中国组织工程研究 ›› 2014, Vol. 18 ›› Issue (4): 577-582.doi: 10.3969/j.issn.2095-4344.2014.04.015
• 骨科植入物 orthopedic implant • 上一篇 下一篇
Ilizarov牵拉架外固定治疗胫骨骨缺损的钢环参数选择
余 凯,杨 晶,杨广忠,艾合买提江,陈柯屹,赵弟庆,袁春晓
- 新疆医科大学第一附属医院骨科,新疆维吾尔自治区乌鲁木齐市 830054
-
修回日期:2013-09-14出版日期:2014-01-22发布日期:2014-01-22 -
通讯作者:杨广忠,主任医师,新疆医科大学第一附属医院骨科,新疆维吾尔自治区乌鲁木齐市 830054 -
作者简介:余凯,男,1987年生,河南省卢氏县人,汉族,新疆医科大学在读硕士,主要从事创伤骨科方面的研究。
Parameter selection for steel ring of Ilizarov external fixation in the treatment of tibial bone defects
Yu Kai, Yang Jing, Yang Guang-zhong, AiHeMaiTiJiang, Chen Ke-yi, Zhao Di-qing, Yuan Chun-xiao
- Department of Orthopedics, the First Affiliated Hospital of Xinjiang Medical University, Urumqi 830054, Xinjiang Uygur Autonomous Region, China
-
Revised:2013-09-14Online:2014-01-22Published:2014-01-22 -
Contact:Yang Guang-zhong, Chief physician, Department of Orthopedics, the First Affiliated Hospital of Xinjiang Medical University, Urumqi 830054, Xinjiang Uygur Autonomous Region, China -
About author:Yu Kai, Studying for master’s degree, Department of Orthopedics, the First Affiliated Hospital of Xinjiang Medical University, Urumqi 830054, Xinjiang Uygur Autonomous Region, China
摘要:
背景:既往尚无有效的方法彻底治疗胫骨骨缺损合并软组织缺损。Ilizarov技术的应用能在一定程度上解决短缩畸形、软组织损伤及关节挛缩等相关问题。
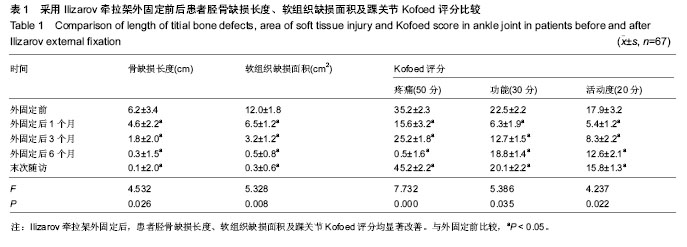
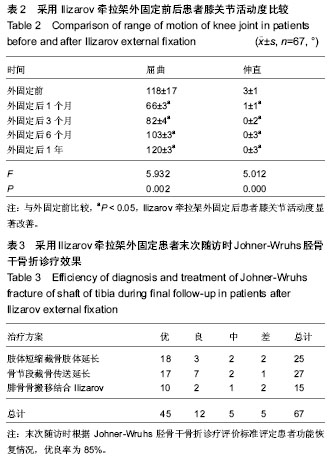
结果与结论:67例均得到随访,时间6-35个月。67例骨缺损得以重建,骨折愈合,但其中5例效果较差;44例软组织缺损病例中,40例创面闭合,4例创面未愈合。外固定后1,3,6个月及末次随访胫骨缺损长度和软组织缺损面积均较外固定前改善(P < 0.05);外固定后踝关节Kofoed评分及膝关节ROM均较外固定前改善(P < 0.05);末次随访时各种治疗方案疗效评价优良率为85%。对于合并皮肤缺损的胫骨骨髓炎性骨缺损,应用Ilizarov技术治疗胫骨骨缺损创伤小,能够避免多次复杂手术,缩短治疗时间和节省治疗费用,但也有一定的缺点和局限性。选用Ilizarov环形外固定架钢环的大小和材质对外固定效果和固定后调整均有一定影响。
中图分类号:
引用本文
余 凯,杨 晶,杨广忠,艾合买提江,陈柯屹,赵弟庆,袁春晓. Ilizarov牵拉架外固定治疗胫骨骨缺损的钢环参数选择[J]. 中国组织工程研究, 2014, 18(4): 577-582.
Yu Kai, Yang Jing, Yang Guang-zhong, AiHeMaiTiJiang, Chen Ke-yi, Zhao Di-qing, Yuan Chun-xiao. Parameter selection for steel ring of Ilizarov external fixation in the treatment of tibial bone defects[J]. Chinese Journal of Tissue Engineering Research, 2014, 18(4): 577-582.
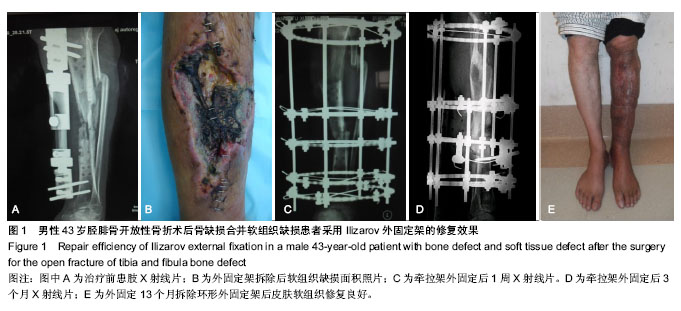
2.4 典型病例 男性患者,43岁,入院诊断为胫腓骨开放性骨折术后骨缺损合并软组织缺损,采用Ilizarov外固定架治疗,随访13个月,修复效果优,不良事件为患肢软组织瘢痕(图1)。
2.5 不良事件 随访期间患者均未发生移植物-宿主反应,4例通过游离皮片植皮成活,2例通过局部旋转皮瓣修复覆盖创面,4例未能愈合;治疗前足下垂11例经治疗末次随访功能改善8例;治疗前膝关节强直5例功能恢复均欠佳;治疗前14例合并其他部位损伤的患者损伤都得以控制及改善。
| [1] McKee MD, Yoo DJ, Zdero R, et al.Combined single-stage osseous and soft tissue reconstruction of the tibia with the Ilizarov method and tissue transfer.J Orthop Trauma. 2008; 22(3):183-189. [2] Wu CC.Single-stage surgical treatment of infected nonunion of the distal tibia. J Orthop Trauma. 2011;25(3):156-161.[3] Tuli SM.Tibialization of the fibula: a viable option to salvage limbs with extensive scarring and gap nonunions of the tibia.J Clin Orthop Relat Res. 2005;(431):80-84.[4] 纪红军,冯琼华.锁定加压钢板联合植骨治疗胫骨下段骨不连38例[J].临床骨科杂志,2011,14(6):718.[5] 朱雅龙,吴金平,王永安,等.锁定钢板治疗四肢长管状骨骨不连[J].临床骨科杂志,2011,14(6):720.[6] 秦泗河,李刚.Ilizarov理论与技术的起源、发展与传播史[J].中国骨与关节损伤杂志,2010,3(5):417-423.[7] 陈建文,秦泗河.Ilizarov技术临床应用的相关问题[J].中国骨与关节外科,2011,4(1):56-59.[8] Tripathy SK,Saini R,Sudes P,et al.Application of the Ponseti principle for deformitv correction in neglected and relapsed club foot using the Ilizarov fixator. J Pediatr Orthop B. 2011; 20(1):26-32.[9] 秦泗河,陈建文,郑学建,等.改良Ilizarov技术救治频临截肢的下肢残缺畸形[J].中国骨科杂志,2010,30(4):423-426.[10] 秦泗河. Ilizarov技术概述[J].中华骨科杂志,2006, 26(9): 642-645.[11] Fischgrund J, Paley D, Suter C. Variables affecting time to bone healing during limb lengthening. J Clin Orthop.1994; 301:31-37.[12] Ullmann Y,Fodor L,Soudry M,et al.The Ilizarov technique in joint contractures and dislocations. J Acta Orthop Belg. 2007;73(1):77-82.[13] Steinwender G,Saraph V,Zwick EB,et al.Complex footdeformities associated with soft-tissue scarring in children. J Foot Ankle Surg.2001;40(1):42-49.[14] Segev E,Wientroub S,Kollender Y,et al.A combined use of a free vascularised flap and an external fixator forreconstruction of lower extremity defects in children.J Orthop Surg(Hong Kong).2007;15(2):207-210.