• 脊柱植入物 spinal implant • 上一篇 下一篇
应用多聚醚酮椎间融合器修复Ⅱ型及Ⅱa型Hangman骨折:6个月随访评价
黄阳亮1,钟 祎2,刘少喻1
- 1中山大学附属第一医院脊柱外科,广东省广州市 510700;2广州医科大学生理学教研室,广东省广州市 510000
-
出版日期:2015-09-24发布日期:2015-09-24 -
通讯作者:黄阳亮,中山大学附属第一医院脊柱外科,广东省广州市 510700 -
作者简介:黄阳亮,男,1982年生,湖南省湘潭市人,汉族, 2008年中山大学毕业,硕士,主治医师,主要从事脊柱外科临床、教学与科研工作。
Polyetheretherketone cage for treating type II and type IIa Hangman’s fractures: 6-month follow-up
Huang Yang-liang1, Zhong Yi2, Liu Shao-yu1
- 1Department of Spine Surgery, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou 510700, Guangdong Province, China
2Department of Physiology, Guangzhou Medical University, Guangzhou 510000, Guangdong Province, China
-
Online:2015-09-24Published:2015-09-24 -
Contact:Huang Yang-liang, Department of Spine Surgery, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou 510700, Guangdong Province, China -
About author:Huang Yang-liang, Master, Attending physician, Department of Spine Surgery, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou 510700, Guangdong Province, China
摘要:
背景:Hangman骨折即创伤性枢椎滑脱,不稳定Hangman骨折的Ⅱ型、Ⅱa型及ⅡI型骨折需要手术治疗。咽后入路是上颈椎前路手术显露的常用手段。然而,重要结构周围的牵拉与分离使得手术程序复杂,增加了神经损伤的发生率。 目的:评价创新性应用多聚醚酮椎间融合器治疗Hangman骨折的临床疗效及安全性。 方法:收集Ⅱ型及Ⅱa型Hangman骨折患者8例,均进行C2/3椎间融合。术后随访进行X射线检查,评价融合时间及内植物位置。比较术前与术后6个月骨折处成角及移位数据和复位情况,以颈椎创伤后评分评价功能恢复,以目测类比评分评价颈部疼痛。 结果与结论:所有8例患者均得以成功随访,平均随访13个月(6-26个月)。与术前相比,术后6个月患者颈椎创伤后评分增高,目测类比评分及成角畸形和移位均降低(P < 0.05)。全部患者末次随访未见颈部活动受限,术后3或6个月所有患者椎间均骨性融合,无相关并发症。结果证实,应用多聚醚酮椎间融合器治疗Ⅱ型及Ⅱa型Hangman骨折临床疗效及安全性均较好。
中国组织工程研究杂志出版内容重点:人工关节;骨植入物;脊柱;骨折;内固定;数字化骨科;组织工程
中图分类号:
引用本文
黄阳亮,钟 祎,刘少喻. 应用多聚醚酮椎间融合器修复Ⅱ型及Ⅱa型Hangman骨折:6个月随访评价[J]. 中国组织工程研究, doi: 10.3969/j.issn.2095-4344.2015.39.013.
Huang Yang-liang, Zhong Yi, Liu Shao-yu. Polyetheretherketone cage for treating type II and type IIa Hangman’s fractures: 6-month follow-up[J]. Chinese Journal of Tissue Engineering Research, doi: 10.3969/j.issn.2095-4344.2015.39.013.
Eight patients were collected at the beginning, and they were all successfully follow-up for 6 months or longer. None of them was lost, so their data were put into final statistical analysis.
