Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (14): 2284-2289.doi: 10.3969/j.issn.2095-4344.0744
Previous Articles Next Articles
Research and application of the reamer-irrigator-aspirator
Li Hai-feng, Gu San-jun, Yin Qu-dong
- Department of Orthopaedics, the Ninth People’s Hospital of Wuxi, Wuxi 214062, Jiangsu Province, China
-
Received:2017-12-22Online:2018-05-18Published:2018-05-18 -
Contact:Yin Qu-dong, Chief physician, Department of Orthopaedics, the Ninth People’s Hospital of Wuxi, Wuxi 214062, Jiangsu Province, China -
About author:Li Hai-feng, Master, Attending physician, Department of Orthopaedics, the Ninth People’s Hospital of Wuxi, Wuxi 214062, Jiangsu Province, China
CLC Number:
Cite this article
Li Hai-feng, Gu San-jun, Yin Qu-dong . Research and application of the reamer-irrigator-aspirator[J]. Chinese Journal of Tissue Engineering Research, 2018, 22(14): 2284-2289.
share this article

2.1 扩髓-灌洗-吸引器的结构和性能 扩髓-灌洗-吸引器前方为直径12-19 mm的空心多孔锥形金属钻头,中央部分的内层为长度360-520 mm的空心钻体,外层为塑料收集管,后方有锁夹盖和和钻体封口。收集管后部有进水口、引流口。钻体封口位于钻体最后方,防止灌洗液从空心的钻体后方溢出。钻体后方与电钻连接后用可滑动的锁夹盖套住并锁定,见图1。进水口通过塑料管连接灌洗生理盐水袋。引流口与负压引流装置之间连接一个带有过滤网的塑料瓶,滤网收集颗粒状植骨材料,收集瓶内收集滤液[1-4]。由于钻头非常锋利,可打磨皮质骨,故滤网中收集的颗粒状植骨材料,为大量松质骨和部分皮质骨的混合物。"

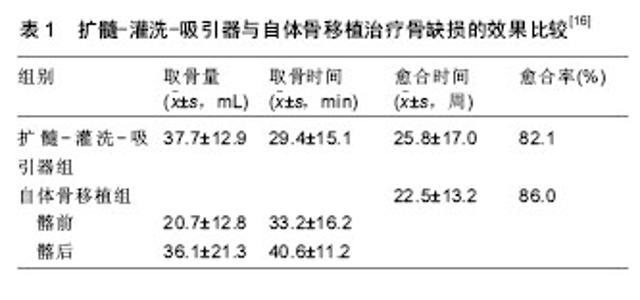
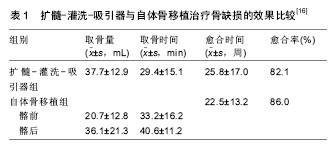
