中国组织工程研究 ›› 2014, Vol. 18 ›› Issue (43): 6896-6901.doi: 10.3969/j.issn.2095-4344.2014.43.002
• 组织工程骨及软骨材料 tissue-engineered bone and cartilage materials • 上一篇 下一篇
自体微小颗粒骨与骨形态发生蛋白2混合移植修复感染性骨不连
王 军,时宁文,钱红波,王一村
- 解放军南京军区南京总医院骨科,江苏省南京市 210002
-
收稿日期:2014-09-20出版日期:2014-10-15发布日期:2014-10-15 -
通讯作者:时宁文,副主任医师,解放军南京军区南京总医院骨科,江苏省南京市 210002 -
作者简介:王军,男,1986年生,汉族,江苏省盐城市人,2011年东南大学毕业,硕士,医师,主要从事创伤外科、感染、修复重建的临床与基础研究。
Autogenous micromorselized bone grafting mixed with bone morphogenetic protein-2 to repair infected nonunion
Wang Jun, Shi Ning-wen, Qian Hong-bo, Wang Yi-cun
- Department of Orthopedics, Nanjing General Hospital of Nanjing Military Region, Nanjing 210002, Jiangsu Province, China
-
Received:2014-09-20Online:2014-10-15Published:2014-10-15 -
Contact:Shi Ning-wen, Associate chief physician, Department of Orthopedics, Nanjing General Hospital of Nanjing Military Region, Nanjing 210002, Jiangsu Province, China -
About author:Wang Jun, Master, Physician, Department of Orthopedics, Nanjing General Hospital of Nanjing Military Region, Nanjing 210002, Jiangsu Province, China
摘要:
背景:感染性骨不连是目前创伤骨科治疗的难题,既要彻底清除感染病灶组织控制感染,修复缺损软组织闭合创面,又要修复骨缺损促进骨折愈合,最大程度恢复肢体的功能。由于自体微小颗粒骨取材方便,重组人骨形态发生蛋白2来源广泛,其混合植骨模式成骨可靠、安全性高,适于修复感染性骨不连。 目的:观察骨形态发生蛋白2混合自体微小颗粒骨移植修复感染性骨不连的治疗效果。 方法:采用自体微小颗粒骨(髂骨、长骨干骺端松质骨)混合骨形态发生蛋白2修复感染性骨不连23例,股骨骨髓炎清创外固定固定后骨缺损7例,胫骨骨髓炎清创外固定固定后骨缺损16例,其中11例患者因瘢痕挛缩或软组织条件差继续使用外固定支架,患者12例改用内固定钢板固定,固定后1,3,6个月和1年复查X射线评价骨折愈合情况,并采用Johner-Wruhs评分评估临床疗效。 结果与结论:所有病例平均随访13.4个月,骨折愈合,骨不连均得以修复,创面均闭合,无感染复发。Johner-Wruhs评分优良率为95%。提示骨形态发生蛋白2混合自体微小颗粒骨移植模式,在感染性骨不连修复中来源广泛、成骨可靠和安全性高。
中图分类号:
引用本文
王 军,时宁文,钱红波,王一村. 自体微小颗粒骨与骨形态发生蛋白2混合移植修复感染性骨不连[J]. 中国组织工程研究, 2014, 18(43): 6896-6901.
Wang Jun, Shi Ning-wen, Qian Hong-bo, Wang Yi-cun. Autogenous micromorselized bone grafting mixed with bone morphogenetic protein-2 to repair infected nonunion[J]. Chinese Journal of Tissue Engineering Research, 2014, 18(43): 6896-6901.