Clinical results
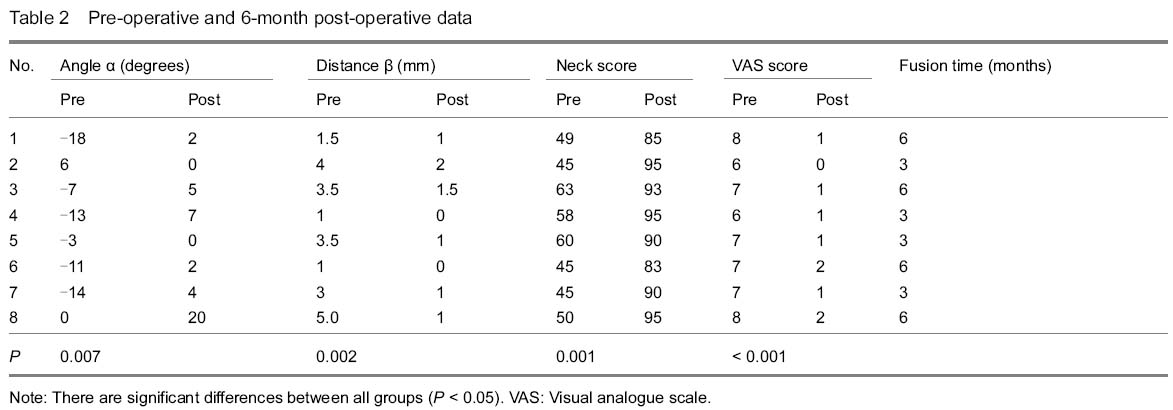
The mean operative time was 97.0±21.4 minutes (range 70-135) and the mean hemorrhage amount was 31±10.5 mL (range 20-50). We did not observe transient or permanent hoarseness, dysphagia and dysphonia. By Smith and Robinson approach, lower part of axis body could be exposed without difficulty in all of our patients. There were no further operations. Of the total 8 consecutive patients, follow-up evaluation data of 6 months or longer were available for all patients at a mean clinical follow-up of 13.0±6.21 months (range 6-26). The Clinical Post-Traumatic Neck Score (Mayo) was 51.88±7.38 (range 45-63) pre-operatively and 90.75±4.68 (range 83-95) at 6-month follow-up. There was a significant improvement (P=0.001). The pre-operative VAS scale score was 7.00±0.76 (range 6-8) and 6-month post-operative score was 1.13±0.64 (range 0-2). There was a significant difference between pre and post-operative results (P < 0.001) (Table 2). In our 6-month post-operative questionnaires of Neck Score, no patients complained of cervical movement limitation that disturbed daily activities; and cervical pain was relieved, no further oral analgesics were needed. On last follow-up, there was no cervical pain recorded either.
Radiographic results
Cervical radiograph examinations performed at the last follow-up visits showed no subsidence, collapse, breaking, or pseudarthrosis at the level of the implants. There was no bone material absorption or necrosis at the contiguous vertebral bodies, and no noticeable inflammatory reaction. There were no lucency gaps between fracture lines. Fusion was observed after 3 or 6 months in all of our patients.
The mean of angle deformity (α) pre-operatively was -7.50±8.05, and 6-month post-operatively was 5.00±6.52; the difference was significant (P=0.007). The mean of displacement distance (β) pre-operatively was 2.81±1.49, and 6-month post-operatively was 0.94±0.68, which was significant either (P=0.002) (Table 2).
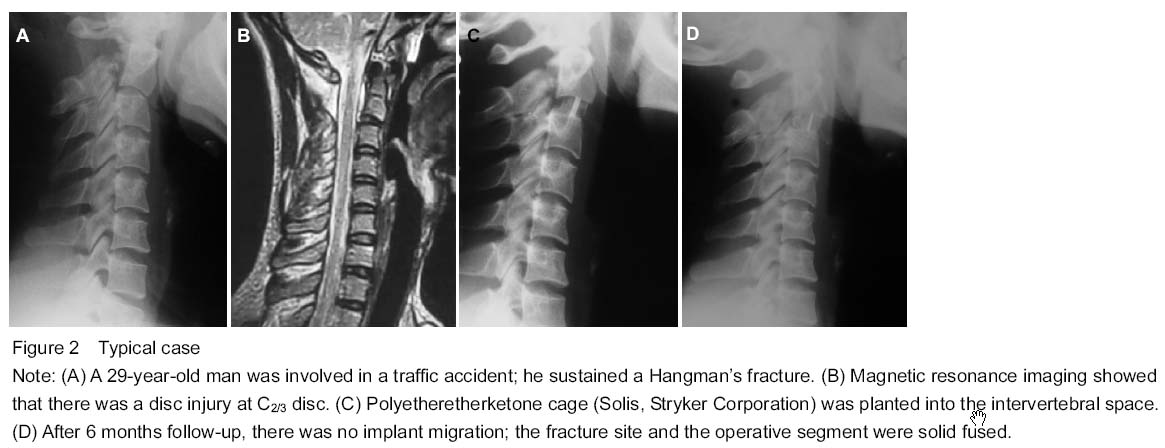
Typical case
A traffic accident caused a 29-year-old man a hangman’s fracture, his C2/3 disc and upper cervical ligaments were injured at the same time. He received solis fixation and reported a satisfied clinical outcome 6 months later (Figure 2).
