中国组织工程研究 ›› 2021, Vol. 25 ›› Issue (15): 2334-2340.doi: 10.3969/j.issn.2095-4344.3823
• 数字化骨科 digital orthopedics • 上一篇 下一篇
胫后肌腱转位治疗足下垂的有限元分析
何少波1,刘继超1,杨立峰1,丁永峰2,李伍建1
- 1西安交通大学附属3201医院骨科,陕西省汉中市 723000;2重庆文理学院,重庆市 402160
Finite element analysis of transposition of posterior tibial tendon for foot drop
He Shaobo1, Liu Jichao1, Yang Lifeng1, Ding Yongfeng2, Li Wujian1
- 1Department of Orthopedics, 3201 Hospital Affiliated to Xi'an Jiaotong University, Hanzhong 723000, Shaanxi Province, China; 2Chongqing University of Arts and Sciences, Chongqing 402160, China
摘要:
文题释义:
胫后肌腱转位手术:将胫后肌腱自止点处切断,穿过胫腓骨骨间膜或踝关节皮下隧道,重新固定在楔骨上,以加强踝关节背伸能力,改善足下垂状态,通常用于治疗腓总神经不可逆性损害所致足下垂。
表面肌电信号(surface electromyography,sEMG):是肌肉收缩时伴随的电信号,是在体表无创检测肌肉活动的重要方法,其电位变化的振幅与肌肉负荷大小存在相关性。表面肌电信号的应用背景主要集中在康复医学和体育科学两大领域,也用于模式识别等生物医学工程领域。
背景:胫后肌腱转位作为治疗腓总神经不可逆性损害所致足下垂的金标准,对其临床疗效研究报道甚多,但一直缺少详细的有限元受力分析。
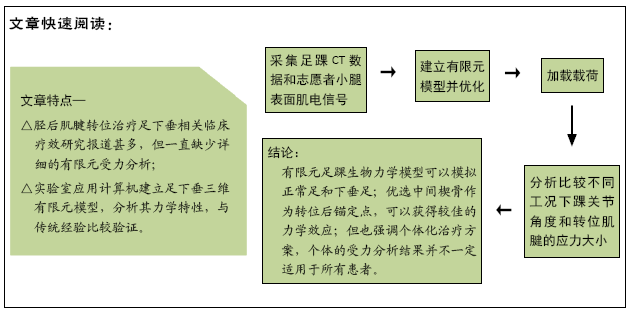
目的:建立腓总神经损伤所致足下垂三维有限元模型,分析力学特性,并与传统经验相互验证。
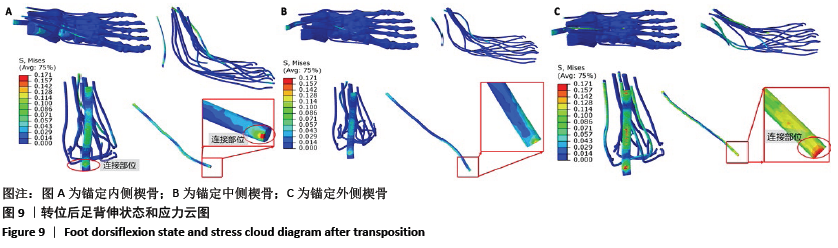
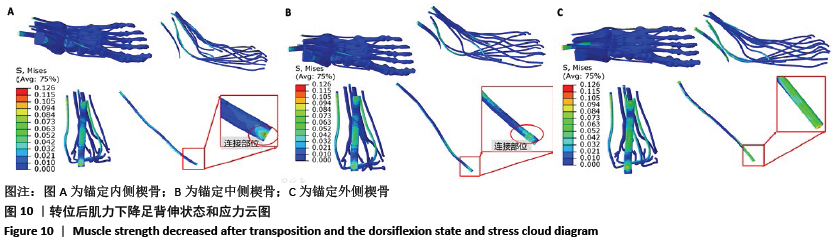
