Chinese Journal of Tissue Engineering Research ›› 2022, Vol. 26 ›› Issue (27): 4406-4410.doi: 10.12307/2022.875
Previous Articles Next Articles
Application of the socket-shield technique in the implant restoration
Wang Wenli, Zhang Zihan, Li Yourui
- Department of Prosthodontics, Affiliated Hospital, Binzhou Medical University, Binzhou 256603, Shandong Province, China
-
Received:2021-01-25Accepted:2021-03-04Online:2022-09-28Published:2022-03-12 -
Contact:Li Yourui, MD, Attending physician, Department of Prosthodontics, Affiliated Hospital, Binzhou Medical University, Binzhou 256603, Shandong Province, China -
About author:Wang Wenli, Master candidate, Department of Prosthodontics, Affiliated Hospital, Binzhou Medical University, Binzhou 256603, Shandong Province, China -
Supported by:the Project of Medical, Health Science and Technology Development Plan of Shandong Province, No. 2017WS753 (to LYR); Science and Technology Program of Binzhou Medical University, No. 2016KJ06 (to LYR)
CLC Number:
Cite this article
Wang Wenli, Zhang Zihan, Li Yourui. Application of the socket-shield technique in the implant restoration[J]. Chinese Journal of Tissue Engineering Research, 2022, 26(27): 4406-4410.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
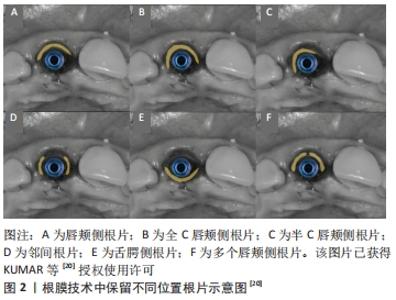
2.1 根膜技术的组织学基础 拔牙时的创伤和牙周韧带血供的丧失是导致拔牙后牙槽嵴发生改变的主要原因[8],特别是在上颌前牙区,该区域唇侧骨板较薄且大部分血供来自牙周膜,拔牙后不可避免地导致骨板吸收及覆盖软组织的塌陷,从而产生美学问题。牙根浸没技术最早由CASEY和LAUCIELLO在20世纪70年代提出,临床研究也已证实无论是活髓牙还是死髓牙的牙根保留,都可能会对拔牙后组织改变产生一定的影响。随后,SALAMA等[9]使用牙根浸没技术来维持固定局部义齿修复时桥体区的牙槽嵴形态,取得了良好的效果。2010年,HURZELER等[10]最先将牙根保留疗法引入种植领域,并将其命名为根膜技术,即保留拔牙窝内唇颊侧部分根片同期完成即刻种植,从而保留了根片唇颊侧的束状骨-牙周韧带复合体,保证了牙槽嵴良好的血供,基于生物学原理避免常规拔牙后所引发的唇颊侧牙槽骨吸收。 HURZELER等[10]对根膜技术进行了动物组织学上的观察,发现在根片的舌侧形成新的牙骨质和牙周附着结构,唇舌侧牙槽嵴无任何吸收且有新骨形成。MILTIADIS等[11]对采用根膜技术即刻植入的种植体进行了人类组织学分析,结果显示唇侧骨板由健康、完整的牙周韧带支持营养,无任何吸收迹象;种植体形成良好的骨结合,并在其表面有大量的致密成熟骨,骨与植入物的接触百分比为76.2%;种植体和根片之间的大部分间隙被致密的成熟骨填充,只有冠方部分存在非浸润的结缔组织。由此可认为,保留唇颊侧根片与即刻种植相结合不会妨碍种植体骨结合,还可避免拔牙后唇颊侧骨板的明显吸收。 2.2 根膜技术中保留根片的量 2.2.1 保留根片的厚度 根膜技术中保留根片的厚度是否会影响牙槽嵴的吸收,这是该技术在临床应用中备受关注的点。TAN等[12]通过Beagle犬动物实验观察到根片厚度在0.5-1.5 mm之间波动时,骨吸收与根片厚度呈负相关。具体的说,根片厚度在0.5-1.5 mm之间时,随根片厚度的增加唇侧骨板吸收可能会减少。出现这种现象的确切原因目前尚不清楚,可能是根片较厚时种植窝预备的不良反应如发热、振动等可得到有效控制,从而保留更健康的牙周韧带。当根片厚度超过1.5 mm时,尚不确定骨吸收与根片厚度是否仍存在线性关系,部分学者在临床操作中保留根片的厚度以根管至唇颊侧根面的一半作为参考标准[13-14]。此外,GALVO-GUIRADO等[15]通过动物实验比较了保留不同厚度根片和唇颊侧牙槽骨对根膜技术的影响,结果表明,当保留3 mm厚的唇颊侧骨板和2 mm厚的根片时可维持最佳的牙槽嵴形态。 2.2.2 保留根片的长度 合适的根片长度是根膜技术应用的前提。GALVO-GUIRADO等[16]在6只狗体内采用根膜技术植入48枚种植体(24枚狭窄型种植体和24枚标准型种植体),并保留了不同长度的剩余根片,冠方段(1/3);冠方中上段(2/3);全长(3/3),在第4,12周分别进行种植体稳定性分析和组织学评估,结果显示48枚种植体均可形成良好的骨结合;对于两种类型的种植体而言,与保留冠方中上段(2/3)和全长(3/3)根片相比,保留冠方段(1/3)根片的唇舌侧牙槽嵴吸收量最小,且保留根片长度大于2 mm时,组织学结果显示骨、根片和种植体之间缺乏黏附,结缔组织向根方迁移,破坏束状骨的稳定性。