Design
Retrospective case analysis.
Time and setting
Experiments were conducted in the Department of Orthopedics, Renmin Hospital of Wuhan University in China from February 2011 to January 2013.
Subjects
Patients who had undergone percutaneous
pedicle screw fixation or traditional open internal fixation for simple vertebral compression fracture from February 2011 to January 2013 were enrolled, and informed consent was obtained from all participants.
Inclusion criteria
There were (1) diagnosed by ordinary X-ray films and thoracolumbar MRI; (2) single vertebral compression fracture below T10 without neurological symptoms and signs; and (3) informed consent to treatment programs, and approved by the hospital ethics committee.
Exclusion criteria
There were (1) multiple segments vertebral fractures; (2) thoracic spine fracture above T10; (3) patients with spinal canal stenosis demonstrated by MRI or lower limb neurological symptoms and signs; and (4) patients with obvious contraindications for surgical treatment.
Percutaneous pedicle screw fixation group
A total of 25 cases were enrolled, 15 males and 10 females, aged from 23 to 56 years (average, 32.5 ± 10.5 years). Injured segments: T11 in 5 cases, T12 in 4 cases, L1 in 8 cases, L2 in 3 cases, L3 in 3 cases and L4 in 2 cases. Cause of injury: high falling injury in 10 cases, traffic accident injury in 9 cases and falling injury in 6 cases.
Traditional open internal fixation group
A total of 30 cases were enrolled, 18 males and 12 females, aged from 18 to 60 years (average, 36.5 ± 11.8 years). Injured segments: T11 in 3 cases, T12 in 6 cases, L1 in 9 cases, L2 in 3 cases, L3 in 5 cases and L4 in 3 cases; cause of injury: high falling injury in 12 cases, traffic accident injury in 13 cases and falling injury in 5 cases.
Sextant percutaneous pedicle screw system including “male and female” extension rods, measuring plate, screws, and so on, made from titanium alloy, with good biocompatibility, is produced by Medtronic Inc., USA.
Methods
Internal fixation for single-level vertebral body compression fractures
Traditional open internal fixation group: After the success of general anesthesia, the patients were placed in prone position, and then positioning, sterilizing and laying aseptic towel were performed in order. A longitudinal incision was made along the locating pin, the skin and subcutaneous tissue were cut open, and paraspinous soft tissue was stripped to expose the injured vertebra and the vertebral lamina and upper and lower articular process of the upper and lower vertebrae. The pedicle screws were placed conventionally, and distraction was performed until reduce was satisfied. After irrigating wound surface and fixing drainage tube, the wound was sutured by layers.
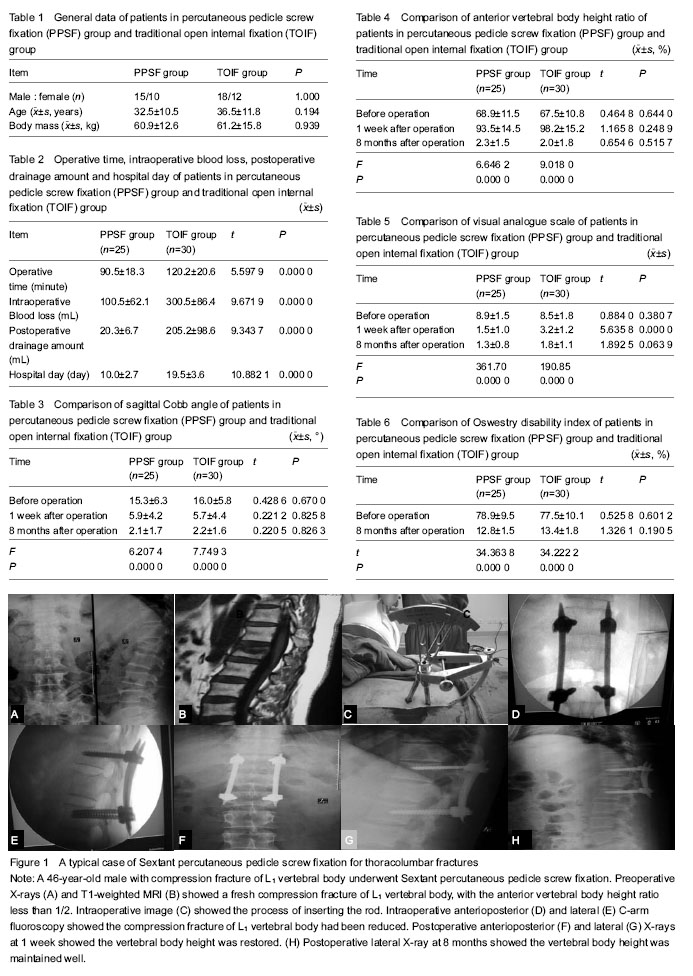
Percutaneous pedicle screw fixation group: after the success of general anesthesia, the patients were placed in the prone position with vacant abdomen. Using C-arm, the four pedicle “cat’s eyes” of the upper and lower vertebrae of the fractured vertebra was positioned. After routine disinfection and laying towels, the pedicle puncture was performed first on one side (e.g. left side). A 1.5 cm skin incision was made on the locating point. The needle was penetrated from 9:00 position of the “cat’s eye”, to a depth of 6 cm, with the needle on the middle and upper 1/3 of the pedicle by lateral fluoroscopy. After verification, three extenders with different sizes were inserted in order from small to large, and then hollow pedicle screw with suitable length was screwed into the pedicle, with U-shaped groove just touching the facet, finally universal pedicle screw extension rod was indwelt. Another homolateral screw was inserted with the same method. The “male and female” extension rods should be equal in altitude and jointed, and then measuring plate was installed to measure the length of the connecting rod. After confirming the length of the connecting rod, a proper connecting rod was inserted. Anteroposterior and lateral fluoroscopy was performed to observe the position of screws and rods; if the position was satisfactory, distraction and reduction was carried out for several times until the lateral vertebral height was satisfactory; finally the tail screws were tightened. The screws and rods on the other side were set with the same method.
Postoperative management
Anti-infection and symptomatic treatment was given to all patients. The drainage tubes were removed at 48 hours after operation. For patients who had undergone percutaneous pedicle screw fixation, no drainage tubes were put. Patients who had undergone percutaneous pedicle screw fixation could began out-of-bed activity under protection of chest-back support at 1 week after operation, while for patients who had undergone traditional open internal fixation, out-of-bed activity under protection of chest-back support was permitted at 1 month after operation. All patients began low back muscle training at 3 days after operation, and they were followed up at 1 week, 4, 8 and 12 months after operation.
Indexes during preoperative period
There were operative time, intraoperative blood loss and drainage amount (drainage amount in percutaneous pedicle screw fixation group was determined by number of soaked gauze, one soaked gauze was calculated as
20 mL), and hospital day.
Imaging indicators
There were pre- and postoperative sagittal Cobb angle and anterior vertebral bodyheight ratio, measured according to X-ray films.
Anterior vertebral body height ratio = injured anterior vertebral body height / referred anterior vertebralbody height×100%;
Referred anterior vertebral body height = (upper anterior vertebral body height + lower anterior vertebral body height)/2.
Main outcome measures
Visual analogue scale and Oswestry disability index were used to evaluate the clinical results.
Statistical analysis
Data were expressed as mean ± SD, and statistical analysis was performed using SPSS 19.0 software (SPSS Inc., Chicago, IL, USA). Sex constituent ratio was compared using Chi-square test; other data was analyzed using t-test or one-way analysis of variance. A value of P < 0.05 was considered statistically significant.