| [1] Müller EJ, Wick M, Muhr G. Traumatic spondylolisthesis of the axis: treatment rationale based on the stability of the different fracture types. Eur Spine J. 2000;9(5):123-128. [2] Ferro FP, Borgo GD, Letaif OB, et al. Traumatic spondylilisthesis of axis: epidemiology, management and outcome. Acta Ortop Bras. 2012;20(2):84-87. [3] Bransford RJ, Alton TB, Patel AR, et al. Upper cervical spine trauma. J Am Acad Orthop Surg. 2014;22(11):718-729. [4] Marcon RM, Cristante AF, Teixeira WJ, et al. Fractures of the cervical spine. Clinics (Sao Paulo). 2013;68(11):1455-1461. [5] Effendi B, Roy D, Cornish B, et al. Fractures of the ring of the axis: A classification based on the analysis of 131 cases. J Bone Joint Surg Br. 1981;63B(5):319-327. [6] Dalbayrak S, Yaman O. A coinsidence, a chance or a misfortune? Hangman's fracture. Neurol Neurochir Pol. 2014;48(4):305-307. [7] Levine AM, Edwards CC. The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am. 1985;67(7):217-226. [8] Verheggen R, Jansen J. Hangman's Fracture: arguments in favor of surgical therapy for Type Ⅱand Ⅲ according to Edwards and Levine. Surg Neurol. 1998;49(5):253-262. [9] White AA, Panjabi MM. Clinical biomechanics of the spine. Lippincott, Philadephia, USA. 1978. [10] Li Z, Li F, Hou S, et al. Anterior discectomy/corpectomy and fusion with internal fixation for the treatment of unstable hangman's fractures: a retrospective study of 38 cases. J Neurosurg Spine. 2015;22(4):389-393. [11] Singh PK, Garg K, Sawarkar D, et al. Computed tomography-guided C2 pedicle screw placement for treatment of unstable hangman fractures. Spine (Phila Pa 1976). 2014;39(18):E1058-E1065. [12] Chowdhury FH, Haque MR. C1-C3 Lateral Mass Screw-Rod Fixation and Fusion for C2 Pathologies and Hangman's Fractures. Asian Spine J. 2014;8(6):735-746. [13] Jeong DH, You NK, Lee CK, et al. Posterior C2-C3 Fixation for Unstable Hangman's Fracture. Korean J Spine. 2013; 10(3): 165-169. [14] McAfee PC, Bohlman HH, Riley LH, et al. The anterior retropharyngeal approach to the upper part of the cervical spine. J Bone Joint Surg. 1987;69(6):1371-1383. [15] Park SH, Sung JK, Lee SH, et al. High anterior cervical approach to the upper cervical spine. Surg Neurol. 2007; 68(1):519-524. [16] Hur H, Lee JK, Jang JW, et al. Is it feasible to treat unstable hangman's fracture via the primary standard anterior retropharyngeal approach? Eur Spine J. 2014;23(8): 1641-1647. [17] Wison AJ, Marshall RW, Ewart M. Transoral fusion with internal fixation in a displaced hangman’s fracture. Spine. 