中国组织工程研究 ›› 2014, Vol. 18 ›› Issue (29): 4742-4751.doi: 10.3969/j.issn.2095-4344.2014.29.026
• 组织构建循证医学 evidence-based medicine in tissue construction • 上一篇 下一篇
肩袖损伤后单排与双排缝合方法比较的Meta分析
庄 泽,卢华定,陈郁鲜,彭 优,任建华,王 昆
- 中山大学附属第三医院关节创伤外科,广东省广州市 510630
-
修回日期:2014-05-26出版日期:2014-07-09发布日期:2014-07-09 -
通讯作者:王昆,主任医师,中山大学附属第三医院关节创伤外科,广东省广州市 510630 -
作者简介:庄泽,男,1984年生,广东省普宁市人,汉族,2007年中山大学毕业,医师,主要从事关节外科和创伤骨科的研究。
Single-row versus double-row suture in rotator cuff repair: a meta-analysis
Zhuang Ze, Lu Hua-ding, Chen Yu-xian, Peng You, Ren Jian-hua, Wang Kun
- Department of Joint Traumatic Surgery, Third Affiliated Hospital of Sun Yat-sen University, Guangzhou 510630, Guangdong Province, China
-
Revised:2014-05-26Online:2014-07-09Published:2014-07-09 -