普通钻头扩髓带来二大不利影响,一是高压致骨髓内容物向组织内渗透,引起炎症反应和脂肪回流致肺栓塞;二是钻头高速转动打磨皮质骨产生高温致骨热坏 死[5-12]。扩髓-灌洗-吸引器钻头和钻体均为空心结构,持续性罐洗负压吸引具有减压和降温作用,可减少扩髓带来的不利影响。Higgins等[10]利用尸体胫骨比较扩髓-灌洗-吸引器和传统方法扩髓在胫骨远端的降温和降压效果,结果显示扩髓-灌洗-吸引器组最高温度为(42± 9.1) ℃,明显低于传统方法组(58.7±15.9) ℃(P=0.025),即有明显降温效果,但降压变化与理论上不一致,他们认为是引流管堵塞所致。Wang等[12]采用猪股骨实验研究,一侧行扩髓-灌洗-吸引器逆行扩髓(扩髓-灌洗-吸引器组),对侧AO标准方法扩髓(AO组),然后行髓内钉固定,测量肺动脉压、平均动脉压、部分动脉氧压和心输出量等指标,结果显示扩髓-灌洗-吸引器组在减少脂肪栓塞的生理指标和脂肪栓子数方面优于AO组。Pap等[13]采用绵羊制成医源性单侧肺损伤模型,测量肺通透性比较扩髓-灌洗-吸引器和传统方法扩髓的全身反应效果,结果显示,扩髓-灌洗-吸引器组的全身炎症衰减指 标——尿素/蛋白比(91.5)低于传统方法扩髓组(256.7),扩髓-灌洗-吸引器组的D-二聚体水平较低、肺通透性增加。Miller等[2]利用在犬股骨比较不扩髓髓内钉固定(UR组),传统方法扩髓髓内钉固定(SR组)和扩髓-灌洗-吸引器扩髓髓内钉固定(扩髓-灌洗-吸引器组),测量在扩髓和插入髓内钉过程中微栓子通过颈动脉的数量和大小,处死动物后大脑组织行免疫染色和微梗死体积测定,结果显示3组通过颈动脉的总栓塞负荷分别为0.049,0.045,0.013 mL,UR组和SR组微栓子的数量和大小相近,但扩髓-灌洗-吸引器组较大栓子(> 200 μm)数量更少,与其他两组比较差异显著(P=0.03),脑组织病理检查证实存在颗粒栓塞,组织学分析表明所有组应激相关蛋白均增加;与UR和SR相比,扩髓-灌洗-吸引器组有更少脑部栓子和较少应激。因此扩髓-灌洗-吸引器具有降压、降温、减轻炎症反应和减少脂肪栓塞作用,可减少扩髓的不利影响[10-14]。 2.2 手术方法 目前仅应用于股骨和胫骨。根据具体情况股骨选择顺行或逆行法扩髓,仰卧或俯卧位;胫骨仅顺行法扩髓,仰卧位。需要在C臂机透视下进行。首先体表测量股骨峡部髓腔直径,用不透射线的毫米尺定位于股骨峡部髓腔,透视测量髓腔最小直径,选用的扩髓-灌洗-吸引器钻头直径比髓腔内皮质直径要大1.0- 1.5 mm,最大不超过2 mm,以便能打磨出松质骨和部分皮质骨[4-5]。股骨顺行法从转子间梨状窝开孔,股骨逆行法从髁间窝后交叉韧带止点前开孔。经正侧位双平面透视验证下插入导针位置正确。在台下先完成扩髓-灌洗-吸引器组装连接,然后沿导针插入,在扩髓-灌洗-吸引器进入髓腔的操作顺序为:钻入-回退-暂停,重复多次缓慢进行扩髓。为了取得足够植骨材料,导针远端需要预弯以到达股骨远端的内外侧髁部,而且每次只能沿导针单轨通道进行扩髓。术中需频繁透视以避免股骨前皮质扩髓过度以及偏心扩髓,发生医源性穿孔或骨折。停止扩髓后仍有出血,故建议停止负压吸引。采集足够自体骨后停止扩髓,取出扩髓-灌洗-吸引器,将收集袋的自体骨注入样本杯测量储存备用。闭合切口后绷带加压包扎。扩髓后骨皮质变薄者,建议术后制动4- 6周。与顺行法进针相比,股骨逆行法进针时同心轨迹更多,可避免仰卧位多次摆放体位、准备及铺巾,尤其适用于肥胖和股骨近端皮肤损伤患者[4]。 2.3 适应证和应用效果 2.3.1 髓内钉固定的特殊扩髓方法 髓内钉是股骨和胫骨干骨折内固定的金标准,扩髓是髓内钉固定的标准技术,扩髓后可使用较粗大髓内钉,增加内固定稳定性;另一方面,扩髓还迫使骨髓进入断端、引起折端血肿反应,可以促进骨折端成骨。但是,标准的扩髓方法也存在增加髓腔压力,引起全身炎症反应和栓塞风险,以及产高热致骨热坏死等不利影响[1-4]。采用扩髓-灌洗-吸引器扩髓,具有降压、降温、减轻炎症反应和减少脂肪栓塞作用,可减少标准扩髓方法的不利影响[10-14]。 2.3.2 获取大量自体骨移植方法 自体髂骨移植是骨移植的金标准,但取骨部位疼痛、麻木等并发症发生率为6%-30%[15-19],而且,当骨缺损较大时,髂嵴获取的自体骨数量仍然不够。长骨骨髓富含松质骨和基质干细胞,具有取骨潜力,扩髓-灌洗-吸引器则提供可从长骨髓腔获取大量自体骨移植的一种手段。研究显示一侧髂后嵴可获取平均36 mL、髂前嵴平均26 mL体积的取骨 量[1-3],而使用扩髓-灌洗-吸引器在一侧股骨可获取平均67 mL体积(范围40-90 mL)、一侧胫骨平均37.5 mL体积的骨颗粒[3,16,18]。骨颗粒为松植骨和皮质骨混合物。研究显示,骨颗粒和滤液中均含有具有分化潜能的骨髓基质干细胞和多种成骨因子[2-5,18-20],骨髓基质干细胞的特征和表型与来源于髂骨或脂肪的基质干细胞一致,均可诱导成骨[2-5,18-21];成骨因子包括骨形态发生蛋白2、成纤维细胞生长因子、胰岛素样生长因子1、血小板源性生长因子和转化生长因子[19-25]。Porter等[22]收集5例行全髋关节置换患者股骨近端通过扩髓-灌洗-吸引器获取滤液(230±200) mL,采用Ficoll密度梯度离心分离出单个核细胞(6.2±5.2)×109 L-1,上清液中含成纤维细胞生长因子2、胰岛素样生长因子1和潜在的转化生长因子β1,但骨形态发生蛋白2低于检测水平;细胞包括成纤维细胞,为基质干细胞,体外可诱导分化成骨细胞、脂肪细胞和软骨细胞,相比于从骨颗粒中培养的骨生长细胞,滤液中细胞虽然也有成软骨能力,但对成骨细胞培养更敏感。Churchman等[23]研究显示,扩髓-灌洗-吸引器获取人体股骨干集落形成成纤维细胞中基质干细胞的中位数为314 333,相当于约1 L髂骨抽吸骨髓中基质干细胞数量。Cox等[24]比较扩髓-灌洗-吸引器与髂骨骨髓的基质干细胞数量、表型和分化能力,扩髓-灌洗-吸引器包括骨颗粒部分和液体部分,骨颗粒采用胶原酶消化处理,对纤维母细胞集落形成单位进行计数,其表型用流式细胞仪(CD33、CD34、CD45、CD73、CD90、CD105)鉴定,结果显示扩髓-灌洗-吸引器组的基质干细胞数量与髂骨骨髓组相当,表型与其他已知来源一致,3组的集落形成单位中位数:髂骨骨髓组为8.5/200 μL,扩髓-灌洗-吸引器液体组为19.5/200 μL,扩髓-灌洗-吸引器骨颗粒组为109/200 μL;3组总细胞数:髂骨骨髓组为920,扩髓-灌洗-吸引器液体组为 114 983,扩髓-灌洗-吸引器骨颗粒组为12 785;扩髓-灌洗-吸引器滤液中也含有大量基质干细胞,不需要酶消化就可提取,不需要细胞扩增就能用于骨修复。Van等[25]利用猪比较从扩髓-灌洗-吸引器和髂骨获取自体骨行细胞培养研究表明,扩髓-灌洗-吸引器骨移植的细胞基质矿化明显高于髂骨移植,二者差异有统计学意义(P=0.031 3),即扩髓-灌洗-吸引器骨移植提供了优越髂骨骨移植的成骨性能。Hammer等[26]采用动物实验比较扩髓-灌洗-吸引器扩髓和常规方法扩髓、髓内钉固定对长骨骨折愈合的影响,结果显示扩髓-灌洗-吸引器扩髓加植骨的刚度和扭转强度优于常规方法扩髓(P < 0.05),扩髓-灌洗-吸引器扩髓加植骨的骨痂面积明显多于常规方法扩髓(P < 0.05)。 