中国组织工程研究 ›› 2017, Vol. 21 ›› Issue (32): 5240-5248.doi: 10.3969/j.issn.2095-4344.2017.32.026
• 组织构建循证医学 evidence-based medicine in tissue construction • 上一篇
Meta分析评价手术辅助上颌快速扩弓矫治成人上颌横向发育不足的稳定性
费 露,白 洋,袁小平
- (西南医科大学附属口腔医院正畸科,四川省泸州市 646000)
-
收稿日期:2017-06-25出版日期:2017-11-18发布日期:2017-11-15 -
通讯作者:袁小平,教授,硕士生导师,西南医科大学附属口腔医院,四川省泸州市 646000 -
作者简介:费露,女,1991年生,四川省犍为县人,西南医科大学在读硕士,主要从事口腔正畸研究。
Stability improvement in adult maxillary transverse deficiency after surgically assisted rapid maxillary expansion: a Meta-analysis
Fei Lu, Bai Yang, Yuan Xiao-ping
- (Department of Orthodontics, Hospital of Stomatology of Southwest Medical University, Luzhou 646000, Sichuan Province, China)
-
Received:2017-06-25Online:2017-11-18Published:2017-11-15 -
Contact:Yuan Xiao-ping, Professor, Master’s supervisor, Department of Orthodontics, Hospital of Stomatology of Southwest Medical University, Luzhou 646000, Sichuan Province, China -
About author:Fei Lu, Studying for master’s degree, Department of Orthodontics, Hospital of Stomatology of Southwest Medical University, Luzhou 646000, Sichuan Province, China
摘要:
文章快速阅读:
.jpg)
中图分类号:
引用本文
费 露,白 洋,袁小平. Meta分析评价手术辅助上颌快速扩弓矫治成人上颌横向发育不足的稳定性[J]. 中国组织工程研究, 2017, 21(32): 5240-5248.
Fei Lu, Bai Yang, Yuan Xiao-ping. Stability improvement in adult maxillary transverse deficiency after surgically assisted rapid maxillary expansion: a Meta-analysis[J]. Chinese Journal of Tissue Engineering Research, 2017, 21(32): 5240-5248.
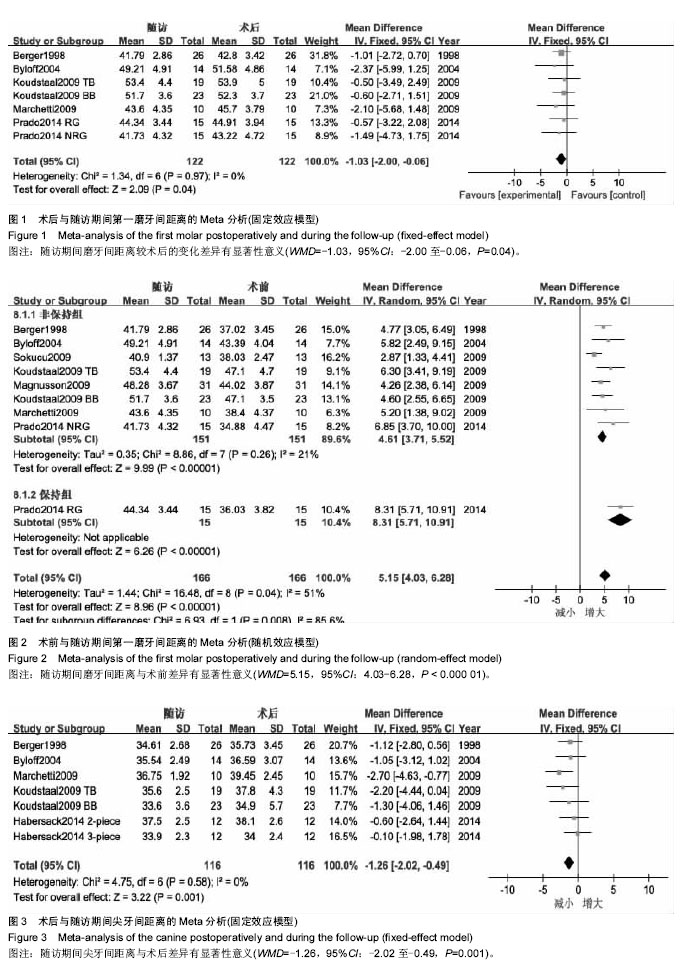
6个研究报道了尖牙间距离的长期变化[2,7,12-13,15,17]。
2.2.3 术后鼻气道改变的稳定性 因各研究间测量方法、选取的测量时间点不同,无法提取足够数据进行Meta分析,仅采用定性描述。3个研究在后前位头影测量片上对鼻底宽度进行了比较[8,13,17]。Berger等[17]选取鼻底最宽部位进行测量,SARME使鼻底宽度增加了约1.31 mm,随访1年无复发,效果稳定。Koudstaal等[13]的研究中选取的梨状孔最下点进行测量,骨支持式组和牙支持式组分别取得了2.4 mm和2.6 mm的扩展量,术后随访期间有少量复发,分别为1.0 mm和1.4 mm。Chamberland等[8]选取的测量点为鼻底双侧最凹点,术后扩展量约为1.4 mm,2年随访期间无显著性复发。Aras等[10]在锥形束CT上测量鼻底宽度,在尖牙区域截面鼻底宽度术后增加约4.68 mm,第一磨牙区域截面鼻底宽度增加约2.73 mm;并利用鼻声反射测量鼻前部最小横截面积和鼻腔容积、鼻后部最小横截面积和鼻腔容积,鼻前部最小横截面积及鼻腔容积、鼻后部最小横截面积及鼻腔容积术后分别增加0.47 cm2、2.29 cm3、0.81 cm2、6.99 cm3,1年随访期内均无显著复发。Magnusson[5]利用鼻腔测压测量了39例患者呼吸时的鼻气道阻力,并通过鼻声反射测量了鼻前部最小横截面积、鼻后部最小横截面积,扩弓3个月后鼻气道阻力明显降低,鼻前部最小横截面积、鼻后部最小横截面积明显增加,但18个月后,以上指标与手术前差异无显著性意义。其中23例患者术前主诉不同程度鼻塞,18个月后鼻后部最小横截面积的增加及主观鼻功能改善较术前差异仍有显著性意义。