[15] Van Bosse HJ,Feldman DS,Anavian J,et al.Treatment of knee flexion contractures in patients with arthrogryposis.J Pediatr Orthop2007,27(8):930-937.[16] Carmichael KD,Maxwell SC,Calhoun JH.Recurrence rates of burn contracture ankle equinus and other foot deformities in children treated with Ilizarov fixation.J Pediatr Orthop.2005; 25(4):523-528.[17] Ferreira RC,Costa MT,Frizzo GG,et al.Correction of severe recurrent clubfoot using a simplified setting of the Ilizarov device. Foot Ankle Int. 2007;28(5):557-568.[18] Zhao ZY,Shao L,Zhao HM,et al. Osteogenic growth peptide aecelerates bon'e healing during distraction osteogenesis in rabbit tibia.J Int Med Res. 2011;39(2):456-463.[19] Spiro AS,Babin K,Lipovac S,et al. Combined treatment of congenital pseudarthrosis of the tibia,including recombinant human bone morphogenetie protein-2:a case series.J Bone Joint Surg. 2011;93(5):695-699.[20] Sashieh S,El Bitar Y,Berjawi G,et al.Distraction histogenesis in ankle burn deformities.J Bum Care Res. 2011;32(1): 160-165.[21] Lee DY, Choi IH, Yoo WJ, et al. Application of the Ilizarov technal to the correction of neurologic equinocavovams foot defor- mity. Clin Orthop Relat Res. 2011;469(3):860-867.[22] Desgrippes Y,Souchet P,Bensahel H.Use of the Ilizarov exter-nal fixator in multioperated,recurrent clubfoot. J Pediatr Orthop Part B. 1992;1(2):181. [23] Segev E, Ezra E, Yaniv M, et al. Vosteotomy and Ilizarov technique for residual idiopathic or neurogenic clubfeet.J Orthop Surg (Hong Kong). 2008;16(2):215-219.[24] Andersen LR, Johannsen HG, Ernst C, et al. Tibial pseudoarthrosis. Treatment using the Ilizarov technique. Ugeskr Laeger. 1996;157:2237-2240. [25] Dagher F, Roukoz S. Compound tibial fractures with bone loss treated by the Ilizarov technique. J Bone Joint Surg [Br]. 1991;73:316-321. [26] Dendrinos GK, Kontos S, Lyritsis E. Use of the Ilizarov technique for treatment of non-union of the tibia associated with infection. J Bone Joint Surg [Am]. 1995;77:835-846.[27] 李红宇,才志勇,李玉山,等.Ilizarov外固定架在胫骨截骨延长治疗中的应用[J].中国矫形外科杂志,2005,13(13):985-987.[28] Bradish CF,Noor S.The Ilizaror method in the management of relapsed club feet.J Bone Joint Surg Br. 2000;82(3):387-391.[29] Melvin JS,Dahners LE.A technique for correction of equinus contracture using a wire fixator and elastic tension.J Orthop Trauma. 2006;20(2):138-142.[30] Cierny G III, Zorn KE. Segmental tibial defects. Comparing conventional and Ilizarov methodologies. Clin Orthop. 1994; 301:118-123. [31] 艾合买提·玉素甫,陈统一,王晓峰,等.应用Ilizarov技术治疗长管状骨缺损性骨不连[J].中华骨科杂志,2006,26(4):247-251.[32] 方广文,吕廷灼,舒衡生,等.Ilizarov技术在治疗骨折并发症中的应用进展[J].中国矫形外科杂志,2010,18(10):825-827. [33] Green SA. A comparison of bone grafting and bone transport for segmental skeletal defects. Clin Orthop. 1994;301:111-117.[34] Brunner UH, Cordey J, Schweiberer L, et al. Force required for bone segment transport in the treatment of large bone defects using medullary nail fixation. Clin Orthop. 1994; 301:147-155. [35] Lovisetti G, Agus MA, Pace F, et al. Management of distal tibial intra-articular fractures with circular external fixation. Strategies Trauma Limb Reconstr. 2009;4(1):1-6.[36] Steinwender G, Saraph V, Zwick EB, et al.Complex foot defor. mities associated with soft-tissue scarring in children. J Foot An-kle Surg. 2001;40(1):42-49.[37] Gillooly JJ, Tilkeridis K, Simonis RB, et al.The treatment of high tibial osteoto- my non-union with the Ilizarov external fixator. Strategies Trauma Limb Reconstr. 2012;7(2):93-97.[38] Mccoy TH Jr, Kim HJ, Cross MB,et al.Bone tumor reconstruction with the Ilizarov method.J Surg Oncol. 2013; 107(4):343-352. |
| [1] | 陈子扬, 蒲 锐, 邓 爽, 袁凌燕. 外泌体对运动介导胰岛素抵抗类疾病的调控作用[J]. 中国组织工程研究, 2021, 25(25): 4089-4094. |
| [2] | 陈 扬, 黄邓高, 高元慧, 王顺兰, 曹 卉, 郑琳麟, 何浩伟, 罗思琴, 肖敬川, 张应爱, 张淑芳. 低强度脉冲场超声促进人脂肪间充质干细胞的增殖和黏附[J]. 中国组织工程研究, 2021, 25(25): 3949-3955. |
| [3] | 杨俊辉, 罗金莉, 袁小平. 人生长激素对人牙周膜干细胞增殖及成骨分化的影响[J]. 中国组织工程研究, 2021, 25(25): 3956-3961. |
| [4] | 孙建威, 杨新明, 张 瑛. 孟鲁司特联合骨髓间充质干细胞移植治疗脊髓损伤模型大鼠[J]. 中国组织工程研究, 2021, 25(25): 3962-3969. |
| [5] | 高 珊, 黄东静, 洪海漫, 贾京桥, 孟 斐. 人胎盘间充质干细胞及诱导的胰岛样细胞移植治疗妊娠期糖尿病大鼠效果比较#br#[J]. 中国组织工程研究, 2021, 25(25): 3981-3987. |
| [6] | 郝晓娜, 张英杰, 李玉云, 许 涛. 过表达脯氨酰寡肽酶的骨髓间充质干细胞修复肝纤维化模型大鼠[J]. 中国组织工程研究, 2021, 25(25): 3988-3993. |
| [7] | 刘建友, 贾中伟, 牛佳伟, 曹鑫杰, 张 栋, 魏 杰. 构建股骨3D数字化模型提出一种新的股骨颈前倾角测量方法[J]. 中国组织工程研究, 2021, 25(24): 3779-3783. |