Contact:Wang Kun, Chief physician, Department of Joint Traumatic Surgery, Third Affiliated Hospital of Sun Yat-sen University, Guangzhou 510630, Guangdong Province, China -
About author:Zhuang Ze, Physician, Department of Joint Traumatic Surgery, Third Affiliated Hospital of Sun Yat-sen University, Guangzhou 510630, Guangdong Province, China
摘要:
背景:肩袖修复的常见方式有单排缝合法和双排缝合法。既往有报道双排缝合法在临床上并未显示出比单排缝合更优的效果。
中图分类号:
引用本文
庄 泽,卢华定,陈郁鲜,彭 优,任建华,王 昆. 肩袖损伤后单排与双排缝合方法比较的Meta分析[J]. 中国组织工程研究, 2014, 18(29): 4742-4751.
Zhuang Ze, Lu Hua-ding, Chen Yu-xian, Peng You, Ren Jian-hua, Wang Kun . Single-row versus double-row suture in rotator cuff repair: a meta-analysis[J]. Chinese Journal of Tissue Engineering Research, 2014, 18(29): 4742-4751.
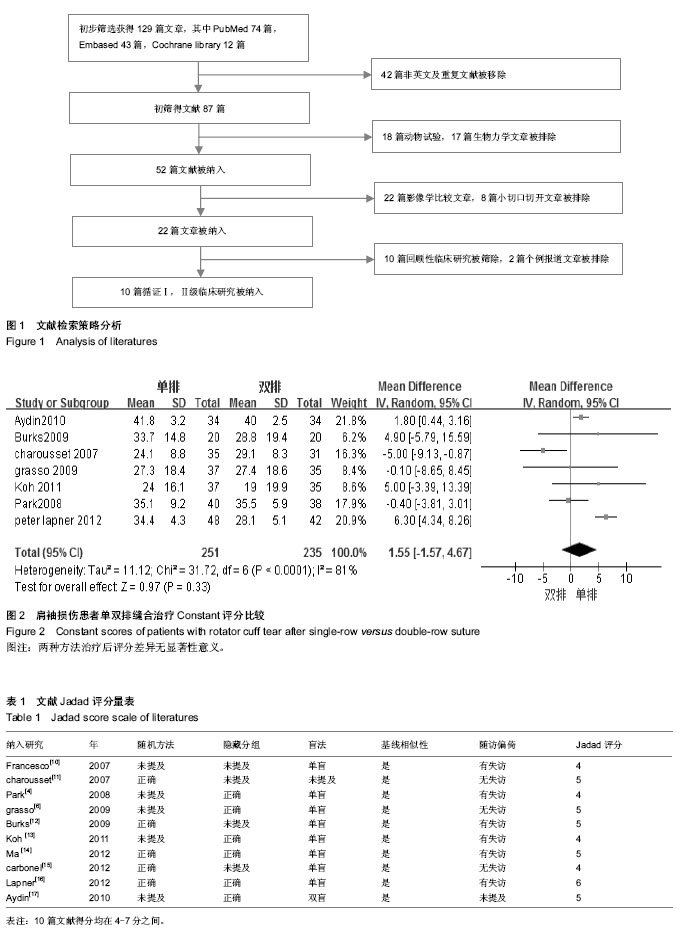
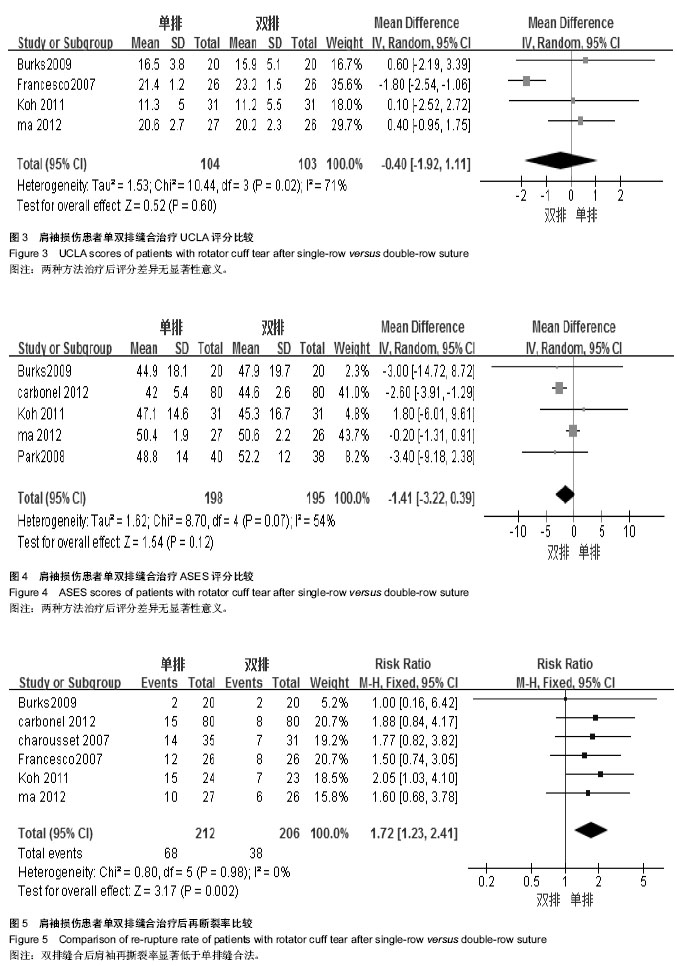
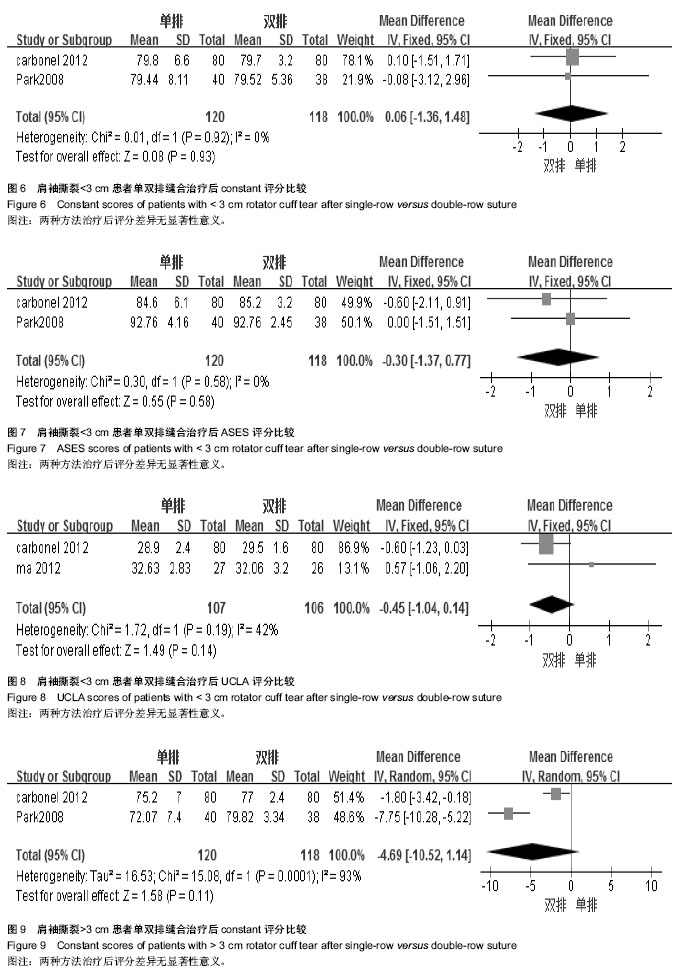
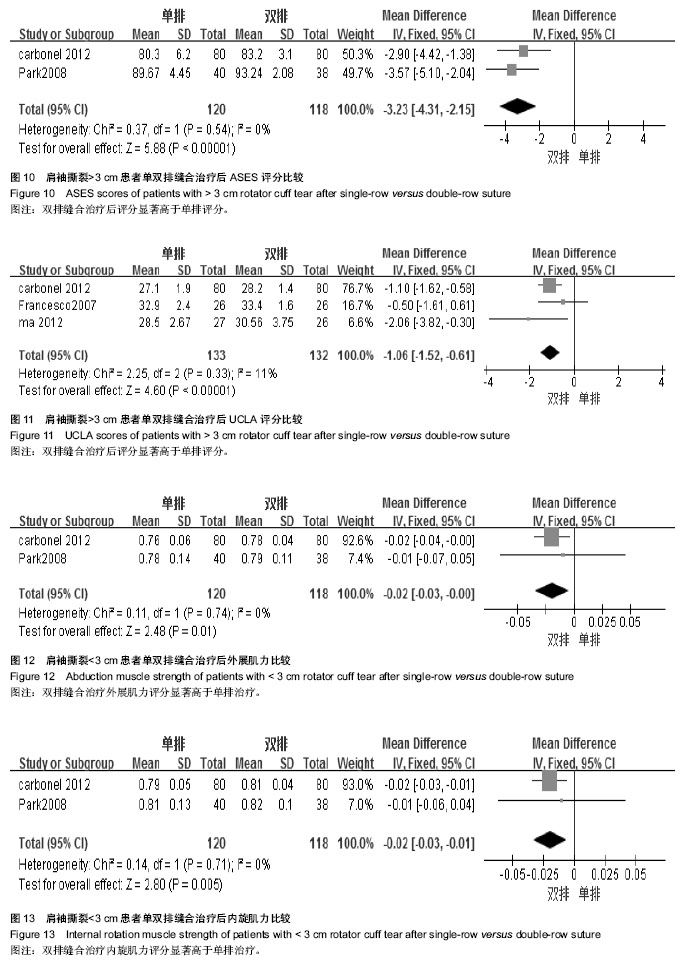
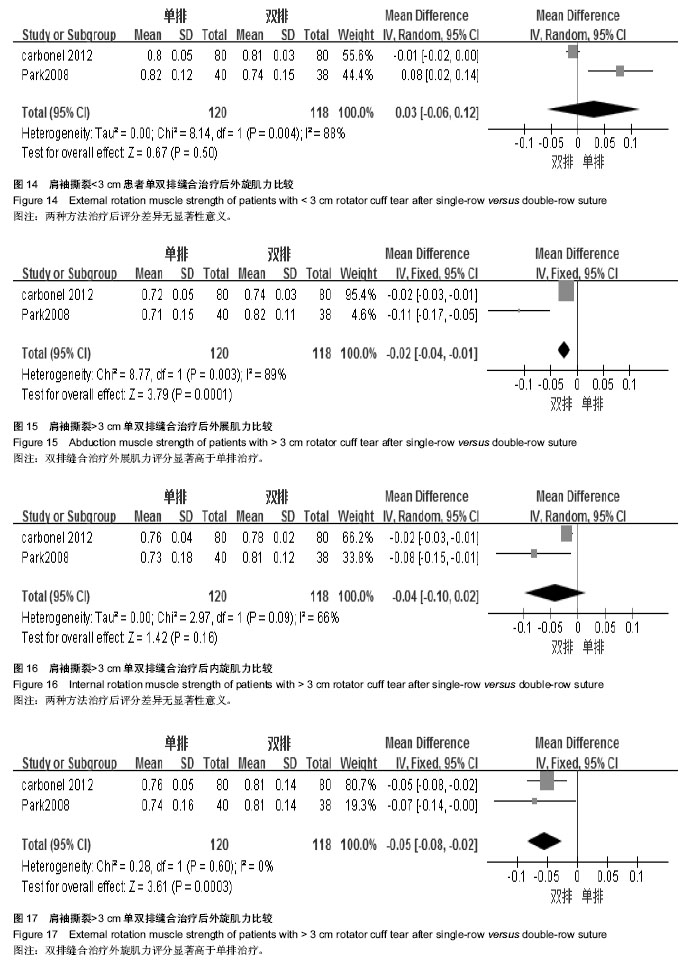
2.3 Meta分析结果 对数据进行4种分类比较:①总的肩袖损伤患者各类评分比较。②总的肩袖损伤患者外科治疗后再断裂率比较。③肩袖撕裂>3和<3 cm亚组分类的各类评分比较。④肩袖撕裂>3和<3 cm亚组分类的肩关节肌力指数(SSI)比较。
| [1] Liem D, Bartl C, Lichtenberg S, et al.Clinical outcome and tendon integrity of arthroscopic versus mini-open supraspinatus tendon repair: A magnetic resonance imaging-controlled matched-pair analysis. Arthroscopy. 2007; 23:514-521. [2] Smith CD, Alexander S, Hill AM, et al.A biomechanical comparison of single and double-row ?xation in arthroscopic rotator cuff repair.J Bone Joint Surg Am. 2006;88:2425-2431.
