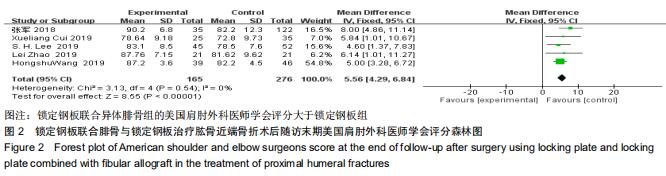
|
[1] PASSARETTI D, CANDELA V, SESSA P, et al. Epidemiology of proximal humeral fractures: A detailed survey of 711 patients in a metropolitan area. J Shoulder Elbow Surg. 2017;26(12): 2117-2124.
[2] BAHRS C, STOJICEVIC T, BLUMENSTOCK G, et al. Trends in epidemiology and patho-anatomical pattern of proximal humeral fractures. Int Orthop. 2014;38(8):1697-1704.
[3] MCLEAN AS, PRICE N, GRAVES S, et al. Nationwide trends in management of proximal humeral fractures: An analysis of 77,966 cases from 2008 to 2017. J Shoulder Elbow Surg. 2019;28(11): 2072-2078.
[4] LAUNONEN AP, LEPOLA V, FLINKKILA T, et al. Conservative treatment, plate fixation, or prosthesis for proximal humeral fracture. A prospective randomized study. BMC Musculoskelet Disord. 2012;13:167.
[5] OLERUD P, AHRENGART L, PONZER S, et al. Internal fixation versus nonoperative treatment of displaced 3-part proximal humeral fractures in elderly patients: A randomized controlled trial. J Shoulder Elbow Surg. 2011; 20(5):747-755.
[6] TAN E, LIE D, WONG MK. Early outcomes of proximal humerus fracture fixation with locking plate and intramedullary fibular strut graft. Orthopedics. 2014; 37(9): e822-827.
[7] LITTLE MT, BERKES MB, SCHOTTEL PC, et al. The impact of preoperative coronal plane deformity on proximal humerus fixation with endosteal augmentation. J Orthop Trauma. 2014; 28(6):338-347.
[8] 张军,庄云强,李东贞,等.锁定钢板结合异体腓骨支撑治疗老年肱骨近端neer三、四部分骨折[J].中华创伤骨科杂志,2018,20(11): 946-952.
[9] 张硕,汪秋柯,陈云丰,等. 定钢板结合异体腓骨治疗头内翻型肱骨近端骨折[J].中华肩肘外科电子杂志,2018,6(1): 9-24.
[10] 张清旭.锁定钢板结合异体腓骨植骨对老年肱骨近端骨折的疗效[J]. 深圳中西医结合杂志,2019,29(14):188-189.
[11] 常祖豪,朱正国,齐红哲,等.锁定钢板结合异体腓骨治疗老年肱骨近端粉碎性骨折的中远期疗效观察[J].解放军医学院学报,2019,40(2): 106-112.
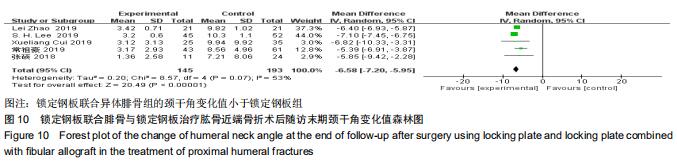
[12] LEE SH, HAN SS, YOO BM, et al. Outcomes of locking plate fixation with fibular allograft augmentation for proximal humeral fractures in osteoporotic patients: Comparison with locking plate fixation alone. Bone Joint J. 2019;101-b(3): 260-265.
[13] ZHAO L, QI YM, YANG L, et al. Comparison of the effects of proximal humeral internal locking system (philos) alone and philos combined with fibular allograft in the treatment of neer three- or four-part proximal humerus fractures in the elderly. Orthop Surg. 2019;11(6):1003-1012.
[14] CUI X, CHEN H, MA B, et al. Fibular strut allograft influences reduction and outcomes after locking plate fixation of comminuted proximal humeral fractures in elderly patients: A retrospective study. BMC Musculoskelet Disord. 2019;20(1): 511.
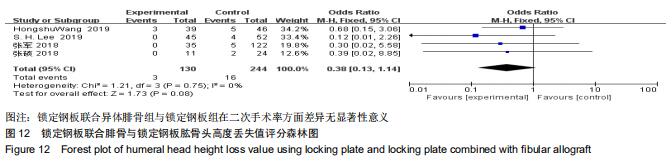
[15] WANG H, RUI B, LU S, et al. Locking plate use with or without strut support for varus displaced proximal humeral fractures in elderly patients. JB JS Open Access. 2019;4(3).pii: e0060.1-8.
[16] LAUNONEN AP, SUMREIN BO, REITO A, et al. Operative versus non-operative treatment for 2-part proximal humerus fracture: A multicenter randomized controlled trial. PLoS Med. 2019;16(7): e1002855.
