Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (11): 1767-1773.doi: 10.3969/j.issn.2095-4344.1104
Previous Articles Next Articles
Causes, assessment and treatment strategies of sarcopenia in older adults
Wang Kun1,2,Luo Jiong1,2,Liu Li1,2,Ouyang Yiyi1,2
- (1College of Physical Education, Southwest University, State Key Laboratory of Physical Fitness Evaluation and Sports Function Monitoring, Chongqing 400715, China; 2Institute for Sports Rehabilitation of Southwest University, Chongqing 400715, China)
-
Received:2018-10-07Online:2019-04-18Published:2021-04-28 -
Contact:Luo Jiong, PhD, Professor, College of Physical Education, Southwest University, State Key Laboratory of Physical Fitness Evaluation and Sports Function Monitoring, Chongqing 400715, China; Institute for Sports Rehabilitation of Southwest University, Chongqing 400715, China -
About author:Wang Kun, Master candidate, College of Physical Education, Southwest University, State Key Laboratory of Physical Fitness Evaluation and Sports Function Monitoring, Chongqing 400715, China; Institute for Sports Rehabilitation of Southwest University, Chongqing 400715, China -
Supported by:the Basic Research Fund of the Central University of Southwest University, No. SWU1809221 (to LL)
CLC Number:
Cite this article
Wang Kun, Luo Jiong, Liu Li, Ouyang Yiyi. Causes, assessment and treatment strategies of sarcopenia in older adults[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(11): 1767-1773.
share this article
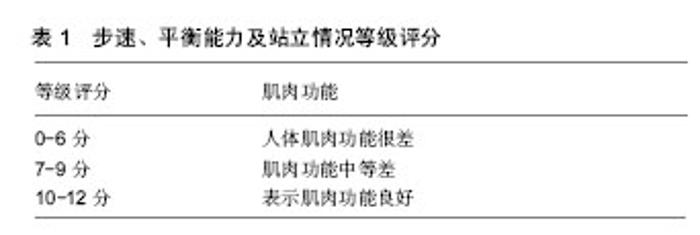
2.1 肌少症评估方法 欧盟肌少症工作小组(EWGSOP)在2010年建立肌少症评估指标,分别为肌肉量、肌力、身体表现3项。国际上关于肌少症的评估与测量方法均在此基础上并根据切点、人种、地区等的不同,进行深化展开。 2.1.1 肌肉量方面 肌肉量的测量评估会因测量方法、肌内血管及脂肪夹杂等产生误差,且受测对象的性别、年龄、体质量及疾病等生物差异因素均会影响测试结果[13]。 欧盟肌少症工作小组的评估标准方面,肌肉量采用双能量X光吸收仪(DXA)或生物电阻法(BIA)评估,并以低于年轻族群2个标准差为切点,参数使用分别有四肢骨骼肌质量(ASM)/ht2、全身骨骼肌质量(TSM)/ht2、ASM/wt、骨骼肌质量指数(SMI)等[8]。而亚太肌少症事物委员会(AWGS,2014)指出[2],男性在肌肉量的切点不论是双能量X光吸收仪还是生物电阻法,皆以 7.0 kg/m2为标准,但女性的双能量X光吸收仪和生物电阻法标准分别为≤5.4 kg/m2和≤5.7 kg/m2,小于标准则视为肌肉量减少。研究对比显示,双能量X光吸收仪具备花费时间短、辐射量低的特征,且在测量骨骼肌量的部分和MRI有很强的相关性(>0.94);而生物电阻法虽然相对简易、安全、便宜,但准确性相对较弱[14-15]。此外,生物电阻法仪器本身的校正方程式是否准确被不断的验证,并且测量时一定程度上会受温度、湿度等测量环境的影响,但因生物电阻法和MRI间具备相关性,加之其可移动及花费低等特征,亚太肌少症事物委员会仍然支持生物电阻法作为肌少症的评估工具之一,尤其用于社区中[16]。而MRI、CT等被认为是肌肉质量检测黄金标准仪器,但其费用高、辐射量大及仪器取得上并不理 想[4]。因此双能量X光吸收仪评估法被认为是目前测量肌少症最广为使用和推荐的评估工具[7],并被中华医学会骨质疏松和骨矿盐疾病分会的《肌少症共识》推荐为首选评估方法[13]。可见,肌肉量的测量评估必须考虑多个影响因子,在工具选择上须遵循便于操作、行之有效原则。 2.1.2 肌力方面 肌力的评估工具目前较常用的有握力及下肢肌力测试。吴雅汝等[15]指出,肌力的测试评估主要使用握力测试,并通过结合年龄来做校正评估。