[3] Milano G, Grasso A, Zarelli D,et al.Comparison between single-row and double-row rotator cuff repair: A biomechanical study. Knee Surg Sports Traumatol Arthrosc.2008;16:75-80.
[4] Park JY, Lhee SH, Choi JH,et al.Comparison of the clinical outcomes of single- and double-row repairs in rotator cuff tears. Am J Sports Med.2008;36:1310-1316.
[5] Sugaya H, Maeda K, Matsuki K,et al. Functional and structural outcome after arthroscopic full-thickness rotator cuffrepair: Single-row versus dual-row ?xation. Arthroscopy. 2005;21:1307-1316.
[6] Grasso A, Milano G, Salvatore M,et al. Single-row versus double-row arthroscopic rotator cuff repair: A prospective randomized clinical study.Arthroscopy. 2009;25:4-12.
[7] Jadad AR, Moore RA, Corral D. Assessing the quality of the reports of randomized clinical trials: is blinding necessary? Control Clin Trials.1996;17(1):1-12.
[8] Constant CR, Murley AH.A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987: 160-164.
[9] Michener LA,McClure PW,Sennett BJ.American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: Reliability, validity, and respon-siveness. J Shoulder Elbow Surg.2002;11:587-594.
[10] Franceschi F, Ruzzini L, Longo UG, et al. Equivalent clinical results of arthroscopic single-row and double-row suture anchor repair for rotator cuff tears: A randomized controlled trial. Am J Sports Med 2007;35:1254-1260.
[11] Charousset C, Grimberg J, Duranthon LD,et al.Can a double-row anchorage technique improve tendonhealing in arthroscopic rotator cuff repair? A prospective non randomized, comparative study of double-row and single-row anchorage techniques with computed tomographic arthrography tendon healing assessment. Am J Sports Med. 2007;35:1247-1253.
[12] Burks RT, Crim J, Brown N,et al.A prospectiver and randomized clinical trial comparing arthroscopic single-and double-row rotator cuff repair. Am J Sports Med. 2009;37:647-683.
[13] Koh KH, Kang KC, Lim TK,et al. Prospective randomized clinical trial of single- versus double-row suture anchor repair in 2-to 4-cm rotator cuff tears: clinical and magnetic resonance imaging results. Arthroscopy.2011;27:453-462.
[14] Ma HL, Chiang ER, Wu HT,et al.Clinical outcome and imaging of arthroscopic single-row and double row rotator cuff repair: a prospective randomized trial. Arthroscopy.2012;28:16-24.
[15] Carbonel I, Martinez AA, Calvo A,et al.Single-row versus double-row arthroscopic repair in the treatment of rotator cuff tears: A prospective randomized clinical study. Int Orthop. 2012; 36:1877-1883.
[16] Lapner PL, Sabri E, Rakhra K, et al. A multicenter randomized controlled trial comparing single-row with double-row ?xation in arthroscopic rotator cuff repair.J Bone Joint Surg Am. 2012;94:1249-1257.
[17] Aydin N, Kocaoglu B, Guven O. Single-row versus double-row arthroscopic rotator cuff repair in small- to medium-sized tears. J Shoulder Elbow Surg.2010;19:722-5.
[18] Kim DH,Elattrache NS,Tibone JE, et al.Biomechanical comparison of a single-row versus double-row suture anchor technique for rotator cuff repair. Am J Sports Med. 2006;34: 407-414.
[19] Meier SW, Meier JD. The effect of double-row ?xation on initial repair strength in rotator cuff repair: A biomechanical study. Arthroscopy.2006;22:1168-1173.
