Chinese Journal of Tissue Engineering Research ›› 2023, Vol. 27 ›› Issue (36): 5891-5897.doi: 10.12307/2023.718
Previous Articles Next Articles
Relationship between the degeneration of paraspinal muscle and sagittal alignment
Liu Ziwen1, 2, Yang Yuming1, 2, Xie Hongru3, Zhang Zepei1, Xu Haoxiang1, Miao Jun1
- 1Second Department of Spine, Tianjin Hospital, Tianjin 300210, China; 2Clinical College of Orthopedics, Tianjin Medical University, Tianjin 300203, China; 3Yuncheng Central Hospital, Yuncheng 044099, Shanxi Province, China
-
Received:2022-09-28Accepted:2022-11-11Online:2023-12-28Published:2023-03-27 -
Contact:Miao Jun, Chief physician, Doctoral supervisor, Second Department of Spine, Tianjin Hospital, Tianjin 300210, China -
About author:Liu Ziwen, Master candidate, Second Department of Spine, Tianjin Hospital, Tianjin 300210, China; Clinical College of Orthopedics, Tianjin Medical University, Tianjin 300203, China -
Supported by:Natural Science Foundation of Tianjin City, No. S20ZDD484 (to MJ)
CLC Number:
Cite this article
Liu Ziwen, Yang Yuming, Xie Hongru, Zhang Zepei, Xu Haoxiang, Miao Jun. Relationship between the degeneration of paraspinal muscle and sagittal alignment[J]. Chinese Journal of Tissue Engineering Research, 2023, 27(36): 5891-5897.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
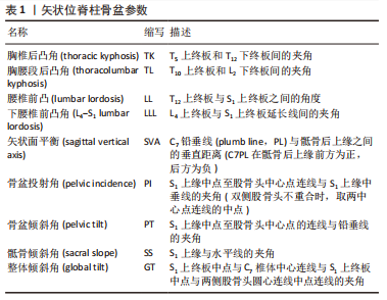
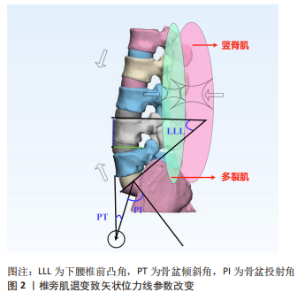
2.1 椎旁肌退变的机制及评价方法 关于椎旁肌退变的机制,首先在形态学上,椎旁肌的退变包括萎缩和变性,即肌肉容积减少(以肌纤维量和体积的减少为特征)和脂肪浸润(肌肉被脂肪组织渗透代替);而在细胞水平,可发生肌节溶解、内皮细胞退化、线粒体数量明显减少等改变,除此之外还会出现结缔组织增加、毛细血管密度下降等组织学改变[17-18]。 根据椎旁肌的退变在形态学上的改变可以得到较好的观测和比较,故对于椎旁肌退变的评价,最常用的就是影像学工具[19-20]。其中MRI具有良好的软组织分辨率,其测量肌肉横截面积(cross sectional area,CSA)及脂肪浸润程度在测量者间及测量者内均具有极好的可信度[21]。SIONS等[22]认为可以采用相对肌肉横截面积(relative muscle cross-sectional area,rmCSA/RCSA),即肌肉总CSA减去肌内脂肪CSA,可以同时评估肌肉质和量。近年来,随着对肌肉退变原理的理解深入,一些新型技术也被用于椎旁肌的研究中。生物阻抗分析在分析全身骨骼肌质量如何影响脊柱排列有着新的发现[23-24]。表面肌电监测患者躯干肌群肌肉活动的整体功能和状态时,具有无痛无创、操作方便、结果可储存等特点[25]。不同于影像学资料直观、静态地对肌肉容积进行观察,表面肌电可以在肌肉进行活动时记录神经肌肉的运动信息,并进行时域、频域分析。脊柱退行性变的患者往往可以通过表面肌电得到椎旁肌耐力下降、多肌群活动失调、肌电活动不对称、肌肉激活时序改变以及屈曲放松现象缺少等异常检查结果[25-29]。 2.2 椎旁肌和脊柱矢状位力线的关系 现阶段有关脊柱退行性病变患者的研究中,往往考虑了脊柱矢状位力线改变与椎旁肌退变两方面的因素,因此将对此进行总结分析。相关脊柱骨盆参数详见表1。"
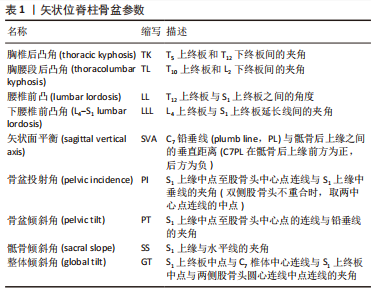
2.2.1 椎旁肌的退变情况和矢状位力线均受年龄、种族等因素影响 年龄的衰老往往伴随着体质的下降和肌肉的退变[30]。在一项对50例未接受手术的退行性脊柱疾病老年患者的研究中,JUN等[2]证实了椎旁肌的脂肪变性与体脂百分比增加以及体质恶化显著相关。同时,椎旁肌(包括多裂肌、竖脊肌等)的完整性在维持适当的矢状位平衡和整体脊柱排列情况方面起着至关重要的作用。一项对36名日本中年和老年妇女的对比研究也表明,竖脊肌肌肉厚度减少是胸椎后凸角增加的重要影响因素,而腰大肌厚度的减少与骶骨前倾增加相关[31]。 在胡宗杉等[32]的一项关于中国正常成年人脊柱-骨盆矢状位形态的多中心研究中,研究者将786名正常成年人按年龄分层后发现,自40岁组至80岁组腰椎前凸角、下腰椎前凸角、腰椎前凸分布指数(腰椎前凸角和下腰椎前凸角的比值)随着年龄的增加而降低,骨盆投射角-腰椎前凸角、整体倾斜角和SVA随着年龄增长明显升高。说明随着年龄的增长,正常情况下机体的整体矢状位形态呈退变进程。对于如何评价个体的骨盆参数是否合适,不同的研究员给出的结论也不尽相同,近来YILGOR等[1]研究者为了预测矫形术后力学并发症的发生率设计了脊柱整体形态与平衡评分,该评分提出以骨盆投射角为基准,来确定其他脊柱骨盆参数的理想值相对骨盆投射角的关系。马鸿儒等[33]认为脊柱整体形态与平衡评分并不适合中国老年人,于是在脊柱整体形态与平衡的基础上考虑年龄与人种因素,选取50-70岁中国健康志愿者的数据来计算理想值,可以更适用于实际临床工作中该年龄组的患者。 在一项综合了椎旁肌质量、退变性疾病严重程度、脊柱骨盆参数等多项指标与年龄的相关性分析中,表示椎旁肌质量的平均脂肪浸润与年龄密切相关(r=0.602,P < 0.001);退变性疾病严重程度(r=0.445,P < 0.001)、骨盆投射角(r=0.472,P < 0.001)、骨盆倾斜角(r=0.424,P < 0.001)、骨盆投射角-腰椎前凸角(r=0.397,P < 0.001)与年龄呈中度相关;骶骨倾斜角与年龄相关性较弱(r=0.162,P=0.038);腰椎前凸角与年龄无关(r=0.001,P=0.986)[3]。这提示在关注椎旁肌退变和矢状位力线改变相关性的同时也要关注年龄等因素的影响,必要时可采用调整年龄等因素后的Spearman相关系数评估参数之间的相关性[3]。 2.2.2 椎旁肌退变和脊柱骨盆参数改变的关系 脊柱退行性变患者常伴随着椎旁肌的退变。以退行性腰椎侧凸为例,由于椎体不对称压缩,腰椎间盘和关节突关节的不对称退变,腰椎稳定性受到破坏,引起侧凸椎体侧方位移,在退变过程中为了对抗脊柱失平衡,腰椎前屈和背伸肌群产生着不同的生理效应,导致肌肉能量消耗增加,引起疼痛、疲劳及萎缩[17]。目前有很多研究均表明椎旁肌的退变和脊柱骨盆参数异常有关[16,19-20,23,34-45]。 研究之间结果类似,即脊柱骨盆参数异常的患者,椎旁肌脂肪浸润程度值升高,CSA (包括rmCSA)减低,呈退变性改变。同样在立位负重条件下,脊柱畸形患者L1-L2(上腰椎)和L4-L5(下腰椎)区的肌肉疲劳程度较正常人更严重,肌电信号表现为中值频率的下降[46]。 除了上述在脊柱退变性疾病的患者与正常人群间的椎旁肌质量比较研究可以看出椎旁肌退变和脊柱骨盆参数改变存在关联,研究员们继续对脊柱不同退变程度的患者进行了深入研究。在YAGI等[34]开展的针对退变性腰椎侧凸患者的相关研究中发现,左右侧腰大肌和多裂肌的不对称程度与脊柱骨盆参数及患者的侧凸Cobb角改变程度呈正相关,证明椎旁肌与整体脊柱力线的退变程度间具有相关性。KATSU等[47]在探究椎旁肌组织在邻近节段退变患者维持脊柱骨盆排列中的作用时,进行了椎旁肌rmCSA与脊柱盆腔参数的相关性分析,结果表明邻近节段退变患者的骨盆倾斜角/骶骨倾斜角和多裂肌/竖脊肌间呈显著正相关。但作者也提出需要进一步的研究来阐明椎旁肌的退变是骨盆排列失调的原因抑或是结果。在2022年一项探讨腰椎管狭窄症患者椎旁肌质量测量值与脊柱盆腔矢状面参数对矢状面平衡的预测价值的大样本量回顾性研究中,测量了110例患者的椎旁肌总横截面积、功能横截面积等椎旁肌质量数据,并用Pearson相关分析研究椎旁肌测量值与矢状面参数之间的相关性,得出总横截面积与腰椎前凸角(r=0.455,P < 0.01)和骨盆投射角-腰椎前凸角(r=-0.286,P < 0.01)显著相关;功能横截面积与腰椎前凸角(r=0.326,P < 0.01)和骨盆投射角-腰椎前凸角(r=-0.209,P < 0.05)均有显著相关性,即较好的椎旁肌质量与脊柱骨盆参数的维持有关[48]。 除了较常讨论的腰段脊柱,颈胸段同样存在这种相关性。在一项探讨了颈椎后路融合术后颈胸段矢状位脊柱参数与颈椎旁肌质量间关系的回顾性研究中,根据双侧颈半棘肌肌肉质量减少的严重程度比较不同亚组之间的颈椎矢状位参数,术后3个月至1年随访,中-重度双侧颈半棘肌减少组C2倾斜角和SVA的变化明显大于轻度双侧颈半棘肌减少组[19]。同样SHIMIZU等[49]证实在颈椎椎板成形术后,切除颈椎半棘肌的患者C2-7 Cobb角较保留颈椎半棘肌的患者显著减小,同时切除颈椎半棘肌的患者由于进行性的矢状位力线的退变,会逐渐在寰枢椎交界处增加异常的机械应力,更易导致齿状突后假瘤的发生(P < 0.001)再一次验证这种相关性存在。 此外PARK等[40]的一项对比研究中考虑椎旁肌的退行性变是脊柱退行性畸形的危险因素,同时对比发现肌肉减少症不是危险因素,即脊柱矢状面不平衡是受孤立的椎旁肌变性影响,而非受全身肌肉影响。为了深入研究以明确细化单个椎旁肌的作用,XIA等[39]对腰椎退行性后凸患者从L1/2到L5/S1每个腰椎水平的不同椎旁肌进行分析,发现多裂肌的rmCSA在多节段和胸椎后凸角呈负相关,在L4/5水平与腰椎前凸角呈正相关,竖脊肌在L3/4和L4/5水平的rmCSA与骨盆投射角呈正相关,此结果提示特定脊柱水平的个别肌肉变性影响矢状面脊柱畸形的进程。此外多裂肌和腰肌的rmCSA从L1/2增加到L5/S1,而竖脊肌的rmCSA减少;下腰椎水平竖脊肌的rmCSA低于多裂肌和腰肌,而上腰椎水平则相反,这表明相对于多裂肌和腰肌,从L1/2到L5/S1的竖脊肌退变逐渐加重。下腰椎水平的竖脊作用严重丧失,这一结果和最近的类似研究一致[50],进一步说明多裂肌和竖脊肌在维持矢状面脊柱-盆腔平衡方面有不同的作用。 同时,考虑到两侧椎旁肌可能存在不对称性退变,可能与退行性腰椎侧凸的发展存在联系。腰椎侧凸除了会导致冠状面各个脊柱参数的改变,也会影响到矢状面的脊柱骨盆参数,目前也有研究者注意到了这一点[12,34]。LEE等[51]发现,腰椎除了同一水平上凸侧和凹侧椎旁肌的退变程度不同之外,不同区域的肌肉退行性变的速度也存在不同,背伸肌组退变更为明显,且始于下腰椎水平,逐渐向上发展。而XIA等[39]在明确脊柱退行性改变所致的脊柱骨盆参数改变的情况下,探究了不同水平椎旁肌的退变程度,得出了与上腰椎相比下腰椎椎旁肌退变程度更高的结论,同时其他研究者也得出相似的结果[50,52]。故综合了退变速率和退变程度两个方面,在柱骨盆参数改变的情况下,下腰椎水平椎旁肌的退变情况要更为严重。 2.2.3 椎旁肌退变和矢状位平衡失稳的关系 矢状位平衡情况可以通过SVA来判断。SVA的测量为S1后上缘与经C7椎体中心所作的铅垂线之间的偏移量,通常认为矢状位的失衡为SVA超过± 50 mm。在脊柱发生退行性改变时,机体可以通过控制椎旁肌来改变脊柱骨盆参数的代偿机制,达到维持矢状位平衡的目的,如胸椎后凸减少、骨盆后倾或旋转、髋部伸展,甚至膝关节屈曲等[53-54]。但这种代偿机制存在弊端,以骨盆后倾增加为例,骨盆倾斜角和行走障碍(walking disability)之间呈显著正相关,即高骨盆倾斜角影响行走的效率,产生疼痛[55]。此外代偿有一定限度,JACKSON等[56]证实,如果SVA没有被代偿机制改善,受试者会产生背痛。其他类似研究也提示高骨盆倾斜角和高SVA会加重腰痛和病情进展[57-58]。TAKAHASHI等[59]在分析了409名社区老年人的数据后,发现胸椎后凸角与背部肌力呈负相关,背部的良好肌力可通过代偿机制降低SVA恶化的风险。 在明晰椎旁肌通过代偿机制与矢状位平衡相关联后,随着椎旁肌的退变加重,椎旁肌的代偿能力下降,会导致矢状位平衡的失稳。在一项纳入171例入院腰椎管狭窄症患者和100名来自社区的健康对照组的前瞻性研究中,先对试验组对象进行椎旁伸肌耐力试验,并根据椎旁肌状态由差至好分为3组(1级、2级和3级)[16];1级组腰椎前凸角明显低于其他两组(P < 0.05),SVA明显高于其他两组(P < 0.05)。大样本量的研究也证明了这种相关性,2019年的一项多中心横断面研究探究了躯干肌质量与脊柱矢状面失平衡的关系,在分析了2 551例患者的躯干肌质量和SVA等数据后,发现躯干肌肉质量与SVA呈负相关(P < 0.000 1),同时当躯干肌肉质量从约23 kg开始下降时,SVA开始增加[57]。 另一项研究在形态学上得出椎旁肌脂肪变性与老年人SVA密切相关[40]。此外YIN等[60]认为相较于单次测得的SVA,步行10 min后再次测量可以检测出隐匿的矢状面失衡。因为患者在静息状态下椎旁肌已经被调动来对抗向前不平衡的趋势[61],一旦运动时椎旁肌疲劳,代偿机制被消耗,SVA便会显著恶化。这种情况被称为动态矢状面不平衡,同时YIN等[60]通过实验为动态矢状面不平衡的诊断提供了一种较好的评价标准。 2.3 脊柱退行性病变进程中椎旁肌和矢状位力线相互影响的机制探究 2.3.1 矢状位力线不良是决定椎旁肌异常激活的重要解剖因素 如上文,骨盆参数包括解剖参数骨盆投射角及姿势参数——骨盆倾斜角和骶骨倾斜角,其中成年后的骨盆投射角不受体位姿势的影响,骨盆投射角定义了骶骨相对于髂骨的相对方向,而骶骨倾斜角和骨盆倾斜角是随着骨盆绕髋轴旋转而变化的动力学参数。有生物力学的研究证实,脊柱骨盆参数的不同与脊柱负荷和肌肉激活不同有关[62]。一般认为骨盆投射角值较大的个体需要通过控制多裂肌等椎旁肌,形成较大的腰椎前凸才能维持直立,所以高骨盆投射角常被报道为正矢状位错位的危险因素[63-66]。这里以骨盆投射角值为例,分析矢状位力线对椎旁肌的影响。HONG等[67]发现,成人脊柱侧凸患者的骨盆投射角值大于对照组,且随侧凸程度增加骨盆投射角平均值增大。LABELLE等[68]的一项关于腰椎滑脱的研究也验证,低度滑脱组的骨盆投射角值明显低于高度滑脱组的平均值。在李方财等[69]的一项研究中,将110例腰椎退行性侧凸患者根据腰椎前凸角和胸腰段后凸角等矢状位参数的变化程度从轻到重分为Ⅰ、Ⅱ、Ⅲ型,其中Ⅲ型患者的骨盆投射角值和骨盆倾斜角值明显低于其他两组,而矢状位失平衡发生率高于其他两组;研究结果考虑为Ⅲ型(严重组)患者骨盆投射角值小,可提供骨盆倾斜角值的变化范围小,从而相较下更容易出现矢状位失平衡。一般状态下,人体可以改变骶骨倾斜角和骨盆倾斜角以获得合适的矢状位力线。即当脊柱出现向前倾斜的倾向时,人体可以通过控制骨盆后倾来进行代偿,此时骶骨倾斜角值降低(骶骨转为垂直),骨盆倾斜角值提高(骨盆以髋关节为中心向后旋转),使得重心重新后移,矢状位再次平衡[70-71]。由于骨盆投射角的值等于骶骨倾斜角与骨盆倾斜角的和,所以对于个体而言,骨盆投射角值的大小决定了骨盆倾斜角和骶骨倾斜角的改变范围,即对抗矢状位失平衡的能力。 同时一些研究者探究了不同类型的矢状位平衡失稳是否会影响脊柱肌肉的激活。BASSANI等[72]组合了无症状成人的4个解剖参数(骶骨倾斜角、骨盆投射角、SVA和4种Roussouly腰骶部矢状面分型)的变化,共模拟出站立状态下2 772种脊柱盆腔构型的肌肉骨骼模型以进行生物力学分析。在肌肉激活方面,SVA前向不平衡组(SVAfront)的构型在所有的4种Roussouly腰骶部矢状面分型中通常导致多裂肌肌力增加,而SVA后向不平衡组(SVAback)的构型多裂肌肌力未产生显著变化,但竖脊肌和腹直肌的力量分别在SVAfront和SVAback姿势中被异常激活。这其实较易理解,当出现脊柱矢状位力线的前向不平衡时,同为躯干伸肌的竖脊肌额外增加肌力,以抵消躯干质量的转移,尽管力量较低;相反,腹直肌被异常激活以抵消向后不平衡的趋势。 2.3.2 椎旁肌通过代偿机制持续影响矢状位力线 在腰椎椎旁肌群中,多裂肌有着肌束多、附着面积最大、肌纤维较短、距离中轴距离最近等特点,在正常情况下两侧多裂肌同时收缩时,椎体将在矢状面上向后旋转,对腰椎前凸角的维持起主要作用[73-75]。在退变性腰椎侧凸等疾病进展中,由于椎间盘及小关节的退变,腰椎前凸角的丢失往往是最早发生改变的脊柱骨盆参数。此时多裂肌的退变受腰椎侧凸影响较小,弓弦效应不明显,多裂肌退变的触发主要是由于腰椎前凸的变化;退变的发展是由于其长期高负荷收缩的代偿工作。通过代偿来减少由于腰椎前凸变小所致的整体脊椎向前倾斜的倾向,维持矢状位平衡[76-77]。 由于多裂肌长期处于异常激活和高负荷状态,可出现萎缩变性等改变[9]。且当多裂肌出现萎缩变性时,原有的代偿平衡再次被打破,脊柱再次出现向前倾斜的倾向,导致腰椎前凸减少(腰椎前凸角或下腰椎前凸角)、骶骨倾斜角减小、骨盆倾斜角增大等矢状位力线参数的恶化伴随着多裂肌的退变持续下去(图2)。"
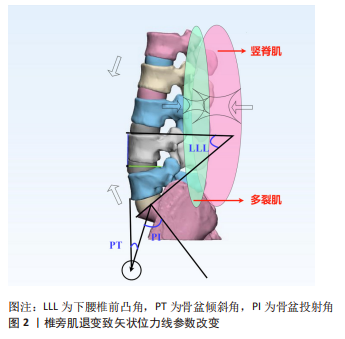

此外代偿机制可以拓展至其他位于脊柱背侧的椎旁肌。丁浚哲等[12]的一项回顾性研究中提出腰椎前屈和背伸肌群存在不同的解剖结构和生理效应,背伸肌群在拮抗退变性腰椎侧凸进展中具有重要作用。在YAGI等[78]关于腰椎退行性后凸患者椎旁肌退变情况的研究中表明,下腰椎椎旁肌表现为多裂肌CSA降低,脂肪浸润面积增大,先明确腰椎退行性后凸患者多裂肌出现退变。同时在与其他邻近节段退变患者相比,多裂肌和腰大肌比值降低,由于腰椎退行性后凸组患者没有冠状畸形,屈曲肌群受弓弦效应较其他邻近节段退变患者影响小,考虑背伸肌群存在独立的退行性变和容积损失。以上实验证实解剖及代偿因素在多裂肌等椎旁肌的退变中具有重要作用。"

| [1] YILGOR C, SOGUNMEZ N, BOISSIERE L, et al. Global Alignment and Proportion (GAP) Score Development and Validation of a New Method of Analyzing Spinopelvic Alignment to Predict Mechanical Complications After Adult Spinal Deformity Surgery. J Bone Joint Surg Am. 2017;99(19):1661-1672. [2] JUN HS, KIM JH, AHN JH, et al. The Effect of Lumbar Spinal Muscle on Spinal Sagittal Alignment: Evaluating Muscle Quantity and Quality. Neurosurgery. 2016;79(6):847-855. [3] ZHANG Y, MANDELLI F, MÜNDERMANN A, et al. Association between fatty infiltration of paraspinal muscle, sagittal spinopelvic alignment and stenosis grade in patients with degenerative lumbar spinal stenosis. N Am Spine Soc J. 2021;5:100054. [4] LOWE T, BERVEN SH, SCHWAB FJ, et al. The SRS classification for Adult Spinal Deformity - Building on the King/Moe and Lenke Classification Systems. Spine. 2006;31(19):S119-S125. [5] SCHWAB F, FARCY JP, BRIDWELL K, et al. A clinical impact classification of scoliosis in the adult. Spine. 2006;31(18):2109-2114. [6] BESS S, SCHWAB F, LAFAGE V, et al. Classifications for Adult Spinal Deformity and Use of the Scoliosis Research Society-Schwab Adult Spinal Deformity Classification. Neurosurg Clin North Am. 2013;24(2):185-193. [7] KALICHMAN L, CARMELI E, BEEN E. The Association between Imaging Parameters of the Paraspinal Muscles, Spinal Degeneration, and Low Back Pain. Biomed Res Int. 2017;2017:2562957. [8] ASAI Y, TSUTSUI S, OKA H, et al. Sagittal spino-pelvic alignment in adults: The Wakayama Spine Study. Plos One. 2017;12(6):e0178697. [9] HE K, HEAD J, MOUCHTOURIS N, et al. The Implications of Paraspinal Muscle Atrophy in Low Back Pain, Thoracolumbar Pathology, and Clinical Outcomes After Spine Surgery: A Review of the Literature. Global Spine J. 2020;10(5):657-666. [10] CHO Y. Evaluation of Global Sagittal Balance in Koreans Adults. J Korean Neurosurg Soc. 2017;60(5):560-566. [11] MCDOWELL MM, TEMPEL ZJ, GANDHOKE GS, et al. Evolution of Sagittal Imbalance Following Corrective Surgery for Sagittal Plane Deformity. Neurosurgery. 2017;81(1):129-134. [12] 丁浚哲, 鲁世保, 孔超, 等. 退变性腰椎侧凸椎旁肌群不对称退变临床意义[J]. 中华骨科杂志,2019,39(18):1133-1141. [13] XU Z, RAO H, ZHANG L, et al. Anterior Cervical Discectomy and Fusion Versus Hybrid Decompression and Fusion for the Treatment of 3-Level Cervical Spondylotic Myelopathy: A Comparative Analysis of Cervical Sagittal Balance and Outcomes. World Neurosurg. 2019;132:e752-e758. [14] JIN C, XIE N, REN Y, et al. How Does Cervical Sagittal Balance Change After Hangman Fracture Treated with Anterior or Posterior Approach Surgery? World Neurosurg. 2020;138:E767-E777. [15] ZAIDMAN N, DE WITTE O. Cervical sagittal balance: a predictor of neck pain after anterior cervical spine surgery? Br J Neurosurg. 2020:1-5. doi: 10.1080/02688697.2020.1850643. [16] HAN G, ZHOU S, WANG W, et al. Correlations between paraspinal extensor muscle endurance and clinical outcomes in preoperative LSS patients and clinical value of an endurance classification. J Orthop Translat. 2022;35:81-86. [17] HIYAMA A, KATOH H, SAKAI D, et al. The correlation analysis between sagittal alignment and cross-sectional area of paraspinal muscle in patients with lumbar spinal stenosis and degenerative spondylolisthesis. Bmc Musculoskelet Disord. 2019;20(1):352. [18] OZCAN-EKSI EE, EKSI MS, TURGUT VU, et al. Reciprocal relationship between multifidus and psoas at L4-L5 level in women with low back pain. Br J Neurosurg. 2021;35(2):220-228. [19] PINTER ZW, SALMONS HIT, TOWNSLEY S, et al. Semispinalis Cervicis Sarcopenia is Associated With Worsening Cervical Sagittal Balance and Junctional Alignment Following Posterior Cervical Fusion for Myelopathy. Clin Spine Surg. 2022. doi: 10.1097/BSD.0000000000001366. [20] MUELLNER M, HAFFER H, CHIAPPARELLI E, et al. Differences in lumbar paraspinal muscle morphology in patients with sagittal malalignment undergoing posterior lumbar fusion surgery. Eur Spine J. 2022;31(11):3109-3118. [21] FORTIN M, OMIDYEGANEH M, BATTIE MC, et al. Evaluation of an automated thresholding algorithm for the quantification of paraspinal muscle composition from MRI images. Biomed Eng Online. 2017;16(1):61. [22] SIONS JM, COYLE PC, VELASCO TO, et al. Multifidi Muscle Characteristics and Physical Function Among Older Adults With and Without Chronic Low Back Pain. Arch Phys Med Rehabil. 2017;98(1):51-57. [23] SALIMI H, OHYAMA S, TERAI H, et al. Trunk Muscle Mass Measured by Bioelectrical Impedance Analysis Reflecting the Cross-Sectional Area of the Paravertebral Muscles and Back Muscle Strength: A Cross-Sectional Analysis of a Prospective Cohort Study of Elderly Population. J Clin Med. 2021;10(6):1187. [24] HIYAMA A, KATOH H, SAKAI D, et al. Correlation analysis of sagittal alignment and skeletal muscle mass in patients with spinal degenerative disease. Sci Reports. 2018;8(1):15492. [25] 李佩芳, 聂涌, 陈佳丽, 等. 表面肌电及其生物反馈在下腰痛中的应用进展[J]. 中国修复重建外科杂志,2017,31(4):504-507. [26] TAKAHASHI I, KIKUCHI SI, SATO K, et al. Effects of the mechanical load on forward bending motion of the trunk - Comparison between patients with motion-induced intermittent low back pain and healthy subjects. Spine. 2007;32(2):E73-E78. [27] MAYER TG, NEBLETT R, BREDE E, et al. The Quantified Lumbar Flexion-Relaxation Phenomenon Is a Useful Measurement of Improvement in a Functional Restoration Program. Spine. 2009;34(22):2458-2465. [28] EBENBICHLER G, HABENICHT R, ZIEGELBECKER S, et al. Age- and sex-specific effects in paravertebral surface electromyographic back extensor muscle fatigue in chronic low back pain. Geroscience. 2020;42(1):251-269. [29] ZYZNAWSKA J, FRANKOWSKI G, WODKA-NATKANIEC E, et al. Disbalance and fatigue of the spinal extensors as one of the causes of the overload disease of the lumbar spine. Acta of Bioeng Biomech. 2019;21(3):119-125. [30] EGUCHI Y, TOYOGUCHI T, INAGE K, et al. Analysis of skeletal muscle mass in women over 40 with degenerative lumbar scoliosis. Eur Spine J. 2019;28(7):1618-1625. [31] MASAKI M, IKEZOE T, FUKUMOTO Y, et al. Association of sagittal spinal alignment with thickness and echo intensity of lumbar back muscles in middle-aged and elderly women. Arch Gerontol Geriatr. 2015;61(2):197-201. [32] 胡宗杉, 马鸿儒, 钱至恺, 等. 基于年龄和性别的中国正常成年人脊柱-骨盆矢状位形态的多中心研究[J]. 中华骨科杂志,2021,41(13):844-855. [33] 马鸿儒, 朱泽章, 史本龙, 等. 退变性脊柱侧凸矫形术后力学并发症的预测:对脊柱整体形态与平衡评分的修正与验证[J]. 中华骨科杂志,2020,40(4): 193-198. [34] YAGI M, HOSOGANE N, WATANABE K, et al. The paravertebral muscle and psoas for the maintenance of global spinal alignment in patient with degenerative lumbar scoliosis. Spine J. 2016;16(4): 451-458. [35] BANNO T, YAMATO Y, HASEGAWA T, et al. Assessment of the Cross-Sectional Areas of the Psoas Major and Multifidus Muscles in Patients With Adult Spinal Deformity A Case-Control Study. Clin Spine Surg. 2017;30(7):E968-E973. [36] WANG X, JIA R, LI J, et al. Research Progress on the Mechanism of Lumbarmultifidus Injury and Degeneration. Oxidative Medicine and Cellular Longevity. 2021;2021:6629037. [37] FAUR C, PATRASCU JM, HARAGUS H, et al. Correlation between multifidus fatty atrophy and lumbar disc degeneration in low back pain. Bmc Musculoskelet Disord. 2019;20(1):414. [38] FERRERO E, SKALLI W, LAFAGE V, et al. Relationships between radiographic parameters and spinopelvic muscles in adult spinal deformity patients. Eur Spine J. 2020;29(6):1328-1339. [39] XIA W, FU H, ZHU Z, et al. Association between back muscle degeneration and spinal-pelvic parameters in patients with degenerative spinal kyphosis. Bmc Musculoskelet Disord. 2019;20(1):454. [40] PARK JS, PARK YS, KIM J, et al. Sarcopenia and fatty degeneration of paraspinal muscle associated with increased sagittal vertical axis in the elderly: a cross-sectional study in 71 female patients. Eur Spine J. 2020;29(6):1353-1361. [41] WANG XJ, HUANG KK, HE JB, et al. Fatty infiltration in cervical extensor muscle: is there a relationship with cervical sagittal alignment after anterior cervical discectomy and fusion? BMC Musculoskelet Disord. 2022;23(1):641. [42] MOSER M, OKANO I, ALBERTINI SANCHEZ L, et al. Preoperative Association Between Quantitative Lumbar Muscle Parameters and Spinal Sagittal Alignment in Lumbar Fusion Patients. Spine (Phila Pa 1976). 2022;47(23):1675-1686. [43] HAN G, WANG W, ZHOU S, et al. Paraspinal Muscle Degeneration as an Independent Risk for Loss of Local Alignment in Degenerative Lumbar Scoliosis Patients After Corrective Surgery. Global Spine J. 2021:21925682211022284. [44] PENNINGTON Z, COTTRILL E, AHMED AK, et al. Paraspinal muscle size as an independent risk factor for proximal junctional kyphosis in patients undergoing thoracolumbar fusion. J Neurosurg Spine. 2019;31(3):380-388. [45] HIYAMA A, KATOH H, SAKAI D, et al. The correlation analysis between sagittal alignment and cross-sectional area of paraspinal muscle in patients with lumbar spinal stenosis and degenerative spondylolisthesis. BMC Musculoskelet Disord. 2019;20(1):352. [46] ENOMOTO M, UKEGAWA D, SAKAKI K, et al. Increase in Paravertebral Muscle Activity in Lumbar Kyphosis Patients by Surface Electromyography Compared With Lumbar Spinal Canal Stenosis Patients and Healthy Volunteers. J Spinal Disord Tech. 2012;25(6):E167-E173. [47] KATSU M, OHBA T, EBATA S, et al. Potential Role of Paraspinal Musculature in the Maintenance of Spinopelvic Alignment in Patients With Adult Spinal Deformities. Clin Spine Surg. 2020;33(2):E76-E80. [48] WANG W, SUN Z, LI W, et al. Relationships between Paraspinal Muscle and Spinopelvic Sagittal Balance in Patients with Lumbar Spinal Stenosis. Orthop Surg. 2022;14(6):1093-1099. [49] SHIMIZU K, MITSUHARA T, TAKEDA M, et al. Effects of Preservation of the Semispinalis Cervicis Inserted into C2 on Craniocervical Alignment After Laminoplasty. World Neurosurg. 2021;146:e1367-e1376. [50] HYUN SJ, BAE CW, LEE SH, et al. Fatty Degeneration of the Paraspinal Muscle in Patients With Degenerative Lumbar Kyphosis: A New Evaluation Method of Quantitative Digital Analysis Using MRI and CT Scan. Clin Spine Surg. 2016; 29(10):441-447. [51] LEE SH, PARK SW, KIM YB, et al. The fatty degeneration of lumbar paraspinal muscles on computed tomography scan according to age and disc level. Spine J. 2017;17(1):81-87. [52] PARK MS, MOON SH, KIM TH, et al. Paraspinal Muscles of Patients with Lumbar Diseases. J Neurol Surg A Cent Eur Neurosurg. 2018;79(4): 323-329. [53] FECHTENBAUM J, ETCHETO A, KOLTA S, et al. Sagittal balance of the spine in patients with osteoporotic vertebral fractures. Osteoporos Int. 2016;27(2):559-567. [54] BARREY C, ROUSSOULY P, LE HUEC JC, et al. Compensatory mechanisms contributing to keep the sagittal balance of the spine. Eur Spine J. 2013;22:S834-S841. [55] LAFAGE V, SCHWAB F, PATEL A, et al. Pelvic Tilt and Truncal Inclination Two Key Radiographic Parameters in the Setting of Adults With Spinal Deformity. Spine. 2009;34(17):E599-E606. [56] JACKSON RP, MCMANUS AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine (Phila Pa 1976). 1994;19(14):1611-1618. [57] HORI Y, HOSHINO M, INAGE K, et al. ISSLS PRIZE IN CLINICAL SCIENCE 2019: clinical importance of trunk muscle mass for low back pain, spinal balance, and quality of lifea multicenter cross-sectional study. Eur Spine J. 2019;28(5):914-921. [58] ZHU W, WANG W, KONG C, et al. Lumbar Muscle Fat Content Has More Correlations with Living Quality than Sagittal Vertical Axis in Elderly Patients with Degenerative Lumbar Disorders. Clin Int Aging. 2020;15:1717-1726. [59] TAKAHASHI S, HOSHINO M, OHYAMA S, et al. Relationship of back muscle and knee extensors with the compensatory mechanism of sagittal alignment in a community-dwelling elderly population. Sci Rep. 2021;11(1):2179. [60] YIN J, MA X, LIN T, et al. Characteristics and treatment of dynamic sagittal imbalance in adult spinal deformity. Eur Spine J. 2020;29(9):2340-2353. [61] SHIBA Y, TANEICHI H, INAMI S, et al. Dynamic global sagittal alignment evaluated by three-dimensional gait analysis in patients with degenerative lumbar kyphoscoliosis. Eur Spine J. 2016;25(8):2572-2579. [62] BASSANI T, OTTARDI C, COSTA F, et al. Semiautomated 3D Spine Reconstruction from Biplanar Radiographic Images: Prediction of Intervertebral Loading in Scoliotic Subjects. Front Bioeng Biotechnol. 2017;5:1. [63] YAGI M, KING AB, BOACHIE-ADJEI O. Incidence, Risk Factors, and Natural Course of Proximal Junctional Kyphosis Surgical Outcomes Review of Adult Idiopathic Scoliosis. Minimum 5 Years of Follow-up. Spine. 2012;37(17):1479-1489. [64] CRUZ-JENTOFT AJ, LANDI F, SCHNEIDER SM, et al. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing. 2014;43(6):748-759. [65] BLONDEL B, SCHWAB F, BESS S, et al. Posterior Global Malalignment After Osteotomy for Sagittal Plane Deformity It Happens and Here is Why. Spine. 2013; 38(7):E394-E401. [66] BAE JS, JANG JS, LEE SH, et al. Radiological analysis of lumbar degenerative kyphosis in relation to pelvic incidence. Spine J. 2012;12(11):1045-1051. [67] HONG JY, SUH SW, MODI HN, et al. Correlation of Pelvic Orientation With Adult Scoliosis. J Spinal Disord Tech. 2010;23(7):461-466. [68] LABELLE H, MAC-THIONG JM, ROUSSOULY P. Spino-pelvic sagittal balance of spondylolisthesis: a review and classification. Eur Spine J. 2011;(Suppl 5):641-646. [69] 李方财, 陈其昕, 陈维善, 等. 腰椎退行性侧凸患者脊柱矢状位参数与骨盆参数的相关性[J]. 中华骨科杂志,2013,33(9):928-934. [70] GOTTFRIED ON, DAUBS MD, PATEL AA, et al. Spinopelvic parameters in postfusion flatback deformity patients. Spine J. 2009;9(8):639-647. [71] ROUSSOULY P, GOLLOGLY S, BERTHONNAUD E, et al. Sagittal alignment of the spine and pelvis in the presence of L5-S1 isthmic lysis and low-grade spondylolisthesis. Spine. 2006;31(21):2484-2490. [72] BASSANI T, CASAROLI G, GALBUSERA F. Dependence of lumbar loads on spinopelvic sagittal alignment: An evaluation based on musculoskeletal modeling. PLoS One. 2019;14(3):e0207997. [73] WARD SR, KIM CW, ENG CM, et al. Architectural Analysis and Intraoperative Measurements Demonstrate the Unique Design of the Multifidus Muscle for Lumbar Spine Stability. J Bone Joint Surg Am. 2009;91A(1):176-185. [74] HEBERT JJ, KOPPENHAVER SL, TEYHEN DS, et al. The evaluation of lumbar multifidus muscle function via palpation: reliability and validity of a new clinical test. Spine J. 2015;15(6):1196-1202. [75] HOFSTE A, SOER R, HERMENS HJ, et al. Inconsistent descriptions of lumbar multifidus morphology: A scoping review. Bmc Musculoskelet Disord. 2020; 21(1):312. [76] SHAFAQ N, SUZUKI A, MATSUMURA A, et al. Asymmetric Degeneration of Paravertebral Muscles in Patients With Degenerative Lumbar Scoliosis. Spine. 2012;37(16):1398-1406. [77] KIM H, LEE CK, YEOM JS, et al. Asymmetry of the cross-sectional area of paravertebral and psoas muscle in patients with degenerative scoliosis. Eur Spine J. 2013;22(6):1332-1338. [78] YAGI M, KANEKO S, YATO Y, et al. Drop Body Syndrome A Distinct Form of Adult Spinal Deformity. Spine. 2017;42(16):E969-E977. |
| [1] | Du Xueting, Zhang Xiaodong, Chen Yanjun, Wang Mei, Chen Wubiao, Huang Wenhua. Application of compressed sensing technology in two-dimensional magnetic resonance imaging of the ankle joint [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(9): 1396-1402. |
| [2] | Xue Ting, Zhang Xinri, Kong Xiaomei. Mesenchymal stem cell therapy for pneumoconiosis using nanomaterials combined with multi-modal molecular imaging [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(7): 1133-1140. |