此外,ROE等[17]提出根片较短时术中可以更好地控制种植体的方向和位置,而当根片较长时种植体植入空间则会明显受限。 2.2.3 保留根片的高度 有学者认为保留的根片应位于牙槽嵴冠方1 mm处,这样不仅能有效防止上皮向下生长,还能保留更多的牙周韧带,以利于维持软组织的稳定[18];但亦有学者认为根片应与唇颊侧牙槽嵴处于同一水平,这样可减少根片折裂及根片内暴露的风险[15]。对于保留根片的高度不同是否会对牙槽嵴的吸收产生影响,TAN等[12]进行了研究,结果表明根膜技术可以有效减少骨吸收,但根片高度与牙槽嵴吸收的关系并不密切。 2.3 根膜技术中保留根片的位置 根膜技术通常应用于前牙美学区,以保留唇侧根片为主[19],但在临床中患者可能会出现复杂和混杂的情况。KUMAR等[20]根据具体临床情况提出了在牙槽窝中保留不同位置的根片,见图2。"
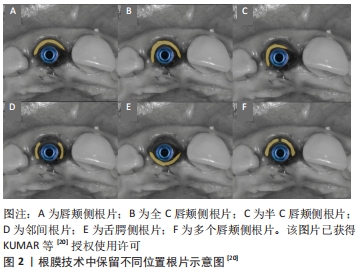

唇颊侧根片即根片仅位于牙槽窝的唇颊部,适用于近远中均存在天然牙的单个缺牙部位;全C唇颊侧根片即根片由牙槽窝唇颊部至两侧邻间部,适用于以下3种情况:该部位两侧均有种植体、两侧牙齿缺失无种植体、一侧有种植体,另一侧牙齿缺失无种植体;半C唇颊侧根片即根片由牙槽窝唇颊部至一侧邻间部,适用于一侧存在天然牙,另一侧有种植体或牙齿缺失无种植体的单个缺牙部位;邻间根片即根片仅位于牙槽窝的近中或远中部分,这种设计适用于唇颊侧骨板吸收需要植骨的情况,也适用于一侧牙齿缺失或存在种植体的情况;舌腭侧根片即根片位于牙槽窝的舌侧或腭侧,这种类型的根片适用范围较小,可考虑用于上颌磨牙;多个唇颊侧根片即在牙槽窝内有两个或多个唇颊侧根片,它适用于牙根纵裂的病例,有证据表明纵裂的牙根之间有骨沉积,这有助于将两个断片固定到位。 2.4 根片与种植体间隙的处理 2.4.1 根片与种植体之间是否保留间隙 HURZELER等[10]采用根膜技术将4枚种植体植入Beagle犬下颌前的磨牙位置,将4枚种植体随机分为与根片保持接触或不接触两组,组织学观察发现,当种植体与根片未接触时,根片舌侧覆盖一层薄薄的新形成的牙骨质,在新形成的牙骨质与种植体之间充满健康的结缔组织,并附着在种植体表面,牙槽嵴无任何吸收现象;另一组将种植体与根片接触放置,在种植体螺纹之间的区域内充满结缔组织,种植体螺纹顶端与根片舌侧新形成的牙骨质发生结合,牙槽嵴未见骨吸收迹象。 此研究说明种植体与根片间有无间隙存在,不会对种植体骨结合及牙槽嵴吸收产生影响。但GLUCKMAN等[21]认为种植体与根片的接触不是必需或推荐的,如发生接触可能存在根片移位及牙周韧带结构破坏的风险。 因此,临床操作中应根据植入位点牙槽窝的大小和形态,做出合适的选择。 2.4.2 根片与种植体的间隙内是否需要植骨 即刻种植时种植体的大小形态往往与拔牙窝不相符,因此拔牙后即刻植入的种植体与牙槽窝壁之间存在着不同程度的间隙,通常将此间隙称为跳跃间隙。目前关于即刻种植跳跃间隙内是否需要植骨仍存在争议,COVANI等[22]研究中未在骨与种植体间的间隙内植入屏障膜或骨移植材料,结果发现间隙内仍有新骨形成并与种植体形成骨结合;PAOLANTONIO等[23]认为即刻种植骨间隙在 2 mm以内,不必植入屏障膜及骨移植材料;CARDAROPOLI等[24]研究表明,在即刻种植体的骨间隙中放置骨移植材料能减少牙槽嵴吸收及软组织的变化,对拔牙后软硬组织的保留有一定的作用。近年来的研究绝大部分认为应在跳跃间隙内植骨,否则不易维持牙槽骨的形态,获得满意的美学效果[25-28]。 对于采用根膜技术时根片与种植体间隙的处理,有学者认为在种植体表面和根片之间的小间隙有自发愈合的潜力,而较大的间隙应该用骨替代物填充,否则就容易受到干扰和感染[29]。GLUCKMAN等[30]认为,当种植体与根片之间存在间隙时即应在间隙内放置骨移植材料。DAYAKAR等[6]研究表明,当种植体表面与根片之间的间隙小于1 mm时不需要骨移植物来填补间隙,但当间隙大于1 mm时则需要进行植骨手术。BAUMER等[31]认为在根片和种植体之间的骨移植物作用有限,应该限制在距离超过1 mm的情况下使用。KUMAR等[20]提出根片和种植体之间的最佳间隙为1.5 mm左右,如果间隙超过3 mm建议进行植骨。 因此,在临床应用中根片与种植体的间隙小于1 mm时可不考虑植骨,当根片与种植体的间隙超过1 mm时可选择植骨。 2.5 根膜技术应用的区域 2.5.1 根膜技术在即刻种植位点的应用 延期种植技术已有明确的研究结果,其在前牙区和后牙区都具有高存留率和成功率[32-33]。为减少软硬组织吸收,获得种植修复良好的美学效果,从而引入根膜技术,该技术多应用于前牙美学区,并取得了令人满意的结果[34]。BRAMANTI等[35]在一项随访3年的研究中比较了根膜技术即刻种植和常规即刻种植两者术后的临床效果,发现两组种植体成功率相当,但采用根膜技术即刻种植术后的骨吸收量低于常规即刻种植,且具有更佳的美学效果。 ZHU等[36]在一项随访4年的研究中,采用根膜技术植入的种植体均成功结合,红色美学评分为13.5。BAUMER等[37]对10例采用根膜技术的病例进行了5年的回顾性研究,结果表明所有种植体无不良事件发生,面部组织轮廓相比拔牙前变化程度较低,红色美学评分为12。同样,SCHWIMER等[38]对根膜技术在后牙区的应用也进行了研究,结果表明保留的根片对维持磨牙区种植位点的牙槽嵴形态也有一定的作用,同时提出由于磨牙部位存在牙根过度弯曲的特异性及根膜技术本身的敏感性,因此该技术在后牙区的应用相比前牙区较为困难。 2.5.2 根膜技术在桥体区的应用 当牙列缺损采用固定局部义齿修复时同样会面临桥体区根方软硬组织吸收的问题[39],导致桥体龈端与牙槽嵴粘膜之间出现缝隙,从而出现食物嵌塞、牙龈炎等一系列问题,因此减少软硬组织吸收维持牙槽嵴形态对于桥体区亦十分重要。牙根浸没技术早在40多年前提出,并且已证明该技术可以保留牙周组织及桥体部位的牙槽嵴,但该技术的应用受根尖周病变和牙髓治疗的限制[40]。