付素华[17]指出,目前最常用的是握力测定法,其与下肢肌力、腓肠肌横截面积、膝关节屈伸力具有良好相关性。周怡君等[14]通过握力测试实验指出,JAMAR握力器为最广泛使用且较标准的评估工具;而下肢肌力测试同样也具备良好的评估效能,但其需受过专门技术训练的技术人员使用测力器才能完成,因此在临床使用受限。在评估标准方面,欧盟肌少症工作小组指出[7],肌力评估以手握力为主,其中男、女分别为<30 kg、<20 kg。有研究提出,更准确的切分点应当根据体质量指数作为参照为切分点[8]。但有学者对此切点标准提出质疑,并认为体质量指数不适合用来评估高龄者的肌力状况[18]。而亚太肌少症事物委员会在欧盟肌少症工作小组等的基础上,针对亚洲人与西方人的肌肉构造特点具有明显的差异问题,因此于2013年提出亚洲男性和女性的手握力切点应分别为<26 kg和<18 kg[7]。事实证明,西方人的肌肉偏重于条状肌,而亚洲人的肌肉块状肌居多;肌腱、肌纤维及长骨等的长度西方人略大于亚洲人。因此,在同样条件下,亚洲人的绝对力量较西方人稍弱,手握力同样也略低于西方人。所以亚太肌少症事物委员会提出的评估肌少症的切点标准更符合于亚洲人。 2.1.3 生理表现方面 Cruz-Jentoft等[4]指出,生理表现方面可使用多种测量方式,主要包括简短身体功能量表(short physical performance battery,SPBB)、行走速度、6 min行走距离、计时起立行走测试等。其中最主要的评估方法是简短身体功能量表和行走速度测量。研究指出,简短身体功能量表是平衡、步频、肌力的综合评估,在临床或研究上都是标准的评估[14],见表1。"
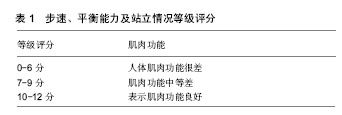
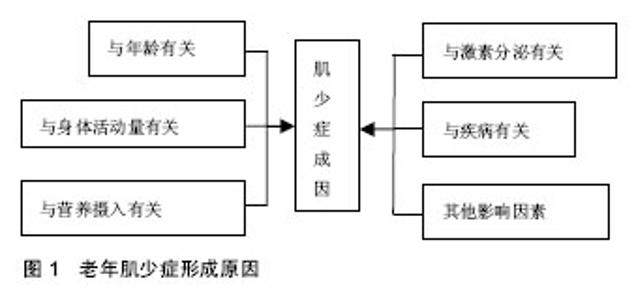
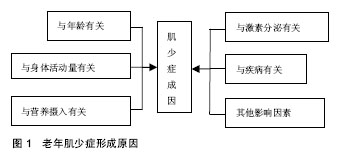
12分为最高,可根据分数来评定受测者日常活动的功能指标,在科学研究和临床实践中均适用[19]。而行走速度因其与失能、跌倒、认知障碍及死亡密切相关,成为近年来热门的研究议题[20]。行走速度的检测是快速、操作简单、可信度极高的测试方法,但距离、起步状态及步速等因素不同,因此操作起来各有差异,一般以小于0.8-1.0 m/s为诊断界线,通过请老年人以正常速度行走5 m取平均值来进行测量[21-22],若低于标准,则判定为生理表现弱,反之亦然。此外,有研究指出,欧盟肌少症工作小组建议采用一般步行速度作为简易快速筛选肌少症的条件,而亚太肌少症事物委员会同样根据不同地域特征、人种差异,提出亚洲人步频速度测量切点为4-6 m速度小于0.8 m/s,并建议用握力加上一般步行速度两者共同作为肌少症筛选条件[7]。事实证明,亚洲人的身高、体型及生理功能等均与西方人存在一定差异,因此为最大限度减小误差,切点的划分应以符合亚洲人实际为宜。 2.2 老年肌少症形成原因及不利影响 2.2.1 老年肌少症形成原因 目前,国内外关于肌少症的成因尚无一致定论,但学者们普遍认为,老年肌少症是由多个因素而非单一因子所造成的,作为一种增龄慢性疾病,肌少症的发病因素复杂多样,见图1。"
| [1] 严嘉枫,纪文宙,周正修.肌少症之流行病学及健康促进介入之探讨[J].身心障碍研究,2015,13(1):9-25.[2] 张淑芳.老年肌少症之诊断与治疗[J].护理杂志, 2014,61(2):101-105.[3] 陈思远,张钦凯.身体活动与肌少症[J].台湾医学, 2014,18(3): 310-316.[4] Cruz-Jentoft AJ, Baeyens JP, Bauer JM,et al.Sarcopenia: Euro-pean consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing.2010; 39( 4):412-423. [5] Fielding RA,Vellas B,Evans WJ,et al.Sarcopenia: an undiag-nosed condition in older adults.Current consensus definition: prev-alence,etiology,and consequences. International working group on sarcopeniaJ Am Med Dir Assoc.2011;12( 4): 249-256. [6] 吴雅汝,詹鼎正.探讨肌少症和骨质疏松症的关系[J].台北市医师公会会刊,2013,57(4):18-21.[7] 杜诗淳,蔡坤维,陈妙文,等.老年人肌少症之预防与照护[J].志为护理, 2015,14(2):62-68.[8] 张珮慈,傅麗蘭.亚洲肌少症之评估指标比较与盛行率介绍[J].台湾体育学术研究,2016.6,(60):145-160.[9] Hida T, Ishiguro N, Shimokata H, et al. High prevalence of sarcopenia and reduced leg muscle mass in Japanese patients immediately after a hip fracture. Gerontol Int.2012;13(2):413-420. [10] Kim SH, Kim TH, Hwang HJ. The relationship of physical activity(PA) and walking with sarcopenia in Korean males aged 60 years and older using the Fourth Korean National Health and Nutrition