[20] Cummins CA, Murrell GA.Mode of failure for rotator cuff repair with suture anchors identi?ed at revision surgery.J Shoulder Elbow Surg.2003;12:128-133.
[21] Wall LB, Keener JD, Brophy RH, et al.Systematic Review Clinical Outcomes of Double-Row Versus Single-Row Rotator Cuff Repairs.Arthroscopy.2009;25(11):1312-1318.
[22] Perser K,Godfrey D,Bisson L.Meta-analysis of Clinical and Radiographic Outcomes After Arthroscopic Single-Row Versus Double-Row Rotator Cuff Repair. Sports Health. 2011; 3(3):268-274
[23] DeHaan AM,Axelrad TW,Kaye E, et al. Does Double-Row Rotator Cuff Repair Improve Functional Outcome of Patients Compared With Single-Row Technique? Am J Sports Med. 2012;40(5):1176-1185.
[24] Bishop J, Klepps S, Lo IK, et al.Cuff integrity after arthroscopic versus open rotator cuff repair: A prospective study.J Shoulder Elbow Surg.2006;15:290-299.
[25] Nho SJ, Brown BS, Lyman S, et al. Prospective analysis of arthroscopic rotatorcuff repair: Prognostic factors affecting clinical and ultrasound outcome. J Shoulder Elbow Surg. 2009;18:13-20. |
| [1] | 陈子扬, 蒲 锐, 邓 爽, 袁凌燕. 外泌体对运动介导胰岛素抵抗类疾病的调控作用[J]. 中国组织工程研究, 2021, 25(25): 4089-4094. |
| [2] | 陈 扬, 黄邓高, 高元慧, 王顺兰, 曹 卉, 郑琳麟, 何浩伟, 罗思琴, 肖敬川, 张应爱, 张淑芳. 低强度脉冲场超声促进人脂肪间充质干细胞的增殖和黏附[J]. 中国组织工程研究, 2021, 25(25): 3949-3955. |
| [3] | 杨俊辉, 罗金莉, 袁小平. 人生长激素对人牙周膜干细胞增殖及成骨分化的影响[J]. 中国组织工程研究, 2021, 25(25): 3956-3961. |
| [4] | 孙建威, 杨新明, 张 瑛. 孟鲁司特联合骨髓间充质干细胞移植治疗脊髓损伤模型大鼠[J]. 中国组织工程研究, 2021, 25(25): 3962-3969. |
| [5] | 高 珊, 黄东静, 洪海漫, 贾京桥, 孟 斐. 人胎盘间充质干细胞及诱导的胰岛样细胞移植治疗妊娠期糖尿病大鼠效果比较#br#[J]. 中国组织工程研究, 2021, 25(25): 3981-3987. |
| [6] | 郝晓娜, 张英杰, 李玉云, 许 涛. 过表达脯氨酰寡肽酶的骨髓间充质干细胞修复肝纤维化模型大鼠[J]. 中国组织工程研究, 2021, 25(25): 3988-3993. |
| [7] | 刘建友, 贾中伟, 牛佳伟, 曹鑫杰, 张 栋, 魏 杰. 构建股骨3D数字化模型提出一种新的股骨颈前倾角测量方法[J]. 中国组织工程研究, 2021, 25(24): 3779-3783. |
| [8] | 孟令杰, 钱 辉, 盛晓磊, 陆剑锋, 黄建平, 祁连港, 刘宗宝. 3D打印建模联合骨水泥成形微创治疗塌陷Sanders Ⅲ型跟骨骨折[J]. 中国组织工程研究, 2021, 25(24): 3784-3789. |
| [9] | 钱选昆, 黄合飞, 武成聪, 刘克廷, 欧 华, 张金鹏, 任 静, 万建杉. 计算机导航微创经椎间孔腰椎椎间融合治疗腰椎滑脱[J]. 中国组织工程研究, 2021, 25(24): 3790-3795. |
