Study selection and characteristics of the included studies
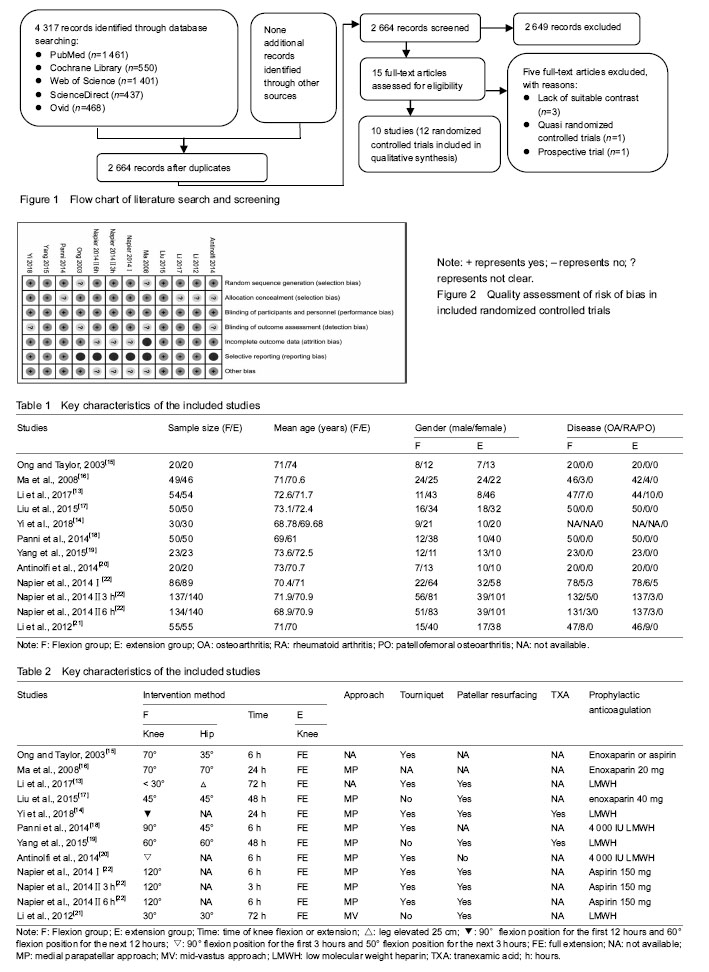
A total of 4 317 relevant studies were initially identified. After duplicate studies were removed, 2 664 studies were available for assessing titles and abstracts for eligibility. Of these, 15 articles were then evaluated for full-text articles. We eventually identified 10 articles[13-22] meeting the Inclusive criteria (Figure 1). Among these, the article by Napier et al.[22] had two RCTs and the second RCT had multiple comparisons. All selected studies were in English and were published between 2003 and 2018. Five studies[13-14, 17, 19, 21] were performed in China, two[15, 22] in UK, two[18,20] in Italy, and one[16] in Australia. The key characteristics of these studies are illustrated in Table 1, while study treatment protocol of the included study is shown in Table 2.
Quality assessment
The methodological quality of all the included RCTs was assessed based on the Cochrane Collaboration recommendations. Although all included RCTs declared randomization, only 10 RCTs mentioned the adequate randomization technique including a random number list[13, 17-21] and a sealed random number envelope[14, 22]. Allocation concealment was mentioned in six trials[14-17, 19, 22] and unclear in four trials[13, 18, 20-21]. Outcome assessors were blinded in six trials[13, 17-19, 21-22], but the blinding in the other four trials was unclear[14-16, 20]. The detailed risk of bias of methodological quality in the eligible RCTs is summarized in Figure 2.