Examination Survey(KNHANES IV-2, 3) 2008-2009. Arch Gerontol Geriatr.2013;56(3); 472-477. [11] Pongchaiyakul C, Limpawattana P, Kotruchin P, et al. Prevalence of sarcopenia and associated factors among Thai population. J Bone Miner Metab.2013; 31(3):346-350. [12] Cheng Q, Zhu X, Zhang X, et al. A cross-sectional study of loss of muscle mass corresponding to sarcopenia in healthy Chinese men and women: reference values, prevalence, and association with bone mass. J Bone Miner Metab.2014;32(1):78-88. [13] 胡世莲.老年肌少症的评估及干预[J].中国临床保健杂志,2017,20(2): 113-116.[14] 周怡君,张皓翔,詹鼎正.肌少症的评估与预防[J].台湾医学.2014, 18(3):303-309.[15] 吴雅汝,周怡君,詹鼎正.肌少症与衰弱症[J].内科学志,2014,25:131-136.[16] Chen LK, Liu LK, Woo J, et al: Sarcopenia in Asia: consensus report of the Asian working group for sarcopenia. J Am Med Dir Assoc.2014;15:95-101. [17] 付素华.老年肌少症患者护理干预策略[J].当代护士,2018.4,25(10): 9-12.[18] 吴佳佳,邢学农.肌少症研究进展[J].医学综述,2016.02,22(4): 753-756.[19] 余卫,程晓光,袁凌青.肌少症的评估方法[J].中华骨质疏松和骨矿盐疾病杂志,2016.9,9(3):240-246.[20] Abellan van Kan G, Rolland Y, Andrieu S, et al: Gait speed at usual pace as a predictor of adverse outcomes in community- dwelling older people an Internationgal Academy on Nutrition and Aging (IANA) Task Force. J Nutr Health Aging.2009; 13:881-889. [21] Cederholm TE, Bauer JM, Boirie Y, Schneider SM, et al. Toward a definition of sarcopenia. Clin Geriatr Med.2011;27:341-53. [22] 张冰,李维辛.老年人糖尿病相关性肌少症的研究进展[J].中国康复理论与实践,2016,22(11):1294-1297.[23] 林泰祐,林麓娟.阻力训练对减缓老年人骨骼肌减少症的效益[J].中华体育季刊,2011,25(1):10-21.[24] Drummond MJ, Miyazaki M, Dreyer HC, et al. Expression of growth-related genes in young and older human skeletal muscle following an acute stimulation of protein synthesis. J Appl Physiol (1985).2009, 106(4):1403-1411. [25] Frontera WR,Hughes VA,FieldingRA,et al.Aging of skeletal muscle: a 12-yr longitudinal study.J Appl Physiol (1985).2000; 88(4):1321-1326. [26] 林雨薇,钱桂玉,许美智.老年人肌肉减少症的成因与影响[J].大专体育,2010.10,(110):85-91.[27] 虚佳文,陈怡茹,黄国晋.老人肌少症肥胖症[J].台湾医学,2014,18(3): 317-324.[28] Layman DK. Dietary Guidelines should reflect new under-standings about adult protein needs. Nutr Metabo.2009;6:12. [29] Buitrago CG,Arango NS,BolandRL.25(OH) 2D3-dependentmodulation of Akt in proliferating and differentiating C2C12 skele-tal muscle cells. J Cell Biochem. 