| [1] Brown GVI, Epker BN, Wolford LM. Transverse maxillary deficiency dentofacial deformities:integrated orthodontic and surgical correction.St Louis:Mosby;1980.[2] Byloff FK, Mossaz CF. Skeletal and dental changes following surgically assisted rapid palatal expansion.Eur J Orthod. 2004;26(4):403-409. [3] Prado GP, Furtado F, Aloise AC, et al. Stability of surgically assisted rapid palatal expansion with and without retention analyzed by 3-dimensional imaging.Am J Orthod Dentofacial Orthop. 2014;145(5):610-616.[4] 聂萍,陶丽,唐艳梅,等. 手术辅助上颌快速扩弓对鼻气道形态和鼻阻力的影响[J].中国口腔颌面外科杂志,2015,13(2):147-150.[5] Magnusson A, Bjerklin K, Nilsson P, et al. Nasal cavity size,airway resistance,and subjective sensation after surgically assisted rapid maxillary expansion:a prospective longitudinal study.Am J Orthod Dentofacial Orthop. 2011;140(5):641-651.[6] Pereira-Filho VA, Monnazzi MS, Gabrielli MA, et al. Volumetric upper airway assessment in patients with transverse maxillary deficiency after surgically assisted rapid maxillary expansion.Int J Oral Maxillofac Surg. 2014;43(5):581-586.[7] Habersack K, Becker J, Ristow O, et al. Dental and skeletal effects of two-piece and three-piece surgically assisted rapid maxillary expansion with complete mobilization:a retrospective cohort study.J Oral Maxillofac Surg. 2014;72(11):2278-2288.[8] Chamberland S, Proffit WR. Short-term and long-term stability of surgically assisted rapid palatal expansion revisited.Am J Orthod Dentofacial Orthop. 2011;139(6):815-822.[9] Kurt G, Altug-Atac AT, Atac MS, et al. Stability of surgically assisted rapid maxillary expansion and orthopedic maxillary expansion after 3 years’ follow-up.Angle Orthod. 2010;80(4): 425-431.[10] Aras A, Akay MC, Cukurova I, et al. Dimensional changes of the nasal cavity after transpalatal distraction using bone-borne distractor:an acoustic rhinometry and computed tomography evaluation.J Oral Maxillofac Surg. 2010;68(7):1487-1497.[11] Al-Ouf K, Krenkel C, Hajeer MY, et al. Osteogenic uni- or bilateral form of the guided rapid maxillary expansion.J Craniomaxillofac Surg. 2010;38(3):160-165.