 Outcomes of meta-analysis
Outcomes of meta-analysis
Total blood loss
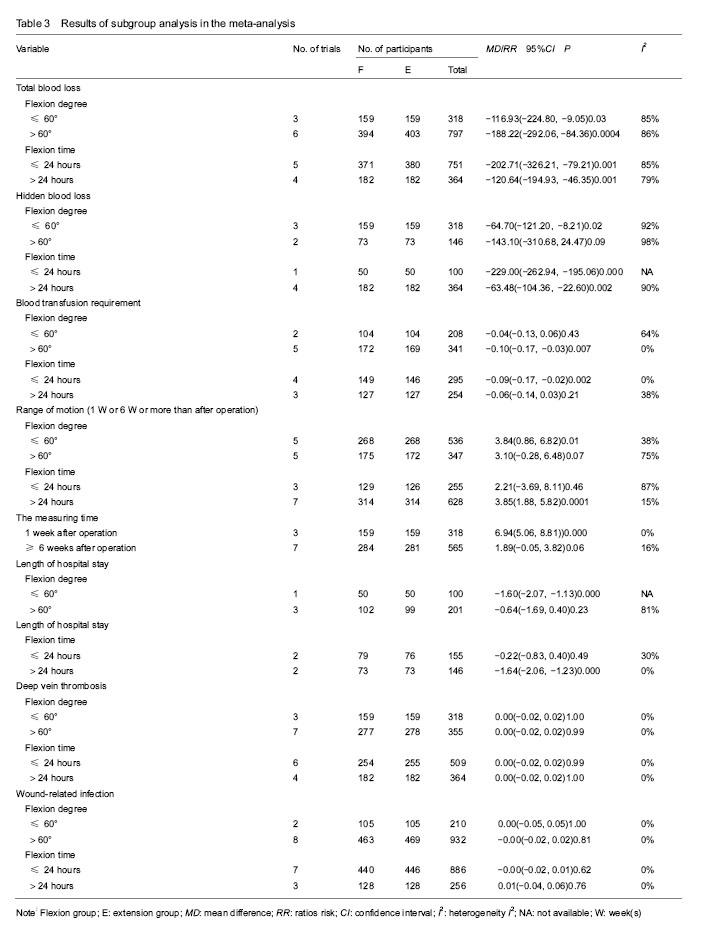
Total blood loss was mentioned in 8 studies[13-14, 17-22], including 1 115 patients (553 patients were in the flexion group and 562 patients in the extension group). Because of the high heterogeneity (P < 0.000 01, I²=88%), a random-effect model was used to pool the data. In pooled analyses, compared with the extension group, there was a significant reduction in the total blood loss in the flexion group (MD=-163.39; 95%CI, -232.74 to -94.04; P < 0.000 01; Figure 3). The subgroup analysis of total blood loss did not emerge any significant differences within all subgroups (Table 3).
Hidden blood loss
Five studies[13, 17-19, 21] with a total of 464 patients reported the outcome of hidden blood loss. Significant heterogeneity was found, so a random-model was adopted (P < 0.000 01, I²=96%). Pooling results demonstrated that there was an outstanding reduction in the hidden blood loss between flexion and extension groups (MD=-95.24; 95%CI, -153.64 to -36.84; P=0.001; Figure 4). In the subgroup analysis of hidden blood loss, there was no significant difference with subgroups based on the time of knee flexion. Subgroup analysis revealed significant reductions in hidden blood loss when the knee was fixed in the ≤ 60° of knee flexion (MD=-64.70; 95%CI, -121.20 to -8.21; P=0.02) compared with the > 60° of knee flexion (MD=-143.10; 95%CI, -310.68 to 24.47; P=0.09) (Table 3).
Blood transfusion requirement
Seven studies[13-19] with a total of 549 patients provided the data of blood transfusion requirement. Discovered no significant heterogeneity, a fixed-model was applied (P=0.59, I²=0%). The meta-analysis unmasked that there was a remarkable reduction in the blood transfusion requirement between flexion and extension groups (RR=-0.07; 95%CI, -0.13 to -0.02; P=0.010; Figure 5). The subgroup analysis revealed that blood transfusion requirement can markedly reduce when the knee was fixed in the > 60° of knee flexion (RR=-0.10; 95%CI, -0.17 to -0.03; P=0.007) in comparison with the ≤ 60° of knee flexion subgroup (RR=-0.04; 95%CI, -0.13 to 0.06; P=0.43). It could dramatically diminish when the knee was fixed for 24 hours (RR=-0.09; 95%CI, -0.17 to -0.02; P=0.002) compared with >24 hours (RR=-0.06; 95%CI, -0.14 to 0.03; P=0.21) (Table 3).
Range of motion
Data from 7 studies[13-14, 16-19, 21] including 883 patients were available for range of motion. Among seven studies, three studies[13, 19, 21] provided the multiple data of range of motion at 7 days, 6 weeks and 6 months postoperatively, which were also involved in pooled analyses. There was remarkable heterogeneity among studies (P=0.006, I²=61%); therefore, a random-model was performed. In pooled analyses, compared with the extension group, there was a significant improvement of range of motion in the flexion group (MD=3.50; 95%CI, 1.31 to 5.69; P=0.002; Figure 6). The subgroup analysis uncovered that range of motion can dramatically improve when the knee was fixed in the ≤ 60° of knee flexion (MD=3.84; 95%CI, 0.86 to 6.82; P=0.01) compared with the > 60° of knee flexion (MD=3.10; 95%CI, -0.28 to 6.48; P=0.07); that it can significantly increase when the knee was fixed for > 24 hours (MD=3.85; 95%CI, 1.88 to 5.82; P=0.000 1) in comparison with ≤ 24 hours (MD=2.21; 95%CI, -3.69 to 8.11; P=0.46); that it could markedly improve at 1 week postoperatively (MD=6.94; 95%CI, 5.06 to 8.81; P=0.000). On the contrary, similar results did not appear at 6 or more than 6 weeks postoperatively (MD=1.89; 95%CI, -0.05 to 3.82; P=0.06) (Table 3).