2012;113( 4):1170-1181. [30] Schiafflno S, Dyar KA, Ciciliot S, et al. Mechanisms regulating skeletal muscle growth and atrophy. FEBS J.2013;280(170): 4294-4314. [31] Morley JE, Malmstrom TK. Frailty, sarcopenia, and hormones. Endocrinol Metab Clin North Am.2013; 42:391-405. [32] Sipilä S, Narici M, Kjaer M,et al. Sex hormones and skeletal musdomized, double-blind, placebo-controlled study. J Clin Endocrinol Metab.2010;95(2):639-650. [33] Cesari M, Kritchevsky SB, Baumgartner RN, et al: Sarcopenia, obesity, and inflammation- results from the Trial of Angiotensin Converting Enzyme Inhibition and Novel Cardiovascular Risk Factors study. Am J Clin Nutr, 2005;82:428-34. [34] Jo E, Lee SR, Park BS, Kim JS: Potential mechanisms underlying the role of chronic in?mmation in age-related muscle wasting. Aging Clin Exp Res.2012;24:412-422. [35] Collins-Hooper H, Woolley TE, Dyson L, et al: Age-related changes in speed and mechanism of adult skeletal muscle stem cell migration. Stem Cells.2012; 30:1182-1195. [36] Wagatsuma A, Sakuma K. Vitamin D signaling in myogenesis: potential for treatment of sarcopenia.BiomedRes Int.2014;2014: 121254. [37] Dyck DJ, Heigenhauser GJ, Bruce CR: The role of adipokines as regulators of skeletal muscle fatty acid metabolism and insulin sensitivity. Acta Physiol (Oxf), 2006;186:5-16. [38] Kim KS, Park KS, Kim MJ, et al. Type 2 diabetes is associated with low muscle mass in older adults. Geriatr Gerontol Int.2014; 14(Suppl 1):115-121. [39] Akpinar TS, Tayfur M, Tufan F, et al. Uncomplicated diabetes does not accelerate age-related sarcopenia. Aging Male.2014;17(4): 205-210. [40] 江柏欣,陈昱宏.肌少症的诊断、成因与临床重要性之探讨[J].台湾家医志,2014,24:1-8.[41] Argilés JM, Busquets S, Felipe A,et al. Muscle wasting in cancer and ageing: cachexia versus sarcopenia. Adv Gerontol. 2006;18: 39-54. Review. [42] Chin SO, Rhee SY, Chon S,et al. Sarcopenia is independengtly associated with cardiovascular disease inolder Korean adults: the Korea National Health and Nutrition Examination on Survey (KNHANES) from, PLoS One. 2013;8(3):e60119. [43] Yu R, Leung J, Woo J: Incremental predictive value of sarcopenia for incident fracture in an elderly Chinese cohort: results from the osteoporotic fractures in men (MrOs) study. J Am Med Dir Assoc. 2014;15:551-558. [44] Fried LP, Walston JD, Ferruci L. Frailty. In: Halter JB, Ouslander JG, Tinetti ME, el al.Hazzard's Geriatric Medicine and Gerontology. 