[12] Marchetti C, Pironi M, Bianchi A, et al. Surgically assisted rapid palatal expansion vs. segmental Le Fort I osteotomy:transverse stability over a 2-year period.J Craniomaxillofac Surg. 2009; 37(2):74-78.[13] Koudstaal MJ, Wolvius EB, Schulten AJ, et al. Stability,tipping and relapse of bone-borne versus tooth-borne surgically assisted rapid maxillary expansion:a prospective randomized patient trial.Int J Oral Maxillofac Surg. 2009;38(4):308-315.[14] Sokucu O, Kosger HH, Bicakci AA, et al. Stability in dental changes in RME and SARME:a 2-year follow-up.Angle Orthod. 2009;79(2):207-213.[15] Magnusson A, Bjeklin K, Nilsson P, et al. Surgically assisted rapid maxillary expansion:long-term stability.Eur J Orthod. 2009;31(2):142-149.[16] Anttila A, Finne K, Keski-Nisula K, et al. Feasibility and long-term stability of surgically assisted rapid maxillary expansion with lateral osteotomy.Eur J Orthod. 2004;26(4):391-395.[17] Berger JL, Pangrazio-Kulbersh V, Borgula T, et al. Stability of orthopedic and surgically assisted rapid palatal expansion over time.Am J Orthod Dentofacial Orthop. 1998;114(6):638-645.[18] Northway WM, Meade JB. Surgically assisted rapid maxillary expansion:a comparison of technique,response,and stability. Angle Orthod. 1997; 67(4):309-320.[19] Stromberg C, Holm J. Surgically assisted,rapid maxillary expansion in adults.A retrospective long-term follow-up study. J Craniomaxillofac Surg.1995,23(4):222-227.[20] Bays RA, Greco JM. Surgically assisted rapid palatal expansion:an outpatient technique with long-term stability.J Oral Maxillofac Surg. 1992;50(2):110-113.[21] Pogrel MA, Kaban LB, Vargervik K, et al. Surgically assisted rapid maxillary expansion in adults.Int J Adult Orthodon Orthognath Surg. 1992;7(1):37-41.[22] Epker BN, Wolford LM. Transverse maxillary deficiency dentofacial deformities:integrated orthodontic and surgical correction.St Louis:Mosby;1980.[23] Timms DJ,Vero D. The relationship of rapid maxillary expansion to surgery with special reference to midpalatal synostosis.Br J Oral Surg. 1981;19(3):180-196.