 Hospitalization time
Hospitalization time
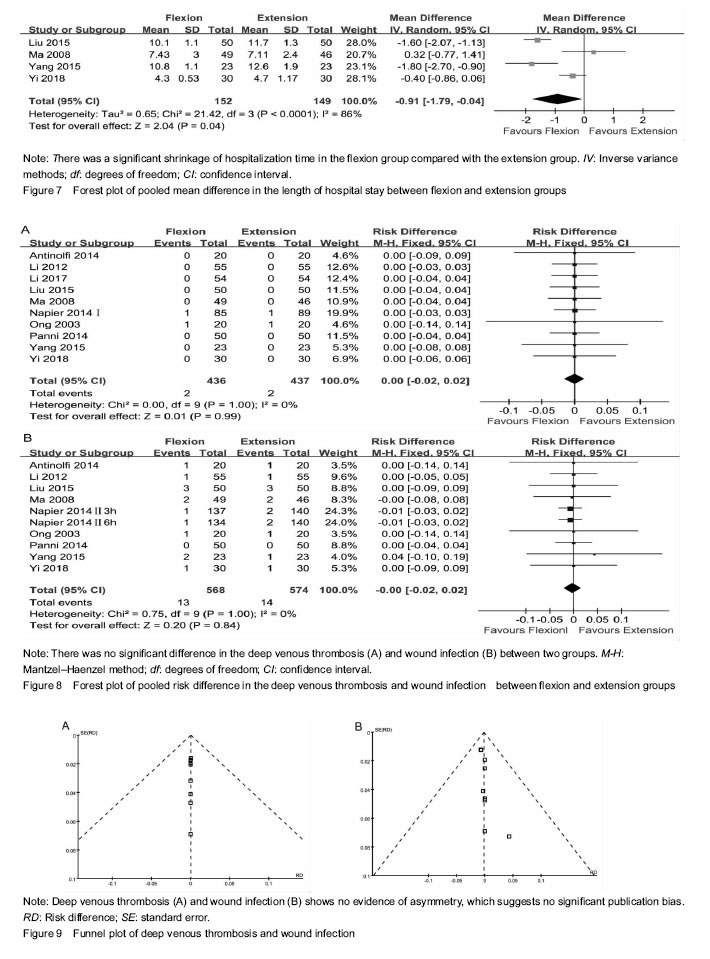
The hospitalization time was mentioned in 4 studies[14, 16-17, 19], including 301 patients (152 patients were in the flexion group and 149 patients in the extension group). Because of the high heterogeneity (P < 0.000 1, I²=86%), a random-effect model was adopted to pool the data. The meta-analysis uncovered that there was a significant shrinkage of hospitalization time in the flexion group compared with the extension group (MD=-0.91; 95%CI, -1.79 to -0.04; P=0.04; Figure 7). The subgroup analysis unmasked that length of hospitalization time could significantly shorten when the knee was fixed in the ≤ 60° of knee flexion (MD=-1.60; 95%CI, -2.07 to -1.13; P=0.000) compared with the > 60° of knee flexion (MD=-0.64; 95%CI, -1.69 to 0.40; P=0.23); that it can dramatically diminish when the knee was fixed for > 24 hours (MD=-1.64; 95%CI, -2.06 to -1.23; P=0.000) in comparison with the knee fixed time of > 24 hours (MD=-0.22; 95%CI, -0.83 to 0.40; P=0.49) (Table 3).
Deep venous thrombosis
Data from 10 studies [13-22] including 873 patients was available for deep venous thrombosis. There was no heterogeneity among studies (P=1.00, I²=0%); hence, a fixed-model was adopted. In pooled analyses, there was no significant between-group difference in the deep venous thrombosis (RR=0.00; 95%CI, -0.02 to 0.02; P=0.99; Figure 8A). The subgroup analysis of deep venous thrombosis did not emerge any significant differences among subgroups (Table 3).
Wound infection
Nine studies[14-22] with a total of 1 142 patients provided the data of wound infection. Detected no significant heterogeneity, a fixed-model was adopted (P=1.00, I²=0%). The meta-analysis unmasked that there was no significant difference in wound infection between flexion and extension groups (RR=-0.00; 95%CI, -0.02 to 0.02; P=0.84; Figure 8B). In the subgroup analysis of wound infection, there was no significant difference among subgroups (Table 3).
Publication bias
Two funnel plots respectively based on deep venous thrombosis and wound infection were used to assess publication bias. Both figures demonstrated only minimal asymmetry and a few outliers, indicating minimal evidence of publication bias (Figure 9).