[1] ENDELE D, JUNG C, BECKER U, et al. Anterior cruciate ligament reconstruction with and without computer navigation: a clinical and magnetic resonance imaging evaluation 2 years after surgery. Arthroscopy. 2009;25(10): 1067-1074.
[2] BUSS DD, WARREN RF, WICKIEWICZ TL, et al. Arthroscopically assisted reconstruction of the anterior cruciate ligament with use of autogenous patellar-ligament grafts. Results after twenty-four to forty-two months. J Bone Joint Surg Am. 1993; 75(9): 1346-1355.
[3] WIGER P, BRANDSSON S, KARTUS J, et al. A comparison of results after arthroscopic anterior cruciate ligament reconstruction in female and male competitive athletes. A two- to five-year follow-up of 429 patients. Scand J Med Sci Sports. 1999; 9(5): 290-295.
[4] ABEBE ES, UTTURKAR GM, TAYLOR DC, et al. The effects of femoral graft placement on in vivo knee kinematics after anterior cruciate ligament reconstruction. J Biomech. 2011; 44(5): 924-929.
[5] ZANTOP T, DIERMANN N, SCHUMACHER T, et al. Anatomical and nonanatomical double-bundle anterior cruciate ligament reconstruction: importance of femoral tunnel location on knee kinematics. Am J Sports Med. 2008; 36(4): 678-685.
[6] KYUNG BS, KIM JG, CHANG M, et al. Anatomic double-bundle reconstruction techniques result in graft obliquities that closely mimic the native anterior cruciate ligament anatomy. Am J Sports Med. 2013; 41(6): 1302-1309.
[7] BEDI A, ALTCHEK DW. The "footprint" anterior cruciate ligament technique: an anatomic approach to anterior cruciate ligament reconstruction. Arthroscopy. 2009; 25(10): 1128-1138.
[8] KAWAKAMI Y, HIRANAKA T, MATSUMOTO T, et al. The accuracy of bone tunnel position using fluoroscopic-based navigation system in anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2012; 20(8): 1503-1510.
[9] TENSHO K, KODAIRA H, YASUDA G, et al. Anatomic double-bundle anterior cruciate ligament reconstruction, using CT-based navigation and fiducial markers. Knee Surg Sports Traumatol Arthrosc. 2011; 19(3): 378-383.
[10] COLOMBET PD, ROBINSON JR. Computer-assisted, anatomic, double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2008; 24(10): 1152-1160.
[11] FERRETTI A, MONACO E, LABIANCA L, et al. Double-bundle anterior cruciate ligament reconstruction: a computer-assisted orthopaedic surgery study. Am J Sports Med. 2008; 36(4):760-766.
[12] CHO WJ, KIM JM, KIM DE, et al. Accuracy of the femoral tunnel position in robot-assisted anterior cruciate ligament reconstruction using a magnetic resonance imaging-based navigation system: A preliminary report. Int J Med Robot. 2018; 14(5): e1933.
[13] FORSYTHE B, COLLINS MJ, ARNS TA, et al. Optimization of anteromedial portal femoral tunnel drilling with flexible and straight reamers in anterior cruciate ligament reconstruction: a cadaveric 3-dimensional computed tomography analysis. Arthroscopy. 2017; 33(5):1036-1043.
[14] MEUFFELS DE, REIJMAN M, VERHAAR JA. Computer-assisted surgery is not more accurate or precise than conventional arthroscopic ACL reconstruction: a prospective randomized clinical trial. J Bone Joint Surg Am. 2012; 94(17):1538-1545.
[15] EGGERDING V, REIJMAN M, SCHOLTEN RJ, et al. Computer-assisted surgery for knee ligament reconstruction. Cochrane Database Syst Rev. 2014;(9):CD007601.
[16] AHN JH, YANG HS, JEONG WK, et al. Arthroscopic transtibial posterior cruciate ligament reconstruction with preservation of posterior cruciate ligament fibers: clinical results of minimum 2-year follow-up. Am J Sports Med. 2006; 34(2): 194-204.
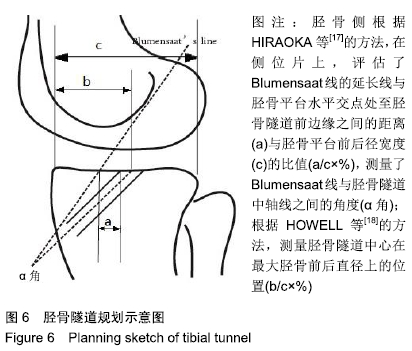
[17] HIRAOKA H, KURIBAYASHI S, FUKUDA A, et al. Endoscopic anterior cruciate ligament reconstruction using a computer-assisted fluoroscopic navigation system. J Orthop Sci. 2006;11(2): 159-166.
[18] HOWELL SM, TAYLOR MA. Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof. J Bone Joint Surg Am. 1993; 75(7): 1044-1055.
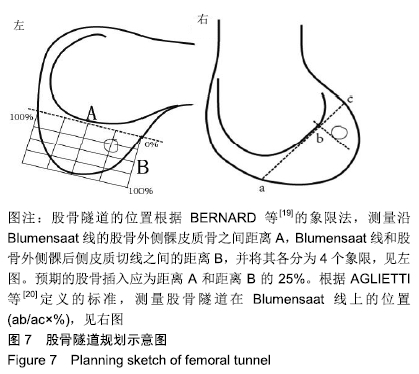
[19] BERNARD M, HERTEL P, HORNUNG H, et al. Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg. 1997; 10(1): 14-21; discussion 212-212.
[20] AGLIETTI P, BUZZI R, MENCHETTI PM, et al. Arthroscopically assisted semitendinosus and gracilis tendon graft in reconstruction for acute anterior cruciate ligament injuries in athletes. Am J Sports Med.1996;24(6):726-731.
[21] FU FH, MUSAHL V. Review Article: The future of knee ligament surgery. J Orthop Surg (Hong Kong). 2001;9(2): 77-80.
[22] GETELMAN MH, FRIEDMAN MJ. Revision anterior cruciate ligament reconstruction surgery. J Am Acad Orthop Surg. 1999;(3):189-198.
[23] JALLIARD R, LAVALLEE S, DESSENNE V. Computer assisted reconstruction of the anterior cruciate ligament. Clin Orthop Relat Res.1998;(354):57-64.
[24] JAGODZINSKI M, RICHTER GM, PASSLER HH. Biomechanical analysis of knee hyperextension and of the impingement of the anterior cruciate ligament: a cinematographic MRI study with impact on tibial tunnel positioning in anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2000; 8(1): 11-19.
[25] FUSS FK. The restraining function of the cruciate ligaments on hyperextension and hyperflexion of the human knee joint. Anat Rec.1991;230(2):283-289.
[26] CHENG T, ZHANG GY, ZHANG XL. Does computer navigation system really improve early clinical outcomes after anterior cruciate ligament reconstruction? A meta-analysis and systematic review of randomized controlled trials. Knee. 2012; 19(2): 73-77.
[27] PLAWESKI S, ROSSI J, MERLOZ P, et al. Analysis of anatomic positioning in computer-assisted and conventional anterior cruciate ligament reconstruction. Orthop Traumatol Surg Res. 2011;97(6 Suppl): S80-85.
[28] YOON KH, KIM JS, KIM SJ, et al. Eight-year results of transtibial nonanatomic single-bundle versus double-bundle anterior cruciate ligament reconstruction: Clinical, radiologic outcomes and survivorship. J Orthop Surg (Hong Kong). 2019; 27(2): 2309499019840827.
[29] VOLPI P, QUAGLIA A, CARIMATI G, et al. Double bundle anterior cruciate ligament reconstruction: Failure rate and patients-reported outcomes at 4-11 years of follow up. J Orthop. 2019;16(3): 224-229.
[30] LI Y J, ZHANG MC, LIU M, et al. [Femoral tunnel positioning in posterior cruciate ligament double-bundle reconstruction by computer aided design]. Zhongguo Gu Shang. 2015; 28(2): 162-167.
[31] COLOMBET P, ROBINSON J, CHRISTEL P, et al. Using navigation to measure rotation kinematics during ACL reconstruction. Clin Orthop Relat Res. 2007;454: 59-65.
[32] ZANTOP T, HERBORT M, RASCHKE MJ, et al. The role of the anteromedial and posterolateral bundles of the anterior cruciate ligament in anterior tibial translation and internal rotation. Am J Sports Med. 2007;35(2): 223-227.
|