6th ed. New York: McGrall-Hill.2009:631-645. [45] Evans WJ, Campbell WW. Sarcopenia and age-related changes in body composition and functional capacity. J Nutr.1993;123 (2 Suppl):465-468. [46] Peterson MD, Rhea MR, Sen A, et al: Resistance exercise for muscular strength in order adults: a meta-analysis. Ageing Res Rev.2010;9:226-237. [47] Peterson MD, Sen A, Gordon PM.Influence of resistance exercise on lean body mass in aging adults: a meta-analysis. Med Sci Sports Exerc.2011; 43:249-258. [48] Crocker T, Forster A, Young J, et al: Physical rehabilitation for older people in long-term care. Cochrane Database Syst Rev. 2013;2:CDOO4294. [49] Abdulla H, Phillips B, Smith K, et al. Physiological mechanisms of action of incretin and insulin in regulating skeletal muscle metabolism. Curr Diabetes Rev.2014;10(5):327-335. [50] Ramel A, Arnarson A, Geirsdottir OG, et al. Glomerular filtration rate after a 12-wk resistance exercise program with post-exercise protein ingestion in community dwelling elderly. Nutrition.2013; 29:719-23. [51] Polly P,Tan TC.The role of vitamin D in skeletal and cardiac muscle fun. Front Physiol.2014;5:145. [52] Basaria S, Coviello AD, Travison TG, et al: Adverse events associated with testosterone administration. N Engl J Med.2010; 363:109-22. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [3] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [4] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [5] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [6] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [7] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [8] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [9] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [10] | Li Jun, Zuo Xinhui, Liu Xiaoyuan, Zhang Kai, Han Xiangzhen, He Huiyu, . Effect of over expression of miR-378a on osteogenic and vascular differentiation of bone marrow mesenchymal stem cell sheet [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(31): 4939-4944. |
| [11] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [12] | Wang Zhen, Lin Haiqi, He Fei, Lin Wentao. Exercise activates skeletal muscle satellite cells: exercise prevention and treatment for age-related sarcopenia and muscle injury [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(23): 3752-3759. |
| [13] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [14] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| [15] | Mo Jianling, He Shaoru, Feng Bowen, Jian Minqiao, Zhang Xiaohui, Liu Caisheng, Liang Yijing, Liu Yumei, Chen Liang, Zhou Haiyu, Liu Yanhui. Forming prevascularized cell sheets and the expression of angiogenesis-related factors [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3479-3486. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||