1999;24(4):295-298. [18] Lin CN, Wu YC, Wang NP, et al. Preliminary experience with anterior interbody titanium cage fusion for treatment of cervical disc disease. Kaohsiung J Med Sci. 2003;19(4): 208-216. [19] McGrory BJ, Klassen RA. Arthrodesis of the cervical spine for fractures and dislocations in children and adolescents. A long-term follow-up study. J Bone Joint Surg Am. 1994; 76(10):1606-1616. [20] Truumees E, Demetropoulos CK, Yang KH, et al. Effects of disc height and distractive forces on graft compression in an anterior cervical discectomy model. Spine. 2002;33(9): 2441-2445. [21] Mastronardi L, Ducati A, Ferrante L. Anterior cervical fusion with polyetheretherketone (PEEK) cages in the treatment of degenerative disc disease, Preliminary observations in 36 consecutive cases with a minimum 12-month follow-up. Acta Neurochir (Wien). 2006.148(9):307-312. [22] Junaid M, Kalsoom A, Khalid M, et al. Cervical disc replacement with polyetheretherketone cages: clinical experience with 151 cases. J Ayub Med Coll Abbottabad. 2014;26(4):444-447. [23] Cho DY, Liau WR, Lee WY, et al. Preliminary experience using a polyetheretherketone (PEEK) cage in the treatment of cervical disc disease. Neurosurgery. 2002;51(3): 1343-1350. [24] Kim CH, Chung CK, Jahng TA, et al. Segmental kyphosis after cervical interbody fusion with stand-alone polyetheretherketone (PEEK) cages: a comparative study on 2 different PEEK cages. J Spinal Disord Tech. 2015; 28(1):E17-E24. [25] Li XF, Dai LY, Lu H, et al. A systematic review of the management of hangman’s fracture. Eur Spine J. 2006; 15(2):257-269. [26] Shin JJ, Kim SH, Cho YE, et al. Primary surgical management by reduction and fixation of unstable hangman's fractures with discoligamentous instability or combined fractures: clinical article. J Neurosurg Spine. 2013;19(5):569-575. [27] Watanabe M, Nomura T, Toh E, et al. Residual neck pain after traumatic spondylolisthesis of the axis. J Spinal Disord Tech. 2005;18(6):148-151. [28] Schofferman J, Garges K,Goldthwaite N, et al. Upper cervical anterior diskectomy and fusion improves discogenic cervical headaches. Spine. 2002;27(4): 2240-2244. [29] Heiko K, Anton K. Letter to the Editor concerning: A systematic review of the management of hangman’s fracture. Eur Spine J. 2006;15(2):1415-1418. [30] Lewkonia P, Dipaola C, Schouten R, et al. An evidence-based medicine process to determine outcomes after cervical spine trauma: what surgeons should be telling their patients. Spine (Phila Pa 1976). 2012;37(18):E1140- E1147. [31] Muthukumar N. C1-C3 lateral mass fusion for type Ⅱa and typeⅡI Hangman's fracture. J Craniovertebr Junction Spine. 2012;3(2):62-66. |
| [1] | 张同同, 王中华, 文 杰, 宋玉鑫, 刘 林. 3D打印模型在颈椎肿瘤手术切除与重建中的应用[J]. 中国组织工程研究, 2021, 25(9): 1335-1339. |
| [2] | 姚汝斌, 王仕永, 杨开舜. 微创经椎间孔椎间融合治疗单节段腰椎管狭窄症对腰椎-骨盆平衡的改善作用[J]. 中国组织工程研究, 2021, 25(9): 1387-1392. |
| [3] | 梁 彦, 赵永飞, 徐 帅, 朱震奇, 王凯丰, 刘海鹰, 毛克亚. 影像学评估高选择性神经根封闭辅助退行性脊柱侧凸短节段固定融合的效果[J]. 中国组织工程研究, 2021, 25(9): 1423-1427. |
| [4] | 侯广原, 张继学, 张志军, 孟祥晖, 段 文, 高维陆. 骨水泥强化椎弓根螺钉内固定治疗伴骨质疏松腰椎退行性疾病的1年随访[J]. 中国组织工程研究, 2021, 25(6): 878-883. |
| [5] | 吴 刚, 陈建文, 王世隆, 段笑然, 刘海军, 董建峰. 单纯HyProCure跗骨螺钉治疗青少年柔韧性平足合并痛性副舟骨[J]. 中国组织工程研究, 2021, 25(6): 901-905. |
| [6] | 孔令宝, 吕 欣. 胫骨后外侧平台骨折手术治疗中植入物选择与入路对支撑作用的影响[J]. 中国组织工程研究, 2021, 25(6): 942-947. |
| [7] | 占方彪, 程 军, 邹鑫森, 龙 杰, 谢鲤钟, 邓乾蓉. 术中静脉使用氨甲环酸减少多节段脊柱后路围术期出血的Meta分析[J]. 中国组织工程研究, 2021, 25(6): 977-984. |
| [8] | 刘正蓬, 王雅辉, 张义龙, 明 颖, 孙志杰, 孙 贺. 3D打印椎间融合器置入治疗脊髓型颈椎病:颈椎曲度及椎间高度恢复的半年随访[J]. 中国组织工程研究, 2021, 25(6): 849-853. |
| [9] | 罗选翔, 经 历, 潘 彬, 冯 虎. 甲钴胺联合鼠神经生长因子促进脊髓型颈椎病术后神经功能的恢复[J]. 中国组织工程研究, 2021, 25(5): 719-722. |
| [10] | 李兴平, 肖东琴, 赵 桥, 陈 硕, 白亦光, 刘 康, 冯 刚, 段 可. 钛表面载铜抗菌功能膜的制备及性能[J]. 中国组织工程研究, 2021, 25(4): 553-557. |
| [11] | 吕泽祥, 吴居泰, 蒋 健, 冯 骁, 李腾飞, 王业华. 氨甲环酸联合卡络磺钠干预全膝关节置换的失血及安全性[J]. 中国组织工程研究, 2021, 25(3): 386-390. |
| [12] | 吕家兴, 白磊鹏, 杨朝昕, 苗岳松, 金 宇, 李哲宏, 孙广普, 徐 莹, 张擎柱. 膝关节骨性关节炎老年股骨转子间骨折行股骨近端防旋髓内钉内固定评价[J]. 中国组织工程研究, 2021, 25(3): 391-396. |
| [13] | 梁 彦, 赵永飞, 朱震奇, 刘海鹰, 毛克亚. 微创经椎间孔腰椎椎体间融合固定治疗椎间盘源性脊柱侧凸:冠状面和矢状面平衡的2年随访[J]. 中国组织工程研究, 2021, 25(3): 409-413. |
| [14] | 刘 畅, 韩树峰. 股骨近端联合拉力交锁髓内钉与股骨近端防旋髓内钉、亚洲型股骨近端防旋髓内钉内固定治疗老年转子间骨折的Meta分析[J]. 中国组织工程研究, 2021, 25(3): 477-485. |
| [15] | 钱选昆, 黄合飞, 武成聪, 刘克廷, 欧 华, 张金鹏, 任 静, 万建杉. 计算机导航微创经椎间孔腰椎椎间融合治疗腰椎滑脱[J]. 中国组织工程研究, 2021, 25(24): 3790-3795. |
Surgical technique for Hangman’s fracture can mainly be divided into two categories: anterior or posterior. In anterior operations, C2/3 discectomy, autograft and plate fixation are the standard method[10]; on the other hand, C2 pedicle screw or C2/3 pedicle/lateral mass screw fixation is currently popular in posterior operations[11-13]. In clinical practices, the decision of surgical approach depends on surgeon’s training and experience, however, if displacement and/or angulation could not be reduced pre-operatively, posterior approach is not suggested[2].
At present, anterior plating is commonly used in treatment of types II and IIa Hangman’s fracture for its rigid fixation and protection against graft complications; however, the high cervical retropharyngeal approach which is employed in surgical exposure involved lots of dissection and traction around important structures[14-16]. As the consequence of complicate operative procedures, nerves could be mistaken into vessels and injured[17].