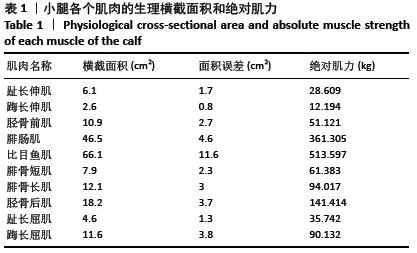
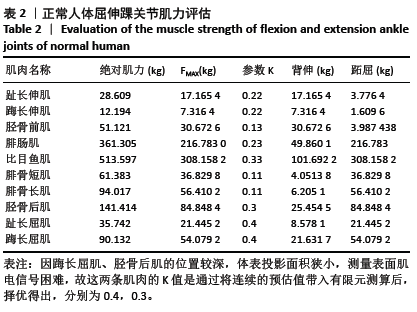
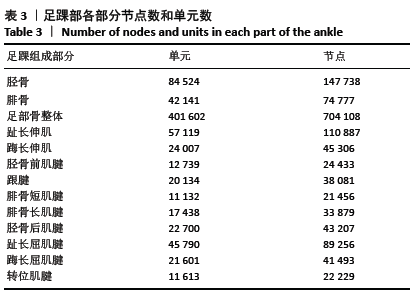
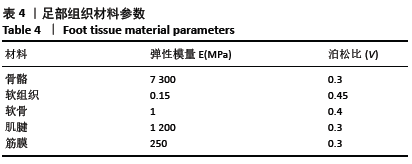
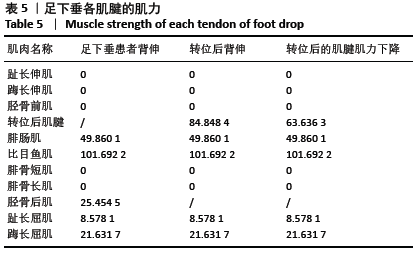
方法:①导入1例左侧腓总神经损伤导致左侧足下垂男性患者的足踝部CT数据,运用MIMICS、Cero、Abaqus、ANSYS等一系列软件重建足踝部骨骼;②选择10位受试者,测量计算出表面肌电信号的均方根幅值RMS,对肌力大小进行预估;③赋予各个部分的材料参数,得出具有正常足的有限元模型,模拟腓总神经完全损伤所致的足下垂畸形状态;④在此基础上,对胫后肌腱转位,锚定点分别确定为内、中、外侧楔骨,转位肌腱将足固定于背伸10°位,且转位后胫后肌肌力下降一级;⑤对3个不同锚定位置的2次下垂状态进行有限元受力分析,分别计算这9种工况下的踝关节背屈、内外翻角度以及转位肌腱的最大应力。研究方案的实施符合西安交通大学附属3201医院的相关伦理要求。所有受试者均对试验过程完全知情同意。
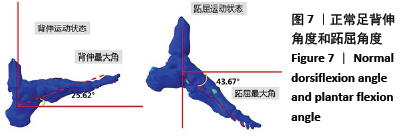
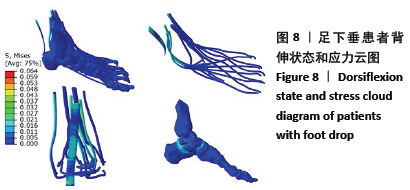
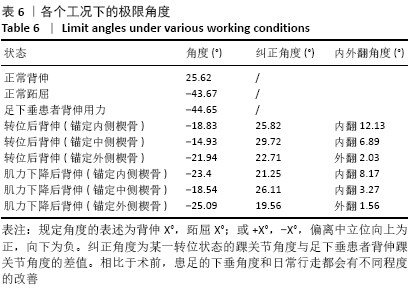
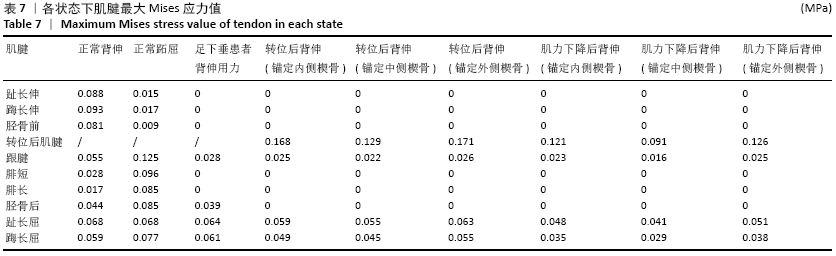
结果与结论:①正常足模型的背伸、跖屈角度均接近且小于极限角度(背伸25.62°<27°,跖屈43.67°<45°);下垂足模型背伸状态的背伸角度为-44.65°,与研究对象的背伸角度-47°相比,较为接近;②纠正足下垂畸形的效果最明显、肌腱所受应力最小的是锚定中间楔骨;纠正足下垂畸形的效果最差、肌腱所受应力最大、有轻度外翻踝作用的是锚定外侧楔骨;具有内翻踝作用的是锚定内侧楔骨;③转位后肌腱的应力集中点在肌腱与骨接触的锚定点附近;④结果说明,有限元建立的足踝生物力学模型可以初步模拟正常足和腓总神经完全损伤源性的下垂足;治疗足下垂畸形时,优选中间楔骨作为转位后锚定点,可以获得较佳的力学效应。此结论与传统手术经验相符合,但也强调个体化治疗方案,个体的受力分析结果并不一定适用于所有患者。
中图分类号: