中国组织工程研究 ›› 2015, Vol. 19 ›› Issue (9): 1313-1320.doi: 10.3969/j.issn.2095-4344.2015.09.001
• 人工假体 artificial prosthesis • 下一篇
全膝关节置换修复膝内翻畸形:胫股角及膝关节活动度随访评价
李广伟,王红军,孙晓智,陈林斌,高宇亮,白忠旭,程新胜
- 郑州市第二人民医院骨二科,河南省郑州市 450000
-
修回日期:2014-12-09出版日期:2015-02-26发布日期:2015-02-26 -
作者简介:李广伟,男,1975年生,河南省郑州市人,汉族,1996年河南医科大学毕业,硕士,副主任医师,主要从事脊柱、关节外科的研究。
Total knee arthroplasty for knee varus deformity: follow-up evaluation of femorotibial angle and range of motion
Li Guang-wei, Wang Hong-jun, Sun Xiao-zhi, Chen Lin-bin, Gao Yu-liang, Bai Zhong-xu, Cheng Xin-sheng
- Second Department of Orthopedics, the Second People’s Hospital of Zhengzhou, Zhengzhou 450000, Henan Province, China
-
Revised:2014-12-09Online:2015-02-26Published:2015-02-26 -
About author:Li Guang-wei, Master, Associate chief physician, Second Department of Orthopedics, the Second People’s Hospital of Zhengzhou, Zhengzhou 450000, Henan Province, China
摘要:
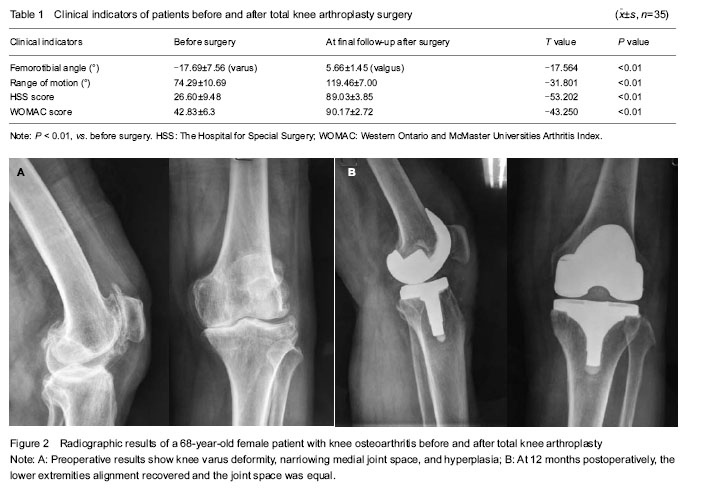
背景:膝关节内翻畸形施行人工全膝关节置换难度大,涉及面多,包括手术入路、术中截骨、软组织松解顺序、方法及程度、软组织平衡等,目前意见不统一,争议较多。 目的:观察全膝关节置换修复成人膝关节内翻畸形胫股角及膝关节活动度的1年以上随访结果。 方法:2006年6月至2013年6月对31例(35膝)膝内翻畸形采用后稳定型假体进行全膝关节置换,髌骨内侧入路,正确截骨,选择性软组织松解,以恢复膝关节正常力线和软组织平衡,获得膝关节的稳定,置换后采取针对性的康复训练。全膝关节置换前后拍X射线片测量胫股角,置换后定期随访检查膝关节活动度,并进行美国特种外科医院(HSS)评分、美国西部Ontario和McMaster大学骨关节炎指数(WOMAC)评估。 结果与结论:所有患者均获得随访,随访时间为12-96个月,随访方式为门诊复查随访。胫股角由置换前平均内翻17.69°(5°-30°)纠正至置换后的5.66°(2°-8°),膝关节活动度由置换前的74.29°(60°-95°)提高到置换后119.46° (105°-130°);HSS评分由置换前的26.60分(14-42分)提高到置换后89.03分(82-95分),优28膝,良7膝;WOMAC评分由42.83分(28-54分)提高到置换后90.17分(85-95分)。结果经统计学分析提示,所有病例置换后胫股角、膝关节活动度、HSS及WOMAC评分均较置换前显著改善(P < 0.01)。置换后X射线片检查未见假体周围透亮区,关节力线正常,无髌骨低位、髌骨骨折。提示成人膝关节内翻畸形患者全膝关节置换后1年以上随访畸形均得到纠正,功能明显改善,修复效果满意。
中图分类号:
引用本文
李广伟,王红军,孙晓智,陈林斌,高宇亮,白忠旭,程新胜. 全膝关节置换修复膝内翻畸形:胫股角及膝关节活动度随访评价[J]. 中国组织工程研究, 2015, 19(9): 1313-1320.
Li Guang-wei, Wang Hong-jun, Sun Xiao-zhi, Chen Lin-bin, Gao Yu-liang, Bai Zhong-xu, Cheng Xin-sheng. Total knee arthroplasty for knee varus deformity: follow-up evaluation of femorotibial angle and range of motion[J]. Chinese Journal of Tissue Engineering Research, 2015, 19(9): 1313-1320.
| [1] Li S, Chen Y, Su W, et al. Systematic review of patellar resurfacing in total knee arthroplasty. Int Orthop. 2011; 35(3): 305-316. [2] Radcliff KE, Orozco FR, Quinones D, et al. Preoperative risk stratification reduces the incidence of perioperative complications after total knee arthroplasty. J Arthroplasty. 2012;27(8 Suppl):77-80.e8. [3] Zietz C, Bergschmidt P, Fritsche A, et al. Comparison of cross-sections of different femoral components for revision total knee replacement. J Orthop Surg (Hong Kong). 2012;20(1):32-36. [4] Wang X, Weng X, Lin J, et al. Surgical technique and clinical results of total knee arthroplasty in treating endstage gonarthrosis combined with valgus knee deformity. Zhongguo Xiufu Chongjian Waike Zazhi. 2012;26(5): 513-517. [5] Robertsson O, Dunbar M, Pehrsson T, et al. Patient satisfaction after knee arthroplasty: a report on 27, 372 knees operated on between 1981 and 1995 in Sweden. Acta Orthop Scand. 2000;71(3):262-267. [6] Gao W, Chen BC, Duan JT, et al. The anatomic research on the rotation relationship among the proximal tibia, distal femur and patella. Zhonghua Guke Zazhi. 2005;25(11): 687-691. [7] Li BW. Biomechanical alterations in total knee arthroplasty. Zhongguo Zuzhi Gongcheng Yanjiu yu Linchuang Kangfu. 2008;12(17):3313-3316. [8] Zhou YX. Effect of artificial knee joint prosthesis design on patellofemoral joint function after total knee arthroplasty. Zhonghua Guke Zazhi. 2006;26(9):646-648. [9] Wang Y, Zhou YG, Wang JF, et al. Preliminary clinical outcome of mobile-bearing knee replacement. Zhonghua Guke Zazhi. 2002;22(5):276-279. [10] Kim YH, Yoon SH, Kim JS. Early outcome of TKA with a medial pivot fixed-bearing prosthesis is worse than with a PFC mobile-bearing prosthesis. Clin Orthop Relat Res. 2009;467(2):493-503. [11] Wyss T, Schuster AJ, Christen B, et al. Tension controlled ligament balanced total knee arthroplasty: 5-year results of a soft tissue orientated surgical technique. Arch Orthop Trauma Surg. 2008;128(2):129-135. [12] Lädermann A, Saudan M, Riand N, et al. Fixed-bearing versus mobile-bearing total knee arthroplasty: a prospective randomize clinical and radiological study. Rev Chir Orthop Reparatrice Appar Mot. 2008;94(3):247-251. [13] Karachalios TH, Sarangi PP, Newman JH. Severe varus and valgus deformities treated by total knee arthroplasty. J Bone Joint Surg. 1994;76B:938-942. [14] Zhou DG, Lv HS, Du XK. Lower Extremity Alignment Analysis of Varus Knee with X-ray Image. Zhongguo Yixue Yingxiang Jishu. 2001;17(12):1222-1224. [15] Pan WJ, Jing K, He Y. Early clinical outcome of total knee arthroplasty for patients with knee of varus deformity and flexion contracture. Zhongguo Guyuguanjie Sunshang Zazhi. 2011;26(7):595-597. [16] Havet E, Gabrion A, Leiber-Wackenheim F, et al. Radiological study of the knee joint line position measured from the fibular head and proximal tibial landmarks. Surg Radiol Anat. 2007;29(4):285-289. [17] Hao SC, Jiang JN, Wang Y, et al. Effect of treatment of posterior stabilized total knee arthroplasty. Zhongguo Guyuguanjie Sunshang Zazhi. 2011;26(7):622-623. [18] Liu PF, Guo L, Tian FD, et al. Clinical analysis of total knee arthroplasty therapy for unilateral knee varus combined with flexion contracture deformity. Zhongguo Guyuguanjie Sunshang Zazhi. 2013;28(2):119-121. [19] Feng CL, Li ZS, Li AY, et al. Clinical research of total knee arthroplasty for patients with knee of varus deformity. Chongqing Yixue. 2013;42(11):1229-1230. [20] Lv HS, Yuan YL, Kou BL, et al. Clinic analysis of 1336 total knee arthroplasty. Beijing Daxue Xuebao (Yixueban). 2002; 34(5):618-622. [21] Li J, Zheng K, Hu PX, et al. Comparison of short-term result between high-flex and conventional posterior stabilized prosthesis in total knee arthroplasty. Zhongguo Xiufu Chongjian Waike Zazhi. 2010;24(3):278-281. [22] Kim YH, Sohn KS, Kim JS. Range of motion of standard and high flexion posterior stabilized total knee prosthese. A prospective, randomized study. J Bone Joint Surg (Am). 2005;87(7):1470-1475. [23] McCalden RW, MacDonald SJ, Bourne RB, et al. A randomized controlled trial comparing “high-flex” vs “standard” posterior cruciate substituting polyethylene tibial inserts in total knee arthroplasty. J Arthroplasty. 2009; 24(6 Suppl):33-38. [24] Bao YJ, Dong JY, Xu DL. Application of fixed-bearing knee joint prosthesis in treatment of varus deformity in elderly osteoarthritis patients. Jiefangjun Yixueyuan Xuebao. 2013; 34(5):484-491. [25] Yamazaki J, Ishigami S, Nakmura T, et al. Hy-Flex II total knee system and range of motion. Arch Orthop Trauma Surg. 2002;122(3):156-160. [26] Hsu RW. The management of the patella in total knee arthroplasty. Chang Gung Med J. 2006;29(5):448-457. [27] Zhang X, Wang ZW. Patella treatment in total knee arthroplasty. Zhongguo Zuzhi Gongcheng Yanjiu yu Linchuang Kangfu. 2011;15(13):2421-2424. [28] Zou YG, Chen ZW, Feng ZQ, et al. Factors related to anterior knee pain after total knee arthroplasty. Nanfang Yike Daxue Xuebao. 2011;31(8):1428-1430. [29] Raviraj A, Prabhu A, Pai S, et al. Fixed vs mobile-bearing total knee arthroplasty: does it make a difference?--a prospective randomized study. J Arthroplasty. 2010;25(5): 835. [30] Chai W, Sun CJ, Ni M, et al. Case-control study on earlier medial tibial pain after total knee arthroplasty. Zhongguo Gushang. 2014;27(4):269-273. |