2015年,根膜技术与位点保存相结合应用于桥体区——即桥体盾[41],它克服了牙根浸没技术的限制,可减少桥体区牙槽嵴的吸收,有效维持桥体区牙槽嵴原有形态。GLUCKMAN等[13]对10例患者采用桥体盾的14个位点进行研究,在12,18个月的随访中,所有病例都成功地维持了桥体区牙槽嵴形态,无软硬组织塌陷。 2.6 临床操作要点 2.6.1 适应证 目前,国际上对根膜技术的适应证尚无共识性结论,但适应证的选择应基于以下几点考虑[42-43]:主要适用于上下颌前牙区;因外伤或破坏性龋病导致无法修复的单颗或多颗连续牙齿;有健康的牙周组织及充足的骨量;无急慢性根尖周炎症,口腔卫生良好。 2.6.2 禁忌证 绝对禁忌证:有常规口腔种植手术的禁忌病史(糖尿病未得到控制或治疗,口腔和颌面部放化疗等);目前存在牙周病或有牙周病史;牙齿松动。 相对禁忌证:保留根片区域有垂直折裂的牙齿;在骨平面以下有水平折裂的牙齿;有内吸收或外吸收的牙齿。 2.6.3 术中操作要点 因根膜技术主要应用于前牙美学区[44],现以前牙区保留单颗牙齿的唇侧根片为例,简述术中操作要点:用金刚砂车针将待拔除牙齿的牙冠截至平齐牙龈,再沿根管方向将牙根分为唇、舌侧两部分[45],采用微创拔牙器械取出舌侧根片,修整唇侧根片呈弯月微凹形态,且冠方位于牙槽嵴顶水平或牙槽嵴顶上方1 mm处,厚度为1.5 mm左右[46-47],修整结束后检查根片的稳定性,保证根片稳定不松动后根据种植体制造商的指南进行种植窝的预备,植入相应的种植体。若种植体植入后与根片间存在1 mm以上的间隙时,可选择在间隙内植骨。 2.6.4 术后即刻修复 采用根膜技术即刻植入种植体后,应选择个性化愈合基台或临时修复体进行即刻封闭,以支撑牙龈组织,更好地维持龈缘及龈乳头的形态[48]。KAN等[49]在即刻种植后采用新型复合树脂制作模拟对侧天然牙牙龈结构的修复体,直至观察到和谐的软组织结构及龈缘轮廓后戴入最终修复体,1年后临床和影像学随访显示,种植体龈缘及龈乳头形态保持良好,获得了满意的美学效果。 ABD-ELRAHMAN等[44]研究中比较了采用根膜技术即刻种植与常规即刻种植后即刻修复的美学效果,两组即刻种植后均在直线型愈合基台上安放“S”型的临时修复体,以最大限度地支持软组织并即刻负载;术后6个月进行口腔锥形束CT扫描显示,采用根膜技术即刻种植位点的唇侧骨板水平和垂直方向骨损失量明显小于传统即刻种植技术;且采用根膜技术即刻种植位点维持良好的牙龈组织形态,术后6个月的红色美学评分为12,传统即刻种植位点的牙龈组织明显塌陷,红色美学评分为9。因此,即刻修复对维持软组织稳定、获得良好的美学效果具有重要意义。 2.7 并发症 2.7.1 生物学并发症 根膜技术面临着术后种植体骨结合失败、根片暴露、根片感染、根片移位、种植体周围炎、种植体周围黏膜炎等这些生物学并发症发生的风险[50-51]。GLUCKMAN等[52]对128例采用根膜技术即刻种植的病例进行了1-4年的回顾性研究,共25例发生并发症(并发症发生率19.5%),其中5例种植体骨结合失败,16例根片暴露(内部暴露12例,外部暴露4例),3例根片感染,1例根片移位,所有随访病例中无种植体周围炎发生。这项研究表明,根片内部暴露是根膜技术最常见的并发症,其原因可能是根片的冠方和修复体龈端之间缺乏足够的空间;其次,最常见的并发症是根片外部暴露,这可能是由于根片冠方保留过多,或存在穿透覆盖软组织的锐利边缘。该研究中所有并发症通过清创、修整根片、软组织移植等方法得到了有效解决。 2.7.2 机械并发症 根膜技术同样会出现螺丝松动或折断、基台松动或折断、种植体折裂、修复体崩瓷、松动或脱落等这些种植修复的机械并发症[53-54],对此应该严格把握种植适应证、合理设计种植修复方案以及重视种植修复后咬合关系的调整,从而避免机械并发症的发生。"

| [1] ARABBI KC, SHARANAPPA M, PRIYA Y, et al. Socket Shield: A Case Report. J Pharm Bioallied Sci. 2019;11(Suppl 1):S72-S75. [2] VINA-ALMUNIA J, CANDEL-MARTI ME, CERVERA-BALLESTER J, et al. Buccal bone crest dynamics after immediate implant placement and ridge preservation techniques: review of morphometric studies in animals. Implant Dent. 2013;22(2):155-160. [3] MOURYA A, MISHRA SK, GADDALE R, et al. Socket-shield technique for implant placement to stabilize the facial gingival and osseous architecture: A systematic review. J Investig Clin Dent. 2019;10(4):e12449. [4] CHEN ST, BUSER D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla--a systematic review. Int J Oral Maxillofac Implants. 2014;29 Suppl:186-215. [5] TIWARI S, BEDI RS, WADHWANI P, et al. Comparison of Immediate Implant Placement Following Extraction with and Without Socket-Shield Technique in Esthetic Region. J Maxillofac Oral Surg. 2020;19(4): 552-560. [6] DAYAKAR MM, WAHEED A, BHAT HS, et al. The socket-shield technique and immediate implant placement. J Indian Soc Periodontol. 