2.1 参与者数量分析 所有23例患者均进入结果分析,无脱失。 2.2 骨形态发生蛋白2混合自体骨移植修复感染性骨不连的愈合情况及不良反应 23例患者混合骨移植固定后植骨全部成活,其中2例胫骨外固定架改为内固定后出现创面皮肤张力较大,部分皮缘坏死,均待消肿后经清创再次缝合后愈合。23例均获随访,随访时间10-23个月,平均13.4个月,感染未见复发,创面愈合良好,无窦道、骨外露及钢板外露,经X射线片、CT证实为骨折已愈合,除4例患者因骨折部位靠近关节需跨关节外固定造成一定程度关节功能障碍,其余患者均恢复正常行走,功能感觉良好。综合评估情况见表1。
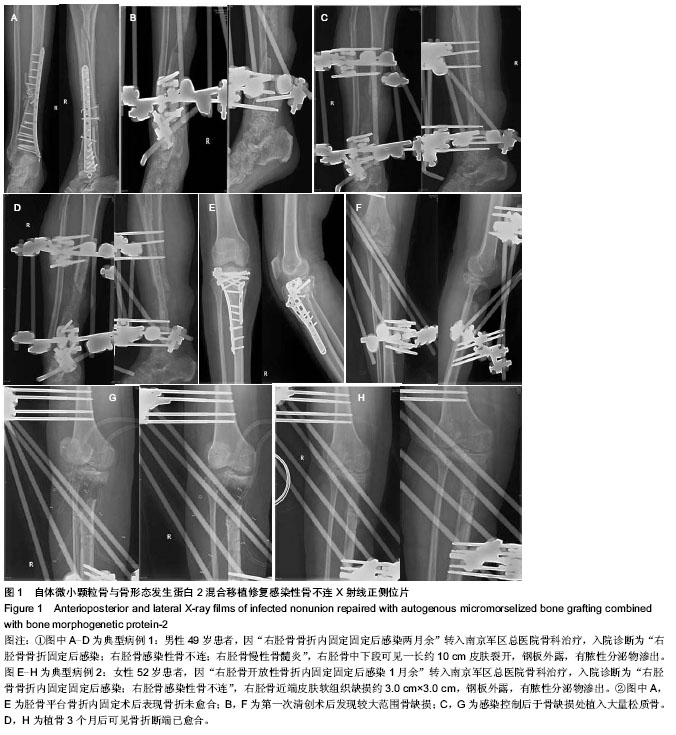
2.3 骨形态发生蛋白2混合自体骨移植修复感染性骨不连的并发症及不良反应 所有骨移植患者未出现明显的并发症及不良反应。2.4 典型病例 见图1。
| [1] Atkins RM.Principles of management of septic nonunion of fracture. Injury. 2007;38(Suppl 2):S23-S32. [2] Jain AK, Sinha S. Infected nonunion of the long bones. Clin Orthop Relat Res. 2005;(431):57-65. [3] Motsitsi NS. Management of infected nonunion of long bones: the last decade(1996-2006). Injury. 2008;39(2): 155-160. [4] Rigal S, Merloz P, Le N. Bone transport techniques in posttraumatic bone defects. Orthop Traumatol Surg Res. 2012;98(1):103-108. [5] Mora R, Maccabruni A, Bertani B, et al. Revision of 120 tibial infected non-unions with bone and soft tissue loss treated with epidermato-fascial osteoplasty according to Umiarov. Injury. 2014;45(2):383-387. [6] Lasanianos NG, Kanakaris NK, Giannoudis PV. Current management of long bone large segmental defects. Orthopaed Trauma. 2010;24(2):149-163. [7] 王新涛,闫景龙,杨显声,等.微小颗粒骨移植骨细胞活性的实验研究[J].中华创伤骨科杂志,2008,10(3):260-265. [8] McKay WF, Peckham SM, Badura JM. A comprehensive clinical review of recombinant human bone morphogenetic protein-2 (INFUSE Bone Graft). Int Orthop. 2007;31(6): 729-734. [9] 岳鹏举,赵建宁.骨形态发生蛋白2促进骨缺损修复的研究进展[J].医学研究生学报,2007,20(12):1302-1304. [10] Lo KW, Ulery BD, Ashe KM, et al. Studies of bone morphogenetic protein-based surgical repair. Adv Drug Del Rev. 2012;64(12):1277-1291. [11] 尹鹏.感染性骨不连的治疗进展[J].中国矫形外科杂志, 2013, 21(12):1198-1201. [12] 顾冬云.Johner-Wruhs分类与治疗提示[M].北京:人民军医出版社,2012. [13] Allende C, Mangupli M, Bagliardelli J, et al. Infected nonunions of long bones of the upper extremity: staged reconstruction using polymethylmethacrylate and bone graft impregnated with antibiotics. Chir Organi Mov. 2009;93(3):137-142. [14] Loeffler BJ, Kellam JF, Sims SH. Prospective observational study of donor-site morbidity following anterior Iliac crest bone-grafting in orthopaedic trauma reconstruction patients. J Bone Joint Surg Am. 2012;94(18):1649-1654. [15] 熊卉,张伟,邓益辉.脱钙冻干异体骨移植对骨缺损的修复作用[J].中华实验外科杂志,2006,23(12):1547-1548. [16] 王丁丁,曾戎,杨敏儿,等.缓释型重组人骨形态发生蛋白2/壳聚糖生物骨修复材料诱导骨形成[J].中国组织工程研究与临床康复, 2011,15(25):4583-4586. [17] Yan MN, Ke-Rong D, Tang TT, et al. Reconstruction of peri-implant bone defects using impacted bone allograft and BMP-2 genemodified bone marrow stromal cells. J Biomed Mater Res A. 2010,93(1):304-313. [18] Yash M, Kolambkar, Joel D, et al. Spatiotemporal delivery of bone morphogenetic protein enhances functional repair of segmental bone defects. Bone. 2011;49(3):485-492. [19] 陆维举,李斌,刘刚.