中国组织工程研究 ›› 2017, Vol. 21 ›› Issue (35): 5709-5714.doi: 10.3969/j.issn.2095-4344.2017.35.022
• 骨与关节图像与影像 bone and joint imaging • 上一篇 下一篇
基于三维重建CT的骨盆髋臼一干三枝分型法在修复治疗中的应用
陈 华1,2,李 峰1,2,徐阳平1,2
- 1湖北省中医院,湖北省武汉市 430061;2湖北省中医药研究院,湖北省武汉市 430074
Application of the “one trunk-three branches” classification based on three-dimensional CT reconstruction in the treatment of pelvic and acetabular fractures
Chen Hua1, 2, Li Feng1, 2, Xu Yang-ping1, 2
- 1Hubei Provincial Hospital of Traditional Chinese Medicine, Wuhan 430061, Hubei Province, China; 2Hubei Province Academy of Traditional Chinese Medicine, Wuhan 430074, Hubei Province, China
摘要:
文章快速阅读:
.jpg)
文题释义:
三维重建CT:通过运用表面遮盖法、最大密度投影法、多平面重建法等技术手段,对二维CT的影像数据进行分析处理,最终生成高质量的三维图像。由此产生的CT三维图像直观、立体、空间立体感强,能够清晰显示各自的解剖关系和毗邻关系,能为临床工作提供更多更全面更准确的有价值的信息,能弥补普通X射线平片和常规CT扫描的不足。
一干三枝分型:基于三维重建CT的骨盆髋臼一干三枝分型法。将完整的骨盆髋臼分为一干和三枝。干:耻骨联合、界线、骶骨;三枝:髂枝、方形枝、后壁枝。具体在临床中可见这4种骨折类型:①单干或者单枝骨折(单干,单髂枝,单方形枝,单后壁枝);②一干一枝骨折(一干合并髂枝骨折,一干合并方形枝骨折,一干合并后壁枝骨折);③一干二枝骨折(一干合并髂枝和方形枝骨折,一干合并髂枝和后壁枝骨折,一干合并方形枝和后壁枝骨折);④一干三枝骨折(一干合并髂枝、方形枝和后壁枝骨折)。
摘要
背景:目前尚未有一种系统的分型法能完全、精确、直观地反映骨盆髋臼骨折的特点。螺旋三维重建CT技术为诊断骨盆髋臼骨折提供了直观、全面的影像学资料。
目的:介绍基于三维重建CT的骨盆髋臼骨折一干三枝分型法,并评价其在指导临床修复手术中的作用。
方法:纳入47例骨盆髋臼骨折患者,根据一干三枝分型法,18例单干或者单枝骨折,18例一干一枝骨折,7例一干二枝骨折,4例一干三枝骨折。根据一干三枝分型法选择修复方案:手术入路可分为改良的Stoppa入路、髂腰三角固定后入路、髂窝入路和K-L入路,术中选用一种或者多种联合;入路及固定顺序:先干后枝,若相连的枝已同时复位,无需另选入路及固定,如果没有复位,可能存在旋转,需另选入路及固定。术后随访评价临床效果。
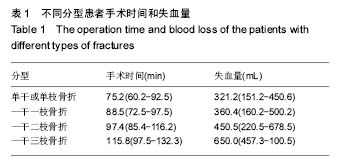
结果与结论:①单干或者单枝骨折、一干一枝骨折、一干二枝骨折、一干三枝骨折的平均手术时间分别为75.2,88.5,97.4,115.8 min,平均失血量分别为321.2,360.4,450.5,650.0 mL;②骨盆骨折术后复位优良率按Matta标准评定:优18例,良27例,可1例,差1例,优良率为96%;髋臼骨折术后复位满意率按Matta标准评定:解剖复位25例,满意复位20例,不满意复位2例,满意率为96%;③所有骨折随访12-35个月,随访率为87%,所有骨盆髋臼骨折平均愈合时间为2.9个月(2.7-4.2个月),平均完全负重时间为3.8个月(2.5-5.6个月);④末次随访时骨盆骨折术后疗效评定按照Majeed量化评分评定:优16例,良25例,可4例,差2例,优良率为87%;末次随访时髋关节功能疗效评定按照改良d'Aubigne和Postel评分标准评定:优15例,良24例,可6例,差2例,优良率为83%。无术后并发症发生;⑤结果表明,基于三维重建CT的骨盆髋臼一干三枝分型在指导骨盆髋臼骨折治疗方法的选择上具有重要意义,有助于指导选择选择手术入路和入路及固定顺序,从而提高骨盆髋臼骨折的治疗效果。
中图分类号:

.jpg)
.jpg)