| [8] | 孟令杰, 钱 辉, 盛晓磊, 陆剑锋, 黄建平, 祁连港, 刘宗宝. 3D打印建模联合骨水泥成形微创治疗塌陷Sanders Ⅲ型跟骨骨折[J]. 中国组织工程研究, 2021, 25(24): 3784-3789. |
| [9] | 钱选昆, 黄合飞, 武成聪, 刘克廷, 欧 华, 张金鹏, 任 静, 万建杉. 计算机导航微创经椎间孔腰椎椎间融合治疗腰椎滑脱[J]. 中国组织工程研究, 2021, 25(24): 3790-3795. |
| [10] | 胡 靖, 向 阳, 叶 川, 韩子冀. 3D打印辅助与徒手置钉经皮椎弓根钉内固定治疗胸腰椎骨折的1年随访[J]. 中国组织工程研究, 2021, 25(24): 3804-3809. |
| [11] | 舒启航, 廖亦佳, 薛静波, 晏怡果, 王 程. 新型颈椎3D打印多孔椎间融合器的三维有限元分析[J]. 中国组织工程研究, 2021, 25(24): 3810-3815. |
| [12] | 王一寒, 李 杨, 张 玲, 张 睿, 徐瑞达, 韩晓峰, 程光齐, 王伟力. 数字骨科三维可视化技术在股骨转子间骨折复位内固定中的应用[J]. 中国组织工程研究, 2021, 25(24): 3816-3820. |
| [13] | 孙玛骥, 王秋安, 张星晨, 郭 冲, 袁 峰, 郭开今. 新型颈椎前路经椎弓根固定钉板系统的研制及生物力学分析[J]. 中国组织工程研究, 2021, 25(24): 3821-3825. |
| [14] | 林 旺, 王盈盈, 郭卫中, 袁翠华, 许胜贵, 张申申, 林成寿. 胫骨平台后外侧柱骨折扩大外侧入路内固定增强力学稳定性及膝关节功能[J]. 中国组织工程研究, 2021, 25(24): 3826-3827. |
| [15] | 朱 云, 陈 渝, 邱 皓, 刘 盾, 靳国荣, 陈诗谋, 翁 政. 对侧皮质锁定螺钉治疗骨质疏松股骨骨折的有限元分析[J]. 中国组织工程研究, 2021, 25(24): 3832-3837. |
设计:回顾性病例分析。
统计学分析:由第一作者和统计教研室老师共同完成,采用SPSS 19.0统计软件进行分析。计量资料以x±s表示,不同时间段组间比较采用重复测量数据方差分析,两两比较采用配对t 检验。检验水准取α=0.05。
3.1 Ilizarov技术修复胫骨大段缺损合并软组织损伤 很多学者临床评价了应用Ilizarov技术治疗胫骨缺损的方法的优缺点[24-29],比较了Ilizarov技术与其他方案的特点[30-32],通过对Ilizarov技术的结果和并发症进行回顾性研究表明该方法治疗胫骨骨缺损是很有效的。本文中治疗后1,3,6个月及末次随访胫骨缺损长度较术前显著改善,其中50例骨折端Ⅰ期愈合,骨缺损得以重建。Green[33]报道了9例应用Ilizarov技术治疗胫骨缺陷,平均缺损6.3 cm。4例患者术前有感染,术后所有9例骨折均愈合无感染残留并且肢体不等长<1 cm,外固定指数为1.8 cm/月。其中Ilizarov组在手术时间、住院天数、下地行走时间、输血和辅助外科手术平均时间少,从而节省成本。Brunner[34]和Cierny等[30]对植骨和Ilizarov骨运输方法进行了比较,结果表明应用Ilizarov治疗骨缺损修复更快,更安全,更便宜。但基于治疗时间较长和患者心理创伤方面的考虑,Cierny建议对于骨缺损<6 cm时行一处截骨骨传输,骨缺损> 6 cm时行二处截骨骨传输治疗时间更短。目前采用胫骨干骺端截骨延长多采用一处截骨,骨延长时间较长,韩立仁等报道采用胫骨上下干骺端两处截骨延长治疗胫骨缺损临床效果较好。
高能量创伤引起的胫腓骨开放性骨折,治疗过程中常合并骨髓炎、骨缺损及软组织损伤,病情复杂、处理较为棘手。骨的解剖形态伴随其所受应力大小的改变而改变,应力能改变骨细胞的电生理化学环境,激发间质细胞潜在的成骨特性,使骨的沉积-吸收活动维持动态平衡而保持骨的基本形态结构稳定,坚强的刚性内固定其早期产生的应力遮挡作用可以很好的保护骨折断新生的血管和骨痂,依据Wolff定律,骨折愈合中后期需要稳定的应力改变,内固定物破坏了骨折愈合所需的压应力改变,导致骨折延迟愈合或不愈合。这是因为成骨活性的细胞未能获得有效的应力刺激而处于功能性休眠状态所导致的。可动力化的调整,既能视病情缩短对骨折端加压,又可牵引延长。通过模块转换动力化的调整环形外固定架,以使骨折由钢性固定转变为弹性固定,优化骨折愈合环境。Ilizarov环形外固定架较强的对抗垂直于胫骨的弯曲动力和剪切应力,通过三维空间固定和不同时间调整相结合,缓慢对患肢行四维畸形矫正和功能重建,在骨折愈合中后期则由高强度的刚性固定向弹性固定的转变,实现模块转化,使Ilizarov环形外固定架动力化,通过动力化调整优化了骨折愈合环境,不但可对固定结构行骨性重建、塑性和延长,还能对神经、血管和软组织进行重建和塑性,对胫骨骨髓炎合并骨缺损有显著的疗效。因此在选用Ilizarov环形外固定架钢环的大小和不同材质的钢环都对治疗效果和固定后的调整有一定影响。
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||