感染性骨不连伴大段骨缺损的治疗[J].中华医学杂志,2009,89(7):476-479. [20] 李志远,李刚,荆浩,等.自体微小颗粒骨一期治疗感染性骨缺损及骨不连的临床研究[J].宁夏医科大学学报,2012,34(4):385-387. [21] 喻赣鹏,陈丹袆,胡宁敏.自体微小颗粒骨移植治疗感染性骨缺损的实验研究[J].宁夏医科大学学报,2011,33(4):322-325. [22] 南宠,荆浩,周岳,等.自体微小颗粒骨植骨混合万古霉素开放性植骨修复感染性胫骨缺损[J].中国组织工程研究, 2013,17(25): 4585-4592. [23] 姚章喜,范天凤,陈欣志,等.灌洗、筋膜蒂皮瓣及外固定架I期治疗胫骨感染性不愈合、骨外露[J].中国现代医学杂志,2008,18(1): 119-122. [24] 陈志文,刘晖,翟文亮,等.I期开放松质骨植骨治疗感染性骨缺损[J].中国骨伤,2008,21(5):377-378. [25] Theos C, Koulouvaris P, Kottakis S, et al. Reconstruction of tibia defects by ipsilateral vascularized fibula transposition. Arch Orthop Trauma Surg. 2008;128(2):179-184. [26] 解琛,蔡锦方,宗玉,等.髓内腓骨移植结合 Ilizarov 技术治疗胫骨感染性骨不连及骨缺损(附7例报告)[J].山东医药, 2014, 54(17): 41-43. [27] Megas P, Saridis A, Kouzelis A, et al. The treatment of infected nonunion of the tibia following intramedullary nailing by the Ilizarov method. Injury. 2010;41(3):294-299. [28] EI-Gammal TA, Shiha AE, El-Deen MA, et al. Management of traumatic tibial defects using free vascularized fibula or Ilizarov bone transport: a comparative study. Microsurgery. 2008;28(5):339-346. [29] Shiha A, Hafez AR, Kenawey M. Salvage of complicated diaphyseal femoral fractures by I-stage open debridement and Ilizarov technique. Ann Plast Surg. 2013;71(5):519-521. [30] Bumbasirevic M, Tomic S, Lasic A, et al. War-related infected tibia nonunion with bone and soft tissue loss treated with bone transport using the Ilizarov method. Arch 0rthop Trauma Surg. 2010;130(6):739-749. [31] Danoff JR, Saifi C, Goodspeed DC, et al. Outcome of 28 open pilon fractures with injury severity-based fixation. Eur J Orthop Surg Traumatol. 2014 [Epub ahead of print]. [32] Hutsuliak VI. Experimental substantiation of the construction peculiarities of the universal apparatus, applied for transosseal osteosynthesis based on three-dimensional modelling. Klin Khir. 2014;(7):56-59. [33] Tresley J, Schoenleber SJ, Singer AD, et al. “Ilizarov” external fixation: what the radiologist needs to know. Skeletal Radiol. 2014 [Epub ahead of print]. [34] Demiralp B, Ege T, Kose O, et al. Reconstruction of intercalary bone defects following bone tumor resection with segmental bone transport using an Ilizarov circular external fixator. J Orthop Sci. 2014[Epub ahead of print]. [35] Balci HI, Kocaoglu M, Eralp L, et al. Knee flexion contracture in haemophilia: treatment with circular external fixator. Haemophilia. 2014 [Epub ahead of print]. [36] Nozaka K, Shimada Y, Kimura Y, et al. Successful treatment of nonunion with an Ilizarov ring fixator after ankle fracture for Charcot arthropathy: a case report. BMC Res Notes. 