[24] Korn EL, Baumrind S. Transverse development of human jaws between the ages of 8.5 and 15.5 years,studied longitudinally with the use of implant.J Dent Res. 1990;69(6):1298-1306.[25] Deeb W, Hansen L, Hotan T, et al. Changes in nasal volume after surgically assisted bone-borne rapid maxillary expansion.Am J Orthod Dentofacial Orthop. 2010;137(6): 782-789.[26] Doruk C, Sokucu O, Bicakci AA, et al. Comparison of nasal volume changes during rapid maxillary expansion using acoustic rhinometry and computed tomography.Eur J Orthod. 2007; 29(3):251-255.[27] Laudemann K, Petruchin O, Nafzger M, et al. Long-term 3D cast model study:bone-borne vs. tooth-borne surgically assisted rapid maxillary expansion due to secondary variable.Oral Maxillofac Surg. 2010;14(2):105-114.[28] Landes CA, Laudemann K, Petruchin O, et al. Advantages and limits of 3-segmen(paramedian) versus 2-segment(median) surgically assisted rapid maxillary expansion(SARME).Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113(1):29-40.[29] Sygouros A, Motro M, Ugurlu F, et al. Surgically assisted rapid maxillary expansion:cone-beam computed tomography evaluation of different surgical techniques and their effects on the maxillary dentoskeletal complex.Am J Orthod Dentofacial Orthop. 2014;146(6):748-757.[30] Kilic E, Kilic B, Kurt G, et al. Effects of surgically assisted rapid palatal expansion with and without pterygomaxillary disjunction on dental skeletal structures:a retrospective review.Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115(2):167-174.[31] Laudemann K, Petruchin O,Mack MG, et al. Evaluation of surgically assisted rapid maxillary expansion with or without pterygomaxillary disjunction based upon preoperative and post-expansion 3D computed tomography data.Oral Maxillofac Surg. 2009;13(3):159-169.[32] Ergina PL, Cook JA, Blazeby JM, et al. Challenges in evaluating surgical innovation. Lancet. 2009;374(9695):1097-1104.[33] Tausche E, Hansen L, Hietschold V, et al. Three-dimensional evaluation of surgically assisted implant bone-borne rapid maxillary expansion:a pilot study.Am J Orthod Dentofacial Orthop. 2007;131(4 suppl):S92-99. |