| [1] | 王金军, 邓增发, 刘 康, 何智勇, 余新平, 梁建基, 李 晨, 郭洲洋. 全膝关节置换静脉滴注氨甲环酸联合含氨甲环酸鸡尾酒局部应用的止血效果及安全性[J]. 中国组织工程研究, 2021, 25(9): 1356-1361. |
| [2] | 陈俊名, 岳 辰, 何沛霖, 张俊涛, 孙墨渊, 刘又文. 髋关节置换与股骨近端防旋髓内钉内固定修复高龄股骨转子间骨折效果的Meta分析[J]. 中国组织工程研究, 2021, 25(9): 1452-1457. |
| [3] | 刘正蓬, 王雅辉, 张义龙, 明 颖, 孙志杰, 孙 贺. 3D打印椎间融合器置入治疗脊髓型颈椎病:颈椎曲度及椎间高度恢复的半年随访[J]. 中国组织工程研究, 2021, 25(6): 849-853. |
| [4] | 赵中溢, 李勇阵, 陈 峰, 季爱玉. 同期双侧全膝关节置换和单髁置换治疗创伤性关节炎的比较[J]. 中国组织工程研究, 2021, 25(6): 854-859. |
| [5] | 袁 俊, 杨家福. 局部氨甲环酸浸润在非骨水泥全膝关节置换过程中止血效果的评价[J]. 中国组织工程研究, 2021, 25(6): 873-877. |
| [6] | 吴 刚, 陈建文, 王世隆, 段笑然, 刘海军, 董建峰. 单纯HyProCure跗骨螺钉治疗青少年柔韧性平足合并痛性副舟骨[J]. 中国组织工程研究, 2021, 25(6): 901-905. |
| [7] | 孔令宝, 吕 欣. 胫骨后外侧平台骨折手术治疗中植入物选择与入路对支撑作用的影响[J]. 中国组织工程研究, 2021, 25(6): 942-947. |
| [8] | 李兴平, 肖东琴, 赵 桥, 陈 硕, 白亦光, 刘 康, 冯 刚, 段 可. 钛表面载铜抗菌功能膜的制备及性能[J]. 中国组织工程研究, 2021, 25(4): 553-557. |
| [9] | 吕家兴, 白磊鹏, 杨朝昕, 苗岳松, 金 宇, 李哲宏, 孙广普, 徐 莹, 张擎柱. 膝关节骨性关节炎老年股骨转子间骨折行股骨近端防旋髓内钉内固定评价[J]. 中国组织工程研究, 2021, 25(3): 391-396. |
| [10] | 刘 畅, 韩树峰. 股骨近端联合拉力交锁髓内钉与股骨近端防旋髓内钉、亚洲型股骨近端防旋髓内钉内固定治疗老年转子间骨折的Meta分析[J]. 中国组织工程研究, 2021, 25(3): 477-485. |
| [11] | 吕泽祥, 吴居泰, 蒋 健, 冯 骁, 李腾飞, 王业华. 氨甲环酸联合卡络磺钠干预全膝关节置换的失血及安全性[J]. 中国组织工程研究, 2021, 25(3): 386-390. |
| [12] | 张德刚, 刘 栋, 李 朋, 王兆林, 张 锴, 张新军. 弹性髓内钉与钢板置入治疗移位锁骨中段B型骨折的短期随访[J]. 中国组织工程研究, 2021, 25(24): 3860-3864. |
| [13] | 邹守平, 卢道云, 叶 力. 微创经皮伤椎置钉治疗胸腰椎骨折:6个月随访脊柱生物力学变化[J]. 中国组织工程研究, 2021, 25(24): 3865-3869. |
| [14] | 张振华, 刘姿辰, 禹宝庆. 聚己内酯及其复合材料在组织工程骨构建中的地位与问题[J]. 中国组织工程研究, 2021, 25(22): 3571-3577. |
| [15] | 闻志靖, 顾鹏真, 贺西京, 李家良, 王一斌, 王逸群. 高分子聚合物聚醚酮酮的发展及其医学应用前景[J]. 中国组织工程研究, 2021, 25(22): 3603-3608. |
After femoral nerve was blocked before surgery, patients were fixed in the supine position under epidural anesthesia, pneumatic tourniquet at the pressure of 300 mm Hg (1 mm Hg = 0.133 kPa) was applied to stop bleeding. All knee joints were inserted through the medial parapatellar approach in anterior knee medial incision, the incision was cut along the medial patella to the medial tibial tubercle, exposing the knee joints, then infrapatellar fat pad was completely resected, the suprapatellar bursa and intra-articular synovial membrane were removed. The medial tibia was released and osteophytes were excised to reduce the patellar tendon tension, then the patella was everted. In the valgus process, patellar ligament tension at the tibial insertion point should be controlled, avoiding patellar rupture or avulsion caused by violence. Subsequently, femoral condyle and osteophytes at tibial articular surface were bited, releasing the medial collateral ligament; after anterior and posterior cruciate ligaments were resected, the medial articular