| [3] | Li Xiaoyin, Yang Xiaoqing, Chen Shulian, Li Zhengchao, Wang Ziqi, Song Zhen, Zhu Daren, Chen Xuyi. Collagen/silk fibroin scaffold combined with neural stem cells in the treatment of traumatic spinal cord injury [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(6): 890-896. |
| [4] | Zhang Qijian, Xu Ximing. Acquisition and application of ectodermal mesenchymal stem cells [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(6): 928-934. |
| [5] | Liu Guangluan, Guo Zonglei, Ge Jin, Huang Dong, Wang Yehua. Anatomic risk factors for medial meniscus posterior root tears combined with anterior cruciate ligament injuries [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(5): 663-668. |
| [6] | Guo Yingqi, Gong Xianxu, Zhang Yan, Xiao Han, Wang Ye, Gu Wenguang. Meniscus extrusion and patellofemoral joint cartilage injury and bone marrow lesions: MRI semi-quantitative score [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 600-605. |
| [7] | Liu Hao, Yang Hongsheng, Zeng Zhimou, Wang Liping, Yang Kunhai, Hu Yongrong, Qu Bo. Lumbar MRI vertebral bone quality score to evaluate the severity of osteoporosis in postmenopausal women [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 606-611. |
| [8] | Li Qizhe, Kong Yao, Fan Jiannan, Wu Yeting, Yang Hua, Xiao Yinlong, Sun Hong. Measurement and clinical significance of acetabular parameters in the Guizhou population [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(36): 5856-5863. |
| [9] | Huan Dawei, Yuan Zhaofeng, Dou Weiqiang, Xia Tianwei, Qiu Yue, Zhang Chao, Shen Jirong. Changes in microcirculatory perfusion of femoral head necrosis assessed by dynamic contrast-enhanced magnetic resonance imaging [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(36): 5864-5869. |
| [10] | Yuan Haibo, Li Dongya, Pan Bin, Guan Kai, Chen Feng, Yuan Feng, Wu Jibin. Sagittal related factors of upper lumbar disc herniation [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(31): 4984-4989. |
| [11] | Li Xiaojuan, Zhang Yuanzhi, Yang Xiaoguang, Gao Yang, Wu Qiong. Quantitative evaluation of bone structure changes in femoroacetabular impingement syndrome by magnetic resonance imaging [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(31): 4965-4970. |
| [12] | Wu Tong, Yin Caiyun, Zhao Mingzhe, Zhu Yishen. Application of functional peptides for biomedical diagnosis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(3): 478-485. |
| [13] | Li Panpan, Qing Haomiao, Ren Sixie, Zhang Yuanyuan. Correlation of medial and lateral posterior tibial slope and their differences with anterior cruciate ligament injury [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(27): 4379-4384. |
| [14] | Jin Xinjie, Lu Xiangdong, Zhao Yibo, Zhao Xiaofeng, Qi Detai, Zhao Bin. Endoscopic transforaminal lumbar interbody fusion for degenerative diseases of the lumbar spine: decompression fusion and preservation of posterior spine anatomy [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(27): 4401-4407. |
| [15] | Wang Wenli, Luo Lankun, Fu Yating, Chu Cheng, Ma Xiao, Liu Hua. Measurement and analysis of gingival biotype in maxillary anterior teeth using cone-beam computed tomography [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(23): 3616-3620. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||