Is there any alternative surgical method besides plate fixation and the retropharyngeal approach for Hangman’s fracture? To reduce iatrogenic operative injury and simplify surgical procedure, a polyetheretherketone cage (Solis, Stryker Corporation, Cestas, France) is employed in our innovative technique which was performed by Smith and Robinson approach. To our knowledge, this method has not been reported before. To demonstrate the reliability, this method is applied to a series of patients. After follow-up, functional and radiological results are evaluated.
This is a retrospective clinical study.
From January 2010 to September 2012, polyetheretherketone cage fixation for Hangman’s fracture was performed in selected patients admitted to our hospital.
This research was designed as a clinical retrospective study in a single center. The diagnosis was made when bi-lateral lamina fractures of axis were recognized. The surgical inclusion criteria were: (1) patients manifested neurologic deficits and/or the fracture was determined to be unstable (i.e., angulation more than 11° and/or translation more than 3.5 mm); (2) type II or IIa Hangman’s fracture (Levine and Edwards’ classification). The exclusion criteria were that (1) type I or III Hangman’s fracture (Levine and Edwards’ classification); (2) in addition to Hangman’s fracture there are other spine fractures; (3) the fracture cannot be reduced by skill traction; (4) not suitable to be treated surgically. In total, eight consecutive patients were identified. Among these patients, there were five men and three women. Average age at surgery was 25.9 years (range 19 to 34 year). The majority of fracture cause was vehicle accidents (5 cases, 62.5%). Other causes were fall from a height (2 cases, 25%) and head trauma (1 case, 12.5%). Two stable cases were excluded; one with type III fracture was treated by posterior approach and one patient with unfavorable health condition was treated non-operatively. Furthermore, preoperative cervical three-dimensional-CT scan was used to exclude other cervical fractures in all of our patients and preoperative MRI was conducted to detect spinal cord compression and upper cervical disc/ligament injuries. Demographic information and classification according to Levine and Edwards were recorded (Table 1).
b1.jpg)
Implants
The operations were performed using polyetheretherketone (PEEK) cages (Stryker Corporation, Cestas, France). The width of the cage, either 12 or 14 mm, was decided by intra-operative measurements; the high of the cage was 1 to 2 mm taller than preoperative disc high of C3/4 to secure stability.
Before surgery, all of our patients received skull traction; the initial weight was 2 kg, if no further displacement could be observed on regular examination of X-ray pictures, traction weight would be increased until 1/10 of body weight. Simultaneously, traction angle was adjusted until the fracture was reduced.
Surgical procedures
The same team of doctors performed all the operations. Under general endotracheal anesthesia, patients were positioned supine with the neck extended and slightly left rotated. A left skin incision was made according to Smith and Robinson approach. The incision was about 4 cm long with its middle point located on the level of superior boarder of thyroid cartilage. Blunt dissections were employed through fascial spaces to reach the avascular plane on C3 vertebral body. Extreme care was taken to differentiate nerve from vessels which went across this area. After exposure of C3, the dissection moved upward and went along with the avascular plane. A needle was inserted into the C2/3 disc space to confirm anatomical position under fluoroscope. After exposure of axis body (usually limited to the lower 1/3), the anchoring pin of distracter was drilled into the cortex. Robinson-spondylodesis procedure was performed to remove discoligamental injuries while preserving osteal endplates (Figure 1). After distraction of the disc space, an adequate size Solis which filled with autograft trabecular bone was put into the operative segment. The bone was harvested from the iliac crest with a T-shaped driver to minimize pain at the donor site. After removal of distracter, the stability of Solis was checked by anterior drawing, and then fluoroscope was used to detect the implant’s position. All of our patients were treated postoperatively with a plastic collar which had to be worn constantly for 3 months.
t1(1).jpg)
Outcome measurements
We conducted regular X-ray picture examinations at 1-week, 3-month, 6-month and the most recent follow-up postoperatively. The radiologic materials were evaluated for location of PEEK cages and condition of the operative levels. Fusion was considered complete when the following criteria were met[18]: (1) trabecular bone across the interfaces and connects superior and inferior vertebral bodies. (2)Radiolucencies inside the cage disappeared. (3) Adequate disc height was restored, without collapse-induced kyphosis.
