, gluteus medius, and thigh muscles after hip arthroplasty. J Arthroplasty. 2016;31(4):906-912. [19] Xu D, Koyama H, Furuhashi H, et al. Comparison of hip muscle volume between fit-and-fill stem and tapered-wedge stem after total hip arthroplasty using the anterolateral approach. J Orthop Sci. 2017;22(6):1102-1106. [20] Tongdee T, Keawaen P, Tongdee R. Evaluation of standard liver volume in adult Thai population using CT volumetric measurement. J Med Assoc Thai. 2013;96(2):217-2124.[21] Dandachli W, Islam UL, Tippettr R, et al. Analysis of acetabular version in the native hip: comparison between 2D axial CT and 3D CT measurements. Skeletal Radiol. 2011;40(7):877-883. [22] Pankal A, Mittal A, Chawla A. The validity and reproducibility of cross table radiographs compared with CT scans for the measurement of anteversion of the acetabular component after total hip arthroplasty. Bone Joint J. 2017;99-b(8):1006-1011. [23] Nomura T, Naito M, Nakamura Y, et al. An analysis of the best method for evaluating anteversion of the acetabular component after total hip replacement on plain radiographs. Bone Joint J. 2014;96-b(5):597-603. [24] Shemesh S, Robinson S, Keswani A, et al. The accuracy of digital templating for primary total hip arthroplasty: is there a difference between direct anterior and posterior approaches? J Arthroplasty. 2017;32(6):1884-1889. [25] Hartford JM, Knowles SB. Risk factors for perioperative femoral fractures: cementless femoral implants and the direct anterior approach using a fracture table. J Arthroplasty. 2016;31(9): 2013-2018.[26] Wang Z, Hou JZ, Wu CH, et al. A systematic review and meta-analysis of direct anterior approach versus posterior approach in total hip arthroplasty. J Orthop Surg Res. 2018;13(1): 229-240. [27] Cheng TE, Wallis JA, Taylor NF, et al. A prospective randomized clinical trial in total hip arthroplasty-comparing early results between the direct anterior approach and the posterior approach. J Arthroplasty. 2017;32(3):883-890. [28] Cadossi M, Sambri A, Tedesco G, et al. Anterior approach in total hip replacement. Orthopedics. 2017;40(3):e553-556.[29] Pilliar RM, Leeand J, Maniatopoulos C. Observations on the effect of movement on bone ingrowth into porous-surfaced implants. Clin Orthop Relat Res. 1986;(208):108-113. [30] Fehring K, Owen A. Kurdin A, et al. Initial stability of press-fit acetabular components under rotational forces. J Arthroplasty. 2014;29(5):1038-1042. [31] Markel D, Horaand N, Grimm M. Press-fit stability of uncemented hemispheric acetabular components: a comparison of three porous coating systems. Int Orthop. 2002;26(2):72-75. [32] Saleh K, Bear B, Wright T, et al. Initial stability of press-fit acetabular components: an in vitro biomechanical study. Am J Orthop. 2008;37(10):519. [33] Kim YH. Acetabular Cup Revision. Hip Pelvis. 2017;29(3):155-158.