2014; 7: 503. [37] Khanfour AA, El-Rosasy M. Late onset tibia vara. Acute correction strategy: proper case selection and a simple external fixation technique. Acta Orthop Belg. 2014;80(2): 241-250. [38] Górski R, ?arek S, Modzelewski P, et al. Bilateral fatigue fractures of the bones of both crura in a patient with a history of abuse of alcohol and psychoactive substances treated with Ilizarov external fixator apparatus. Pol Orthop Traumatol. 2014; 79:123-131. |
| [1] | 袁家威, 张海涛, 揭 珂, 曹厚然, 曾意荣. 基于网络药理学研究桃红四物汤治疗假体周围感染的潜在靶点和机制[J]. 中国组织工程研究, 2021, 25(9): 1428-1433. |
| [2] | 李珊珊, 郭笑霄, 尤 冉, 杨秀芬, 赵 露, 陈 曦, 王艳玲. 感光细胞替代治疗视网膜变性疾病[J]. 中国组织工程研究, 2021, 25(7): 1116-1121. |
| [3] | 刘立华, 孙 伟, 王云亭, 高福强, 程立明, 李子荣, 王江宁. 头颈部开窗减压治疗L1型激素性股骨头坏死:单中心前瞻性临床研究[J]. 中国组织工程研究, 2021, 25(6): 906-911. |
| [4] | 袁新平, 邵艳波, 吴 超, 汪剑龄, 童梁成, 李 颖. 骨折端CT扫描参数个性化微分建模仿真目标骨段的准确性[J]. 中国组织工程研究, 2021, 25(6): 912-916. |
| [5] | 化昊天, 赵文宇, 张 磊, 白文博, 王新卫. 抗生素人工骨治疗慢性骨髓炎疗效和安全性的Meta分析[J]. 中国组织工程研究, 2021, 25(6): 970-976. |
| [6] | 张 宾, 孙丽华, 张俊花, 刘玉三, 崔彩云. 改良翻瓣即刻种植有利于上颌前牙区的软硬组织重建[J]. 中国组织工程研究, 2021, 25(5): 707-712. |
| [7] | 蒋 欣, 乔良伟, 孙 东, 李 明, 房 军, 曲青山. 肾移植患者血清中长链非编码RNA PGM5-AS1表达及调控人肾小球内皮细胞的作用[J]. 中国组织工程研究, 2021, 25(5): 741-745. |
| [8] | 杨 鑫, 金 喆, 冯 旭, 卢 兵. 沈阳市居民对器官、眼组织及遗体捐献的认知及意愿调查[J]. 中国组织工程研究, 2021, 25(5): 779-784. |
| [9] | 李晨杰, 吕林蔚, 宋 阳, 刘静娜, 张春秋. 预紧力作用下钛合金人工假体界面骨小梁形态参数测量与统计分析[J]. 中国组织工程研究, 2021, 25(4): 516-520. |
| [10] | 李兴平, 肖东琴, 赵 桥, 陈 硕, 白亦光, 刘 康, 冯 刚, 段 可. 钛表面载铜抗菌功能膜的制备及性能[J]. 中国组织工程研究, 2021, 25(4): 553-557. |
| [11] | 李 黎, 马 力. 磁性壳聚糖微球固定化乳糖酶及其酶学性质[J]. 中国组织工程研究, 2021, 25(4): 576-581. |
| [12] | 刘 飞, 崔宇韬, 刘 贺. 局部抗生素递送系统治疗骨髓炎的优势与问题[J]. 中国组织工程研究, 2021, 25(4): 614-620. |
| [13] | 李晓壮, 段 浩, 王伟舟, 唐志宏, 王旸昊, 何 飞. 骨组织工程材料治疗骨缺损疾病在体内实验中的应用[J]. 中国组织工程研究, 2021, 25(4): 626-631. |
| [14] | 马 瑞, 王家麟, 吴梦军, 葛 莹, 王 伟, 王坤正. 关节置换后假体周围感染病原菌分布及耐药情况与治疗周期的关系[J]. 中国组织工程研究, 2021, 25(3): 380-385. |
| [15] | 贺 杰, 常 祺. 四肢恶性骨肿瘤骨切除后大段骨缺损的生物重建[J]. 中国组织工程研究, 2021, 25(3): 420-425. |
|
||||||||||||||||
|
表1 自体微小颗粒骨与骨形态发生蛋白2混合移植修复感染性骨不连23例患者基本资料
Table 1 Baseline data of 23 infected nonunion patients undergoing autogenous micromorselized bone grafting with bone morphogenetic protein-2
|
|
统计学分析:所有数据均用x±s表示,应用SPSS 11.0软件进行数据分析,组间数据差异的比较采用两样本t 检验、单因素方差分析和SNK检验,检验水准α=0.05。
1 文章在一期清创彻底控制感染的前提下,二期应用自体微小颗粒骨混合骨形态发生蛋白2共同植骨模式,相比较以往一期植骨风险较大,固定后可能因创面渗出较多、创面张力较大并伴有缺损、感染复发等均会导致植骨失败,再次植骨还会因可用自体骨量减少,出现植骨成功率降低。而二期植骨时感染已控制、创面软组织条件良好,植骨存活率高。 2 试验未使用人工骨材料,考虑人工骨材料移植会发生免疫排异反应,成骨活性较差,虽可达到即时的植骨量要求,但往往成骨活性差,爬行替代和血管化时间较长,难以活化,而且容易感染。
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||