In order to investigate the stability of Solis, we measure angulation (α) and displacement (β) pre- and post-operatively. α was the angle between inferior border of axis and superior border of C3, if the angle points anterior, it is considered to be negative, and if it points posterior, it is considered to be positive. β was the distance between the posterior border of axis and C3. These strategies were taken at the same time points which were at hospital admittance and 6-month follow-up visit. Fusion and strategy collection were confirmed by two different radiologic reviewers, who were blinded to the clinical outcome of our patients. If there was disagreement, a third person was consulted and decision was made by their discussion.
The postoperative functional outcomes were evaluated using the Clinical Post-Traumatic Neck Score (Mayo)[19]. This score system contains critical information such as neck pain, cervical movement, neurological statue and daily leaving activities. Scores were recorded on same time points which were also at hospital admittance and at 6-month follow-up visit for better comparison. Simultanesouly, visual analogue scale (VAS) score was recorded when we are performing questionnaire of Neck Score to further investigate neck pain.
Statistical analysis
Data were analyzed by SPSS software (SPSS, Chicago, IL, USA) and presented as the mean ± SD. The Q-Q plot (a normality test) for an approximation to normal distribution was utilized. The paired t-test was generally applied for normally distributed data sets of angulation (α), displacement (β) and Neck Score. To compare different levels, Wilcoxon signed ranks test was used for VAS. A value of P < 0.05 (two-tailed) was considered significant and confidence interval was 95%.
(1) Preoperative skill traction: The traction is critically important, not only because the fracture could be reduced, but also the function of upper cervical ligament could be testified pre-operatively. Since the stability of intravertebral device depends on compressive loads, the flexibility of upper cervical ligament is the key element of a successful surgery.
The major limitation of this study is the small number of patients, which precludes absolute conclusions with regard to the utility of Solis in treatment of Hangman’s fracture. Moreover, the functional and radiologic outcomes were almost equal with the results of previous clinical studies concerning plate fixation, except operative complications, such as hypoglossal nerve injury[15]. Although clinical study demonstrated the feasibility of Solis fixation, the stability still has to be further investigated by biomechanical researches. Hence, it is recommended in the following conditions: (1) type II and IIa Hangman’s Fractures with obvious C2/3 disc injury and/or angulation more than 11° and/or translation more than 3.5 mm; (2) the displacement should be no more than 5 mm; (3) the fracture could be reduced by skull traction.
1 文章创新性地提出一种应用于治疗Ⅱ型或Ⅱa型Hangman骨折(Levine and Edwards分型)的新型手术方法。术中经前路清除损伤的韧带及椎间盘后,借助牵引与压缩原理,固定多聚醚酮椎间融合器于C2/3椎间。为保证椎间稳定,术前患者均行颅骨牵引以验证上颈椎韧带的张力及复位骨折。试验共收集8例患者,所有椎间均牢固融合,无内植物移位、破裂,无椎间隙塌陷或假关节形成。成角及移位均良好纠正,术后颈部疼痛消退,临床疗效良好。 2 试验所采用的Smith-Robison入路为脊柱外科医师所熟悉,相对于传统的高位颈椎咽后入路,可避免神经血管周围的广泛分离,而且手术时间短,可推荐临床应用。
目前,广泛应用于Ⅱ型或Ⅱa型型Hangman骨折手术治疗的颈前路钛板内固定术具有减少椎间植骨相关并发症以及固定确实的优点。然而,手术显露所采用的颈椎高位咽后入路需进行重要结构周围的切开及牵拉,容易造成神经及血管的医源性损伤。除了上述手术方式外,是否有其它治疗Hangman骨折更为简便有效的方法?文章创新性地应用一种多聚醚酮椎间融合器经Smith and Robinson法显露C2/3椎间盘治疗Hangman骨折。为证实新型手术方式的可靠性,文章收集了相关病例,术后进行随访及X射线检查,并对临床疗效加以评价。
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||