[34] Lingaraj K, Teoand YH, Bergman N. The management of severe acetabular bone defects in revision hip arthroplasty using modular porous metal components. J Bone Joint Surg Br. 2009;91(12):1555-1560. [35] Meneghini RM, Elston AS, Chen AF, et al. Direct anterior approach: risk factor for early femoral failure of cementless total hip arthroplasty: a multicenter study. J Bone Joint Surg Am. 2017;99(2):99-105. [36] Homma Y, Baba T, Sano K, et al. Lateral femoral cutaneous nerve injury with the direct anterior approach for total hip arthroplasty. Int Orthop. 2016;40(8):1587-1593. [37] Eto S, Hwang K, Huddleston JI, et al. The direct anterior approach is associated with early revision total hip arthroplasty. J Arthroplasty. 2017;32(3):1001-1005. [38] Ozaki Y, Homma Y, Baba T, et al. Spontaneous healing of lateral femoral cutaneous nerve injury and improved quality of life after total hip arthroplasty via a direct anterior approach. J Orthop Surg. 2017;25(1) 1-7. |
| [1] | 张同同, 王中华, 文 杰, 宋玉鑫, 刘 林. 3D打印模型在颈椎肿瘤手术切除与重建中的应用[J]. 中国组织工程研究, 2021, 25(9): 1335-1339. |
| [2] | 张 宇, 田少奇, 曾国波, 胡 川. 初次下肢全关节置换后发生心肌梗死的危险因素[J]. 中国组织工程研究, 2021, 25(9): 1340-1345. |
| [3] | 张 冲, 刘志昂, 姚帅辉, 高军胜, 姜 岩, 张 陆. 局部应用氨甲环酸减少老年股骨颈骨折全髋关节置换后引流的安全和有效性[J]. 中国组织工程研究, 2021, 25(9): 1381-1386. |
| [4] | 王海莹, 吕 冰, 李 辉, 王顺义. 减压植骨融合内固定治疗退变性腰椎滑脱:基于脊柱骨盆参数预测患者的功能预后[J]. 中国组织工程研究, 2021, 25(9): 1393-1397. |
| [5] | 张 超, 吕 欣. 髋臼骨折固定后的异位骨化:危险因素、预防及其治疗进展[J]. 中国组织工程研究, 2021, 25(9): 1434-1439. |
| [6] | 李中峰, 陈明海, 凡一诺, 魏秋实, 何 伟, 陈镇秋. 右归饮治疗激素性股骨头坏死作用机制的网络药理学分析[J]. 中国组织工程研究, 2021, 25(8): 1256-1263. |
| [7] | 曾燕华, 郝延磊. 许旺细胞体外培养及纯化的系统性综述[J]. 中国组织工程研究, 2021, 25(7): 1135-1141. |
| [8] | 刘立华, 孙 伟, 王云亭, 高福强, 程立明, 李子荣, 王江宁. 头颈部开窗减压治疗L1型激素性股骨头坏死:单中心前瞻性临床研究[J]. 中国组织工程研究, 2021, 25(6): 906-911. |
| [9] | 刘 钊, 徐西林, 申意伟, 张晓峰, 吕 航, 赵 军, 王政春, 刘旭卓, 王海涛. 塌陷预测方法联合分期分型对股骨头坏死治疗的指导作用与前景[J]. 中国组织工程研究, 2021, 25(6): 929-934. |
| [10] | 李时斌, 赖 渝, 周 毅, 廖建钊, 章晓云, 张 璇. 激素性股骨头坏死发病机制及相关信号通路的靶点效应[J]. 中国组织工程研究, 2021, 25(6): 935-941. |
| [11] | 郑小龙, 何晓铭, 龚水帝, 庞凤祥, 杨 帆, 何 伟, 刘少军, 魏秋实. 酒精性股骨头坏死患者的骨转换特点[J]. 中国组织工程研究, 2021, 25(5): 657-661. |
| [12] | 徐东紫, 张 婷, 欧阳昭连. 心脏组织工程领域全球专利竞争态势分析[J]. 中国组织工程研究, 2021, 25(5): 807-812. |
| [13] | 吴子健, 胡昭端, 谢有琼, 王 峰, 李 佳, 李柏村, 蔡国伟, 彭 锐. 3D打印技术与骨组织工程研究文献计量及研究热点可视化分析[J]. 中国组织工程研究, 2021, 25(4): 564-569. |
| [14] | 常文辽, 赵 杰, 孙晓亮, 王 锟, 吴国锋, 周 剑, 李树祥, 孙 晗. 人工骨膜的材料选择、理论设计及生物仿生功能[J]. 中国组织工程研究, 2021, 25(4): 600-606. |
| [15] | 刘 旒, 周箐竹, 龚 桌, 刘博言, 杨 斌, 赵 娴. 胶原/无机材料构建组织工程骨的特点及制造技术[J]. 中国组织工程研究, 2021, 25(4): 607-613. |
The procedure can be performed using a variety of surgical approaches, and the posterolateral approach (PLA), direct lateral approach, and direct anterior approach (DAA) are commonly used[5]. The DAA was first described by Carl Hueter in 1881[6]. As it passes through the interval of tensor fasciae latae, the sartorius and rectus femoris muscles to the hip joint, it is a minimal invasive technique with less pain, quicker recovery, lower dislocation risk, better fluoroscopy assessment, higher functional outcomes, and higher patient satisfaction compared with the PLA and direct lateral approach[7-12].