| [1] | 姚晓玲, 彭建城, 许岳荣, 杨志东, 张顺聪. 可变角度零切迹前路椎间融合内固定系统治疗脊髓型颈椎病:30个月随访[J]. 中国组织工程研究, 2022, 26(9): 1377-1382. |
| [2] | 靖金鹏, 张 玥, 刘效敏, 刘 壹. 活血类中药注射剂预防骨科术后深静脉血栓形成的网状Meta分析[J]. 中国组织工程研究, 2022, 26(9): 1467-1476. |
| [3] | 刘 港, 马 超, 汪 乐, 曾 杰, 焦 勇, 赵 毅, 任敬佩, 胡传宇, 徐 林, 穆晓红. 踝足矫形器改善脑性瘫痪儿童运动功能:12项随机对照试验证据的Meta分析[J]. 中国组织工程研究, 2022, 26(8): 1299-1304. |
| [4] | 吴 敏, 张业廷, 王 璐, 王军威, 金 毓, 单继新, 白冰怡, 袁琼嘉. 同步训练序列对体成分及激素反应影响比较的Meta分析[J]. 中国组织工程研究, 2022, 26(8): 1305-1312. |
| [5] | 张璟琳, 冷 敏, 朱博恒, 汪 虹. 干细胞源外泌体促进糖尿病创面愈合的机制及应用[J]. 中国组织工程研究, 2022, 26(7): 1113-1118. |
| [6] | 安维政, 何 萧, 任 帅, 刘建宇. 肌源干细胞在周围神经再生中的潜力[J]. 中国组织工程研究, 2022, 26(7): 1130-1136. |
| [7] | 魏 兵, 常 山. 脊柱骨折矢状面不同角度置钉方式的有限元分析[J]. 中国组织工程研究, 2022, 26(6): 864-869. |
| [8] | 高文波, 马宗民, 李淑娴, 聂秀吉. 有限元分析不同骨质下种植体长度及直径对初期稳定性的影响[J]. 中国组织工程研究, 2022, 26(6): 875-880. |
| [9] | 李 杰, 张海涛, 陈锦伦, 叶鹏程, 张 华, 周本根, 赵长青, 孙友强, 陈建发, 向孝兵, 曾意荣. MRI矢状位和轴位测量前交叉韧带断裂与髌股关节的稳定性[J]. 中国组织工程研究, 2022, 26(6): 969-972. |
| [10] | 刘伊依, 邱俊强, 衣龙燕, 周财亮. 接受抗阻训练中老年人白细胞介素6与C-反应蛋白变化的Meta分析[J]. 中国组织工程研究, 2022, 26(5): 804-812. |
| [11] | 王 楠, 钱宇章, 谢 林. 不同针刺方法治疗腰椎间盘突出症的网状Meta分析[J]. 中国组织工程研究, 2022, 26(5): 813-820. |
| [12] | 陈晓旭, 罗雅馨, 毕浩然, 杨 琨. 脱细胞支架制备及其在组织工程和再生医学中的应用[J]. 中国组织工程研究, 2022, 26(4): 591-596. |
| [13] | 康坤龙, 王新涛. 生物支架材料促进骨髓间充质干细胞成骨分化的研究热点[J]. 中国组织工程研究, 2022, 26(4): 597-603. |
| [14] | 沈佳华, 付 勇. 基于石墨烯的纳米材料可否在干细胞领域应用[J]. 中国组织工程研究, 2022, 26(4): 604-609. |
| [15] | 张 通, 蔡金池, 袁志发, 赵海燕, 韩兴文, 王文己. 基于透明质酸的复合水凝胶修复骨关节炎软骨损伤:应用与机制[J]. 中国组织工程研究, 2022, 26(4): 617-625. |
中国组织工程研究杂志出版内容重点:组织构建;骨细胞;软骨细胞;细胞培养;成纤维细胞;血管内皮细胞;骨质疏松;组织工程
|
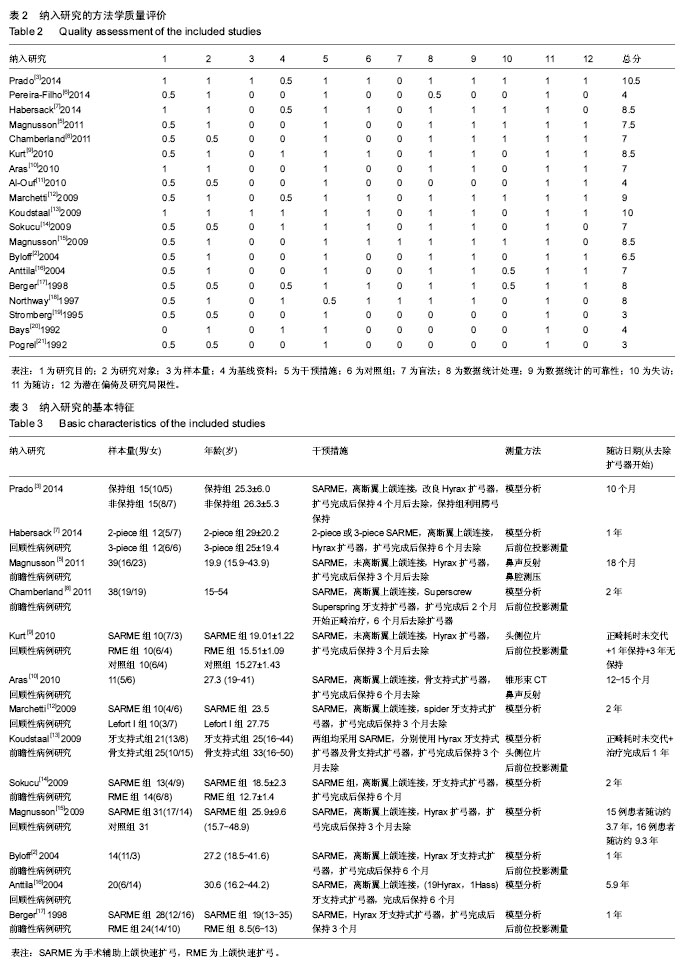
表1 方法学质量评价量表
Table 1 Methodological-quality scoring protocol
|
|
1.5 统计学分析 采用RevMan 5.3软件进行统计分析。该研究纳入的指标均为计量资料,当结局指标测量方法或单位一致时采用加权均数差(weighted mean difference,WMD),不相同时则采用标准化均数差(standardized mean difference,SMD),各效应量均以95%CI表示。研究间的异质性检验通过χ2评价,若I2 < 50%,则采用固位效应模型进行Meta分析,若I2 > 50%,则先分析产生异质性的原因,必要时进行亚组分析,若各研究间无明显临床异质性,则采用随机效应模型。对于异质性过大且无法判断其来源的研究则采用定性描述。
中国组织工程研究杂志出版内容重点:组织构建;骨细胞;软骨细胞;细胞培养;成纤维细胞;血管内皮细胞;骨质疏松;组织工程
中国组织工程研究杂志出版内容重点:组织构建;骨细胞;软骨细胞;细胞培养;成纤维细胞;血管内皮细胞;骨质疏松;组织工程
.jpg)
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||