2018;22(5):451-455. [7] 马国武,薛藏辉.“盾构术”在前牙美学区种植中的应用[J].口腔医学研究,2018,34(6):581-584. [8] SCHWIMER C, PETTE GA, GLUCKMAN H, et al. Human Histologic Evidence of New Bone Formation and Osseointegration Between Root Dentin (Unplanned Socket-Shield) and Dental Implant: Case Report. Int J Oral Maxillofac Implants. 2018;33(1):e19-e23. [9] SALAMA M, ISHIKAWA T, SALAMA H, et al. Advantages of the root submergence technique for pontic site development in esthetic implant therapy. Int J Periodontics Restorative Dent. 2007;27(6):521-527. [10] HURZELER MB, ZUHR O, SCHUPBACH P, et al. The socket-shield technique: a proof-of-principle report. J Clin Periodontol. 2010;37(9): 855-862. [11] MITSIAS ME, SIORMPAS KD, KOTSAKIS GA, et al. The Root Membrane Technique: Human Histologic Evidence after Five Years of Function. Biomed Res Int. 2017;2017:7269467. [12] TAN Z, KANG J, LIU W, et al. The effect of the heights and thicknesses of the remaining root segments on buccal bone resorption in the socket-shield technique: An experimental study in dogs. Clin Implant Dent Relat Res. 2018;20(3): 352-359. [13] GLUCKMAN H, SALAMA M, DU TOIT J. Partial Extraction Therapies (PET) Part 2: Procedures and Technical Aspects. Int J Periodontics Restorative Dent. 2017;37(3):377-385. [14] Du TOIT J, GLUCKMAN H. The Modified Socket-Shield Technique. J Craniofac Surg. 2018;29(7):2005-2006. [15] CALVO-GUIRADO JL, TROIANO M, LOPEZ-LOPEZ PJ, et al. Different configuration of socket shield technique in peri-implant bone preservation: An experimental study in dog mandible. Ann Anat. 2016;208:109-115. [16] CALVO-GUIRADO JL, BENITEZ-GARCIA JA, MATE SDVJ, et al. Socket-shield technique: the influence of the length of the remaining buccal segment of healthy tooth structure on peri-implant bone and socket preservation. A study in dogs. Ann Anat. 2019;221:84-92. [17] ROE P, KAN J, RUNGCHARASSAENG K. Residual root preparation for socket-shield procedures: a facial window approach. Int J Esthet Dent. 2017;12(3): 324-335. [18] MITSIAS ME, SIORMPAS KD, KONTSIOTOU-SIORMPA E, et al. A Step-by-Step Description of PDL-Mediated Ridge Preservation for Immediate Implant Rehabilitation in the Esthetic Region. Int J Periodontics Restorative Dent. 2015;35(6):835-841. [19] GUO T, NIE R, XIN X, et al. Tissue preservation through socket-shield technique and platelet-rich fibrin in immediate implant placement: A case report. Medicine (Baltimore). 2018;97(50):e13175. [20] KUMAR PR, KHER U. Shield the socket: Procedure, case report and classification. J Indian Soc Periodontol. 2018;22(3):266-272. [21] GLUCKMAN H, Du TOIT J, SALAMA M, et al. A decade of the socket-shield technique: a step-by-step partial extraction therapy protocol. Int J Esthet Dent. 2020;15(2):212-225. [22] COVANI U, MARCONCINI S, GALASSINI G, et al. Connective tissue graft used as a biologic barrier to cover an immediate implant. J Periodontol. 2007; 78(8):1644-1649. [23] PAOLANTONIO M, DOLCI M, SCARANO A, et al. Immediate implantation in fresh extraction sockets. A controlled clinical and histological study in man. J Periodontol. 2001;72(11):1560-1571. [24] CARDAROPOLI D, TAMAGNONE L, ROFFREDO A, et al. Preservation of Peri-implant Hard Tissues Following Immediate Postextraction Implant Placement. Part I: Radiologic Evaluation. Int J Periodontics Restorative Dent. 2019;39(5):633-641. [25] CHU SJ, SALAMA MA, GARBER DA, et al. Flapless Postextraction Socket Implant Placement, Part 2: The Effects of Bone Grafting and Provisional Restoration on Peri-implant Soft Tissue Height and Thickness- A Retrospective Study. Int J Periodontics Restorative Dent. 2015;35(6):803-809. [26] ARAUJO MG, LINDER E, LINDHE J. Bio-Oss collagen in the buccal gap at immediate implants: a 6-month study in the dog. Clin Oral Implants Res. 2011;22(1):1-8. [27] CHU SJ, SAITO H, SALAMA MA, et al. Flapless Postextraction Socket Implant Placement, Part 3: The Effects of Bone Grafting and Provisional Restoration on Soft Tissue Color Change-A Retrospective Pilot Study. Int J Periodontics Restorative Dent. 2018;38(4):509-516. [28] TARNOW DP, CHU SJ, SALAMA MA, et al. Flapless postextraction socket implant placement in the esthetic zone: part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change-a retrospective cohort study. Int J Periodontics Restorative Dent. 2014;34(3):323-331. [29] SCHNEIDER D, GRUNDER U, ENDER A, et al. Volume gain and stability of peri-implant tissue following bone and soft tissue augmentation: 1-year results from a prospective cohort study. Clin Oral Implants Res. 2011;22(1):28-37. [30] GLUCKMAN H, DU TOIT J, SALAMA M. The Pontic-Shield: Partial Extraction Therapy for Ridge Preservation and Pontic Site Development. Int J Periodontics Restorative Dent. 2016;36(3):417-423. [31] BAUMER D, ZUHR O, REBELE S, et al. The socket-shield technique: first histological, clinical, and volumetrical observations after separation of the buccal tooth segment - a pilot study. Clin Implant Dent Relat Res. 2015; 17(1):71-82. [32] BUSER D, JANNER SF, WITTNEBEN JG, et al. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: a retrospective study in 303 partially edentulous patients. Clin Implant Dent Relat Res. 2012;14(6):839-851. [33] FISCHER K, STENBERG T. Prospective 10-year cohort study based on a randomized controlled trial (RCT) on implant-supported full-arch maxillary prostheses. Part 1: sandblasted and acid-etched implants and mucosal tissue. Clin Implant Dent Relat Res. 2012;14(6):808-815. [34] DASH S, MOHAPATRA A, SRIVASTAVA G, et al. Retaining and Regaining Esthetics in the Anterior Maxillary Region Using the Socket-Shield Technique. Contemp Clin Dent. 2020;11(2):158-161. [35] BRAMANTI E, NORCIA A, CICCIU M, et al. Postextraction Dental Implant in the Aesthetic Zone, Socket Shield Technique Versus Conventional Protocol. J Craniofac Surg. 2018;29(4):1037-1041. [36] ZHU YB, QIU LX, CHEN L, et al. [Clinical evaluation of socket shield technique in maxillary anterior region]. Zhonghua Kou Qiang Yi Xue Za Zhi. 2018; 53(10):665-668. [37] BAUMER D, ZUHR O, REBELE S, et al. Socket Shield Technique for immediate implant placement - clinical, radiographic and volumetric data after 5 years. Clin Oral Implants Res. 2017;28(11):1450-1458. [38] SCHWIMER CW, GLUCKMAN H, SALAMA M, et al. The socket-shield technique at molar sites: A proof-of-principle technique report. J Prosthet Dent. 2019;121(2):229-233. [39] HABASHNEH RA, WALID MA, ABUALTEEN T, et al. Socket-shield Technique and Immediate Implant Placement for Ridge Preservation: Case Report Series with 1-year Follow-up. J Contemp Dent Pract. 2019;20(9):1108-1117. [40] GLUCKMAN H, SALAMA M, DU TOIT J. Partial Extraction Therapies (PET) Part 1: Maintaining Alveolar Ridge Contour at Pontic and Immediate Implant Sites. Int J Periodontics Restorative Dent. 2016;36(5):681-687. [41] POLIS-YANES C, CADENAS-SEBASTIAN C, OLIVER-PUIGDOMENECH C, et al. A Double Case: Socket Shield and Pontic Shield Techniques on Aesthetic Zone. Case Rep Dent. 2020;2020:8891772. [42] SIORMPAS KD, MITSIAS ME, KOTSAKIS GA, et al. The Root Membrane Technique: A Retrospective Clinical Study With Up to 10 Years of Follow-Up. Implant Dent. 2018;27(5):564-574. [43] SUPRIYA SHAKYA,张鑫,王剑.种植盾构术的研究进展[J].国际口腔医学杂志,2020,47(1):109-114. [44] ABD-ELRAHMAN A, SHAHEEN M, ASKAR N, et al. Socket shield technique vs conventional immediate implant placement with immediate temporization. Randomized clinical trial. Clin Implant Dent Relat Res. 2020;22(5):602-611. [45] YAN SJ, ZHOU C, LIU J, et al. [Clinical evaluation of the socket-shield technique for immediate implantation in the maxillary anterior region]. Hua Xi Kou Qiang Yi Xue Za Zhi. 2019;37(6):615-620. [46] BRAMANTI E, NORCIA A, CICCIU M, et al. Postextraction Dental Implant in the Aesthetic Zone, Socket Shield Technique Versus Conventional Protocol. J Craniofac Surg. 2018;29(4):1037-1041. [47] HUANG H, SHU L, LIU Y, et al. Immediate Implant Combined With Modified Socket-Shield Technique: A Case Letter. J Oral Implantol. 2017;43(2):139-143. [48] CHEREL F, ETIENNE D. Papilla preservation between two implants: a modified socket-shield technique to maintain the scalloped anatomy? A case report. Quintessence Int. 2014;45(1):23-30. [49] KAN JY, RUNGCHARASSAENG K. Proximal socket shield for interimplant papilla preservation in the esthetic zone. Int J Periodontics Restorative Dent. 2013;33(1):e24-e31. [50] ZUHR O, STAEHLER P, HUERZELER M. Complication Management of a Socket Shield Case After 6 Years of Function. Int J Periodontics Restorative Dent. 2020;40(3):409-415. [51] GLUCKMAN H, NAGY K, DU TOIT J. Prosthetic management of implants placed with the socket-shield technique. J Prosthet Dent. 2019;121(4):581-585. [52] GLUCKMAN H, SALAMA M, DU TOIT J. A retrospective evaluation of 128 socket-shield cases in the esthetic zone and posterior sites: Partial extraction therapy with up to 4 years follow-up. Clin Implant Dent Relat Res. 2018;20(2):122-129. [53] De KOK IJ, DUQUM IS, KATZ LH, et al. Management of Implant/Prosthodontic Complications. Dent Clin North Am. 2019;63(2):217-231. [54] STAVROPOULOS A, BERTL K, EREN S, et al. Mechanical and biological complications after implantoplasty-A systematic review. Clin Oral Implants Res. 2019;30(9):833-848. [55] SAEIDI PR, ZUHR O, HURZELER M, et al. Clinical Benefits of the Immediate Implant Socket Shield Technique. J Esthet Restor Dent. 2017;29(2):93-101. [56] 许亚梅,黄弘,王黎,等.改良盾构术与传统即刻种植术的临床效果对比研究[J].华西口腔医学杂志,2019,37(5):490-495. [57] BLASCHKE C, SCHWASS DR. The socket-shield technique: a critical literature review. Int J Implant Dent. 2020;6(1):52. [58] GHARPURE AS, BHATAVADEKAR NB. Current Evidence on the Socket-Shield Technique: A Systematic Review. J Oral Implantol. 2017;43(5):395-403. |
| [1] | Yao Xiaoling, Peng Jiancheng, Xu Yuerong, Yang Zhidong, Zhang Shuncong. Variable-angle zero-notch anterior interbody fusion system in the treatment of cervical spondylotic myelopathy: 30-month follow-up [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1377-1382. |
| [2] | Zhu Chan, Han Xuke, Yao Chengjiao, Zhou Qian, Zhang Qiang, Chen Qiu. Human salivary components and osteoporosis/osteopenia [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1439-1444. |
| [3] | Jin Tao, Liu Lin, Zhu Xiaoyan, Shi Yucong, Niu Jianxiong, Zhang Tongtong, Wu Shujin, Yang Qingshan. Osteoarthritis and mitochondrial abnormalities [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1452-1458. |
| [4] | Zhang Lichuang, Xu Hao, Ma Yinghui, Xiong Mengting, Han Haihui, Bao Jiamin, Zhai Weitao, Liang Qianqian. Mechanism and prospects of regulating lymphatic reflux function in the treatment of rheumatoid arthritis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1459-1466. |
| [5] | Wang Jing, Xiong Shan, Cao Jin, Feng Linwei, Wang Xin. Role and mechanism of interleukin-3 in bone metabolism [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1260-1265. |
| [6] | Zhu Chan, Han Xuke, Yao Chengjiao, Zhang Qiang, Liu Jing, Shao Ming. Acupuncture for Parkinson’s disease: an insight into the action mechanism in animal experiments [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1272-1277. |
| [7] | Guo Jia, Ding Qionghua, Liu Ze, Lü Siyi, Zhou Quancheng, Gao Yuhua, Bai Chunyu. Biological characteristics and immunoregulation of exosomes derived from mesenchymal stem cells [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1093-1101. |
| [8] | Wu Weiyue, Guo Xiaodong, Bao Chongyun. Application of engineered exosomes in bone repair and regeneration [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1102-1106. |
| [9] | Zhou Hongqin, Wu Dandan, Yang Kun, Liu Qi. Exosomes that deliver specific miRNAs can regulate osteogenesis and promote angiogenesis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1107-1112. |
| [10] | Zhang Jinglin, Leng Min, Zhu Boheng, Wang Hong. Mechanism and application of stem cell-derived exosomes in promoting diabetic wound healing [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1113-1118. |
| [11] | Huang Chenwei, Fei Yankang, Zhu Mengmei, Li Penghao, Yu Bing. Important role of glutathione in stemness and regulation of stem cells [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1119-1124. |
| [12] | Hui Xiaoshan, Bai Jing, Zhou Siyuan, Wang Jie, Zhang Jinsheng, He Qingyong, Meng Peipei. Theoretical mechanism of traditional Chinese medicine theory on stem cell induced differentiation [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1125-1129. |
| [13] | An Weizheng, He Xiao, Ren Shuai, Liu Jianyu. Potential of muscle-derived stem cells in peripheral nerve regeneration [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1130-1136. |
| [14] | Fan Yiming, Liu Fangyu, Zhang Hongyu, Li Shuai, Wang Yansong. Serial questions about endogenous neural stem cell response in the ependymal zone after spinal cord injury [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1137-1142. |
| [15] | Xu Lei, Han Xiaoqiang, Zhang Jintao, Sun Haibiao. Hyaluronic acid around articular chondrocytes: production, transformation and function characteristics [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(5): 768-773. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||