| [10] | 胡 靖, 向 阳, 叶 川, 韩子冀. 3D打印辅助与徒手置钉经皮椎弓根钉内固定治疗胸腰椎骨折的1年随访[J]. 中国组织工程研究, 2021, 25(24): 3804-3809. |
| [11] | 舒启航, 廖亦佳, 薛静波, 晏怡果, 王 程. 新型颈椎3D打印多孔椎间融合器的三维有限元分析[J]. 中国组织工程研究, 2021, 25(24): 3810-3815. |
| [12] | 王一寒, 李 杨, 张 玲, 张 睿, 徐瑞达, 韩晓峰, 程光齐, 王伟力. 数字骨科三维可视化技术在股骨转子间骨折复位内固定中的应用[J]. 中国组织工程研究, 2021, 25(24): 3816-3820. |
| [13] | 孙玛骥, 王秋安, 张星晨, 郭 冲, 袁 峰, 郭开今. 新型颈椎前路经椎弓根固定钉板系统的研制及生物力学分析[J]. 中国组织工程研究, 2021, 25(24): 3821-3825. |
| [14] | 林 旺, 王盈盈, 郭卫中, 袁翠华, 许胜贵, 张申申, 林成寿. 胫骨平台后外侧柱骨折扩大外侧入路内固定增强力学稳定性及膝关节功能[J]. 中国组织工程研究, 2021, 25(24): 3826-3827. |
| [15] | 朱 云, 陈 渝, 邱 皓, 刘 盾, 靳国荣, 陈诗谋, 翁 政. 对侧皮质锁定螺钉治疗骨质疏松股骨骨折的有限元分析[J]. 中国组织工程研究, 2021, 25(24): 3832-3837. |
1.1 文献检索 两位作者独立计算机检索Medline (2003年1月至2014年2月)、Embase (2003年1月至2014年2月)、Cochrane library (2014年第2期)和相关的会议记录,检索语种限定在英文。主要英文检索词:“rotator cuff repair”、“rotator cuff tear”、“single-row”、“double-row”、“arthroscopy”、“randomly”、“randomized”、“trail”。
1.5 统计学分析 采用Revman 5.2软件对资料进行Meta分析。首先通过χ2和I2检验对同类研究间的异质性情况进行评估:若P > 0.05,I2 < 50%,说明研究间具有同质性,采用固定效应模型分析;若P < 0.05,I2 > 50%,说明研究间具有异质性,对其异质性来源进行分析,若无临床异质性,则采用随机效应模型分析。若有临床异质性则根据可能出现的异质性因素进行亚组分析,若异质性过大则放弃Meta分析改为描述性分析。
1 针对单双排缝合治疗肩袖损伤的不同优缺点,根据患者的个体特点选择最优缝合方式是一个有意义的临床问题。既往有荟萃分析认为单双排缝合治疗后肩关节功能评分并无统计学差异,但纳入文献相对较少,未对文献内在病例情况进一步分析及亚组分析,未进一步分析治疗后肌力情况和肩袖术后再断裂情况。 2 文章对单双排缝合治疗后效果的进一步更新荟萃评价,通过搜索循证Ⅰ级、Ⅱ级的高质量文献并进行Meta分析。结果显示:肩袖损伤的患者采用双排缝合相对于单排缝合法治疗后肩袖再撕裂率更低,外展肌力恢复情况更优。小于3 cm肩袖损伤单双排缝合法治疗后功能评分无明显差异,大于3 cm的肩袖损伤采用双排缝合法可取得更佳的治疗后功能评分。
王磊2013年比较关节镜下单排固定和双排固定治疗肩袖损伤的疗效。23例肩袖损伤患者(23肩)按随机数字表法分为单排固定组(12例)和双排固定组(11例),单排固定组采用2枚锚钉、简单缝合固定,双排固定组采用3枚锚钉、内排褥式缝合固定。术后24个月评价其临床功能,包括疼痛视觉模拟量表(VAS)评分、Constant评分、美国肩肘外科协会(ASES)评分、美国加州大学肩关节评分系统(UCLA)评分、肩关节活动度(前屈、内旋、外旋)、手术时间及患者满意度,并比较两组再撕裂情况及其临床功能。结果显示单排固定组手术时间短于双排固定组;两组临床功能(VAS、Constant、ASES、UCLA评分)、肩关节活动度(前屈、内旋、外旋)及患者满意度比较差异无统计学意义(P>0.05)。单排固定组术后全层再撕裂2例,双排固定组2例,两组比较差异无统计学意义(P>0.05);单排固定组部分分层再撕裂和全层再撕裂7例,双排固定组2例,两组比较差异有统计学意义(P=0.041);再撕裂患者临床功能(VAS、Constant、ASES、UCLA评分)比较差异无统计学意义(P>0.05)。表明双排固定治疗2-5 cm肩袖撕裂损伤在临床功能及再撕裂方面与单排固定相比并无明显优势。
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||