中国组织工程研究杂志出版内容重点:人工关节;骨植入物;脊柱;骨折;内固定;数字化骨科;组织工程
Design
Material properties of implants were shown in Table 1.
.jpg)
.jpg)
PLA: All posterior THAs were performed with a uniform technique as described in the literatures[1, 9]. The operation was completed in a lateral decubitus position on an operating table with pelvic positioners placed posteriorly (sacrum) and anteriorly (pubic symphysis and rami). A curvilinear incision 10- to 15-cm-long that extended 5 cm distal from greater trochanter at the lateral center of the femoral diaphysis to proximally along the posterior border of greater trochanter and then curves toward the posterior superior iliac spine for approximately 7 cm. The iliotibial band was identified and incised, and the gluteus maximus was split along the fibers. The piriformis and the other short external rotators was identified that were tagged with suture and reflected, which could protect the nearby sciatic nerve and expose the posterior hip capsule. Then the capsule was exposed and incised. Along with flexion, adduction, internal rotation of the leg, in order to allows for hip dislocation. Next, the osteotomized level in femoral neck was identified, which was determined from a preoperative plan, and further performed using an oscillating saw. Before the routine acetabular reaming the labrum, pulvinar and any loose soft tissues should be excised. The subsequent preparation of routine acetabular reaming was similar to that of the DAA. The posterior hip capsule was repaired, and the external rotators were reattached during closure.
.jpg)
Using the cross-sectional area (CSA) in CT images as a surrogate for various tissue volume was reliable and applied in clinical research[18-20]. First, we defined the parameters representing the bone stock that possibly be affected by the surgical approach, including the CSA of the anterior and posterior column of the acetabulum, which be considered as a surrogate for bone volume[18], the height of the anterior and posterior column, acetabular diameter and anteversion. Two independent reviewers were blinded to the approach and given a spreadsheet to measure and record the result. A Picture Archiving and Communication System (YiLianZong, version 3.6, China) was used for radiographic measurement (Figure 2). In order to ensure the same cross-sections measured pre-and post-operation, the most important step was to find the equator section of the acetabulum[21, 22]: connecting the bilateral rotation center of the acetabulum (using a template), which defined as the distinction between the anterior and posterior columns, terming the “line A”. The tangent lines through the medial column of the acetabulum, perpendicular to the “line A”, as the base of the anterior and posterior columns, were termed “line B1” and “line B2”, which were parallel but discontinuous. The height of the anterior and posterior columns was defined as the length of a perpendicular line extending from the top point of the anterior and posterior column to the lines B1 and B2. Then, the vertical distance from anterior to posterior as the diameter of the acetabulum was termed line C, plane with the largest distance was defined as the equatorial section. The tangential line across the open face of the cup connecting the anterior and posterior margins of the acetabulum was termed line D, The anteversion of the acetabulum was obtained by subtracting this angle that composed by line D and A from 90°[21-23]. The CSA of the anterior and posterior column was measured by the curve function of Picture Archiving and Communication System (S1 and S2). The same method was used to measure the upper and next sections, and the mean values of the parameters measured in these three sections of the anterior and posterior were calculated and recorded.
.jpg)
中国组织工程研究杂志出版内容重点:人工关节;骨植入物;脊柱;骨折;内固定;数字化骨科;组织工程
.jpg)
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||