Design
A retrospective case analysis.
Time and setting
Experiments were performed in the Center of Orthopedics, Haikou Municipal People's Hospital Affiliated to Xiangya School of Medicine, Central South University, from March 2006 to October 2011.
Subjects
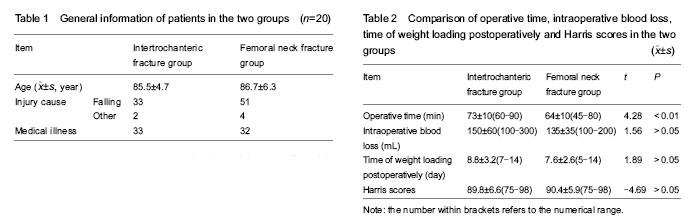
Ninety patients with hip fractures at the age of over 80 years were recruited from in the Center of Orthopedics, Haikou Municipal People's Hospital Affiliated to Xiangya School of Medicine, Central South University, from March 2006 to October 2011. There were 35 cases in intertrochanteric fracture group, aged 80-100 years (mean 85.5 ± 4.7 years). The intertrochanteric fracture was caused by falling in 33 cases and other causes in 2 cases; among them 21 cases were accompanied by medical illness. According to the Evans-Jensen type, 8 cases were classified as type I + II fracture and 27 cases as type III + IV fracture. There were 55 cases in femoral neck fracture group, aged 80-105 years (mean 86.7 ± 6.3 years). The femoral neck fracture was caused by falling in 51 cases and other causes in 4 cases; among them 32 cases were accompanied with medical illness. According to the Garden type, 11 cases were classified as type I + II fracture and 44 cases as type III + IV fracture. There was no significant difference in the age, medical illness, causes of fracture, and fracture type between the two groups (P > 0.05), the information were comparable.
Diagnostic criteria
The fractures were diagnosed by imaging examinations (X-ray or CT).
Inclusion criteria
(1) Patients aged ≥ 80 years. (2) Ipsilateral hip function was normal before injury. (3) Patients were in good general condition and could tolerate surgery. (4) Patients and their families were informed of the treatment and agreed.
Exclusion criteria
(1) Patients had a history of ipsilateral hip fracture or surgery. (2) Patients had surgical contraindications.
Methods
Prosthesis
All involved patients were treated using bipolar cemented handled prosthesis, 9 cases in intertrochanteric fracture group were treated using lengthened handled prosthesis.
Preoperative preparation
Patients were inquired of previous history after admission and received physical examination. Laboratory and conventional examinations were performed at Emergency Room. X-ray films at pelvic anteroposterior, hip anteroposterior, proximal femoral anteroposterior, and chest position were photographed. Blood vessels at the affected side were detected with ultrasound examination if necessary. Intertrochanteric fracture was detected with CT + three-dimensional examination. Preoperative risk assessment was performed and a consultation was suggested for patients with severe medical illness. Patients were treated with antibiotics 1 hour before surgery, to maximize blood drug concentration and prevent infection. Blood preparation was also carried out before surgery. Without any contraindications, preoperative preparations were performed, the affected limbs were immobilized to relax muscles, the fracture was fixed to correct hip varus deformity and achieve fracture alignment. Surgery is performed as early as possible after admission.
Surgical procedures
The cemented bipolar hemiarthroplasty was performed via the hip posterior-lateral approach among the involved patients under the lumbar anesthesia-epidural block anesthesia. An incision, 8-10 cm long, was made. The gluteus medius muscle attached in the femoral trochanter should be preserved. The joint capsule was cut via a T-shaped incision at 1.0-1.5 cm adjacent to the lesser trochanter. Intertrochanteric fractures were treated with two osteotomy surgeries: the first osteotomy was performed in the femoral neck to remove the femoral head and provide enough space for the following surgeries, then calcar femorale was subjected to anatomical reduction and the secondary osteotomy was performed on the bone template. The great and lesser trochanter fractures, as well as the attaching fascia were retained, after the great trochanter was anatomically repositioned, the reconstructed calcar femorale and proximal segment were fixed using steel wire or bone cement. As for femoral neck fractures, femoral neck was truncated with oscillating saw above the lesser trochanter, 1.5 cm lateral to the calcar femorale. During the surgery, medullary cavity was expanded and trimmed according to the osteoporotic conditions and the cavity size. The cemented prosthesis is placed at the anteversion angle of 15°, the contracting adductor should be released. After surgery, the affected limbs were fixed in the 15°-30° abduction position.
Postoperative processing
Patients were treated with antibiotics for 2-3 days postoperatively to prevent infection. The drainage tubes were removed within 24 hours to reduce the risk of retrograde infection. Deep vein thrombosis can be prevented through the following interventions: (1) intermittent compression system at the affected limbs, twice per day; (2) subcutaneous injection of low-molecular-weight heparin calcium 6 000 U, once per day, for 2-3 weeks or 10 mg rivaroxaban, once per day, for 2-3 weeks (rivaroxaban prevention therapy after September 2008). On day 1 postoperatively, patients were instructed to do quadriceps functional exercise and were informed of the range of motion, functional exercise followed the order of active + auxiliary → active → anti-resistance. At 1-2 weeks postoperatively, patients were allowed to get off the bend and resume weight-bearing activities by the support of nursing personnel. Hip flexion should be restricted (< 90°) within 6 months, hip adduction and rotation were forbidden.
Follow-up
The involved patients were followed up for 1-5 years postoperatively through regularly check (outpatient data, Harris score, X-ray plain film), phone visit and on-site visit.
Main outcome measures
(1) Biocompatibility to the host. (2) Operative time, intraoperative blood loss, time of weight loading postoperatively, Harris scores at last follow-up. (3) Complications.
Statistical analysis
Data were statistically analyzed using SPSS 13.0 software (SPSS, Chicago, IL, USA). Measurement data were expressed as the mean ± SD. The difference between the two samples was compared using normal distribution test and homogeneity of variance test, then t test was performed if data met normal distribution and non-parametric rank rum test was performed if data did not meet normal distribution. Count data were compared using chi-square test. A P < 0.05 level was considered statistically significant and P < 0.01 was extremely significant difference.