capsule and the reflected head of semitendinosus and semimembranosus were released, pes anserinus tendon was cut if necessary and released under the periosteum. Intramedullary positioning was located in the area lateral to the insertion point of anterior cruciate ligament, in femoral intercondylar notch, at the valgus angle of 6°-7° (vertical to the mechanical axis of the femur). According to preoperative X-ray measurements, anterior and posterior femoral condyle, as well as distal femoral bone, were amputated 0.8-1.0 cm, in 3° extorsion. Extramedullary positioning was located in 0°-3° retroversion, followed by the osteotomy. The center axis of the femur and the tibia was taken as a reference of all surgeries, while normal side of joint deformity was used as the reference of positioning the prosthesis, the osteotomy was performed 0.6-1.0 cm below the lowest site of the plateau. After the meniscus, anterior and posterior cruciate ligaments were cut, the femur and the tibia were subjected to the osteotomy, which was performed in strict accordance with the mold guidance. Knee joints were straightened and the prosthesis model was inserted, the prosthesis activity and the collateral ligament balance were detected under the extension and flexion conditions. After replacement, the prosthesis activity should allow a 3°-5° hyperextension. The TKA surgery was not performed in patellar bone. The patellar osteophytes were bited and the patellar articular surface was trimmed, eliminating the spalling and exfoliative cartilage, so the patellar size was reduced and close to normal articular surface, good patellofemoral track can be obtained after denervation. Tourniquet was released and wounds were repeatedly rinsed, articular capsule was sutured in the flexion position and soft tissue was also sutured (Figure 1).
.jpg)
Statistical analysis was performed using SPSS 19.0 software. Data were expressed as the mean±SD. The difference before and after TKA surgery was compared using the t-test. A P < 0.05 was considered statistically significant.
1 文章选择首次膝关节置换的膝内翻畸形患者为观察对象,同时为避免内植物材料的影响,均选择后稳定型假体,避免过多外在及客观因素的干扰。 2 全膝关节置换术中发现部分患者通过针对性清除股骨远端、胫骨近端的内侧增生骨赘并初步截骨后,内翻畸形纠正,关节间隙平衡,可不做软组织松解,并且只有切除骨赘,才能真正松解内侧副韧带, 达到软组织平衡,再根据屈伸位内侧稳定结构不同功能决定膝内翻畸形的软组织松解顺序,从而获得不同状态下良好的软组织平衡。 3 针对国人髌骨特点选择保留并作修整及去神经化处理,有效减轻了患者的髌股关节疼痛,近远期效果满意。
只有真正匹配的假体才能根本上提高国人全膝置换的优良率,获得膝关节相关大样本解剖数据是改进假体设计及操作技术的关键。所以必须重视中国人与欧美人膝关节形态的差异,包括国人性别间的差异,这种差异不仅仅是简单的尺寸大小问题,而是形状不同的问题。高质量的假体和精确配套手术器械的国产化, 是推动国内膝关节置换普及和发展的关键。目前有根据国人喜欢蹲坐的特点开发了高屈曲度假体。理论上,该假体除能增加关节活动度外,还能减少膝前痛的发生率,降低聚乙烯衬垫的磨损,但与后稳定假体比较,置换术后膝关节最大屈曲度及膝关节活动度与后稳定性假体相比无明显优势,与Kim等的研究一致,表明高屈曲度假体在改善术后关节屈曲度的不确定性,会产生持续的不良应力逐渐导致软组织再次失去平衡,严重影响术后膝关节的后期稳定。因此,有学者认为高屈曲度假体仅适于术前膝关节活动度良好的患者。
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||