[17] BEKS RB, OCHEN Y, FRIMA H, et al. Operative versus nonoperative treatment of proximal humeral fractures: A systematic review, meta-analysis, and comparison of observational studies and randomized controlled trials. J Shoulder Elbow Surg. 2018;27(8):1526-1534.
[18] FU BS, JIA HL, ZHOU DS, et al. Surgical and non-surgical treatment for 3-part and 4-part fractures of the proximal humerus: A systematic review of overlapping meta-analyses. Orthop Surg. 2019;11(3):356-365.
[19] 赵洪斌,宋洋,黄明光,等.锁定钢板治疗不同neer分型肱骨近端骨折的疗效及生物力学恢复情况的评价[J].中国全科医学,2019,22(32): 3985-3989.
[20] 孙相祥,衡立松,马建兵,等. 骨近端锁定钢板治疗肱骨近端4部分骨折[J].中国组织工程研究,2012,16(44):8206-8211.
[21] YANG TC, SU YP, CHANG MC. The elderly have similar outcomes compared to younger patients after orif with locking plate for comminuted proximal humerus fracture. Acta Orthop Traumatol Turc. 2019;53(1):1-5.
[22] THANASAS C, KONTAKIS G, ANGOULES A, et al. Treatment of proximal humerus fractures with locking plates: A systematic review. J Shoulder Elbow Surg. 2009;18(6): 837-844.
[23] HINDS RM, GARNER MR, TRAN WH, et al. Geriatric proximal humeral fracture patients show similar clinical outcomes to non-geriatric patients after osteosynthesis with endosteal fibular strut allograft augmentation. J Shoulder Elbow Surg. 2015;24(6): 889-896.
[24] NEVIASER AS, HETTRICH CM, BEAMER BS, et al. Endosteal strut augment reduces complications associated with proximal humeral locking plates. Clin Orthop Relat Res.2011;469(12): 3300-3306.
[25] WANG JQ, JIANG BJ, GUO WJ, et al. Serial changes in the head-shaft angle of proximal humeral fractures treated by placing locking plates: A retrospective study. BMC Musculoskelet Disord. 2018;19(1):420.
[26] BAI L, FU ZG, WANG TB, et al. Radiological evaluation of reduction loss in unstable proximal humeral fractures treated with locking plates. Orthop Traumatol Surg Res. 2014;100(3): 271-274.
[27] PANCHAL K, JEONG JJ, PARK SE, et al. Clinical and radiological outcomes of unstable proximal humeral fractures treated with a locking plate and fibular strut allograft. Int Orthop. 2016;40(3): 569-577.
[28] JOST B, SPROSS C, GREHN H, et al. Locking plate fixation of fractures of the proximal humerus: Analysis of complications, revision strategies and outcome. J Shoulder Elbow Surg. 2013; 22(4):542-549.
[29] CHEN H, ZHU ZG, LI JT, et al. Finite element analysis of an intramedulary anatomical strut for proximal humeral fractures with disrupted medial column instability: A cohort study. Int J Surg. 2020;73:50-56.
[30] CHOW RM, BEGUM F, BEAUPRE LA, et al. Proximal humeral fracture fixation: Locking plate construct +/- intramedullary fibular allograft. J Shoulder Elbow Surg. 2012;21(7):894-901.
[31] DI TULLIO PO, GIORDANO V, SOUTO E, et al. Biomechanical behavior of three types of fixation in the two-part proximal humerus fracture without medial cortical support. PLoS One. 2019;14(7):e0220523.
[32] KIM DS, LEE DH, CHUN YM, et al. Which additional augmented fixation procedure decreases surgical failure after proximal humeral fracture with medial comminution: Fibular allograft or inferomedial screws? J Shoulder Elbow Surg. 2018;27(10): 1852-1858.
[33] HE Y, ZHANG Y, WANG Y, et al. Biomechanical evaluation of a novel dualplate fixation method for proximal humeral fractures without medial support. J Orthop Surg Res. 2017;12(1):72.
[34] SALTZMAN BM, ERICKSON BJ, HARRIS JD, et al. Fibular strut graft augmentation for open reduction and internal fixation of proximal humerus fractures: a systematic review and the authors' preferred surgical technique. Orthop J Sports Med. 2016;4(7): 2325967116656829.
[35] CHEN H, YIN P, WANG S, et al. The augment of the stability in locking compression plate with intramedullary fibular allograft for proximal humerus fractures in elderly people. Biomed Res Int. 2018, 2018: 3130625.
[36] HSIAO CK, TSAI YJ, YEN CY, et al. Intramedullary cortical bone strut improves the cyclic stability of osteoporotic proximal humeral fractures. BMC Musculoskelet Disord. 2017;18(1):64.
|