Dawson等[16]多中心前瞻性随机对照研究共133例骨不连或节段性骨缺损行扩髓-灌洗-吸引器与髂前、髂后自体骨移植的效果,结果显示,自体骨移植组髂前取骨量明显少于髂后取骨和扩髓-灌洗-吸引器组(P < 0.001),扩髓-灌洗-吸引器取骨时间明显少于髂后(P=0.005);尽管扩髓-灌洗-吸引器一套装置费用较高,但髂后取骨手术时间较长,所需额外花费较多,总体上应用扩髓-灌洗-吸引器治疗患者的费用较髂后取骨并没有明显增加;自体骨移植组与扩髓-灌洗-吸引器组的愈合率和愈合时间相当(P > 0.05),见表1;二者的骨不愈合率和感染需要再次手术等并发症及取骨部位并发症比较均无差异(P > 0.05);但扩髓-灌洗-吸引器患者供区疼痛评分明显低于自体髂骨移植骨(P < 0.05)。结果提示,扩髓-灌洗-吸引器自体骨移植实现了与自体髂骨移植相似的骨愈合效果,但供区疼痛明显轻而少;扩髓-灌洗-吸引器取骨较髂前获取更大体积的移植骨,较髂后更短取骨时间,对于需要大量自体骨的患者来讲,扩髓-灌洗-吸引器取骨成本更低。Miller等[2]报道将扩髓-灌洗-吸引器骨颗粒、滤液和地塞米松混合植骨治疗13例长骨骨折骨不连和骨缺损,均骨愈合。Stafford[27]报道25例共27处节段性骨缺损性骨不连,其中胫骨19处,股骨8处,15处为开放性骨折合并骨缺损,12处为感染或扩创导致骨缺损,平均缺损长5.8 cm,采用诱导膜技术治疗,第二阶段手术通过扩髓-灌洗-吸引器获取自体骨植入诱导膜内,随访1.5年,80%骨不连部位获得骨愈合,无扩髓-灌洗-吸引器相关并发症。 2.3.3 治疗骨髓炎 对于骨髓炎,需要对病灶行广泛彻底清创、灌洗及敏感抗生素治疗。利用扩髓-灌洗-吸引器行髓腔清创和冲洗,可清除髓腔感染病灶,降低髓腔感染向周围软组织和血液循环播散的风险,因此可以用来治疗髓内型骨髓炎或骨感染[26-32]。Kanakaris等[28]报道应用扩髓-灌洗-吸引器扩髓后将抗生素骨水泥棒置入髓腔治疗24例股骨和胫骨骨髓炎,骨髓炎Cierny-Mader分型:1A型18例,3A型4例,4A型1例,1B型1例,同时根据感染情况行髓腔外清创,局部予有限固定,平均随访21个月,96%患者在随访期间没有感染复发,只有1例股骨骨髓炎术后1年出现感染复发,该例患者局部未应用抗生素骨水泥棒置入,再次扩髓-灌洗-吸引器清创、置入抗生素骨水泥棒治疗,术后随访33个月没有出现感染复发;1例扩髓过程中发生医源性股骨远端不全性骨折,予制动后骨折愈合;1例股骨骨髓炎感染控制良好,但术后8个月因肺栓塞死亡;另1例胫骨骨髓炎术后2周因患者主动要求行胫骨近端截肢保留膝关节,此时患者并无感染复发或加重。结果显示,扩髓-灌洗-吸引器对髓腔进行有效清创和冲洗,可以根除感染病灶,治疗效果与以往文献报道的其他治疗骨髓炎方法相当。Gualdrini等[29]报道治疗36例股骨和胫骨慢性骨感染,Cierny-Mader分型2A,治疗包括扩髓-灌洗-吸引器扩髓和对侧骨开窗、术后置管灌洗,平均随访2.9年,83.2%患者获得愈合(愈合标准为无临床、体液和放射学骨髓部位感染迹象)。Granes等[30]回顾分析43例胫骨和股骨骨干慢性骨髓炎(44处)应用扩髓-灌洗-吸引器治疗,感染持续时间平均13.2年,在10年的随访过程中,83%骨髓炎患者未复发。Zalavras等[7]报道11例创伤性股骨和胫骨骨髓炎采用扩髓-灌洗-吸引器清创和灌洗治疗,平均随访9个月无感染复发。 2.3.4 治疗骨肿瘤 股骨是恶性骨肿瘤最常见转移部位之一,髓内钉固定是预防和治疗股骨恶性骨肿瘤常用方法[1,3,8,31]。当股骨没有发生病理性骨折风险时,行髓内钉预防性固定,可减轻患者疼痛、避免完全骨折,以及提高患者生活质量[8,32]。但是,在没有骨折的股骨肿瘤患者扩髓和插入髓内钉发生脂肪栓塞和肿瘤栓塞,导致低血压、低氧血症、心脏骤停、神志不清和猝死的风险较高[8,32]。血流动力学记录到,髓内钉治疗股骨病理性骨折术中有患者发生继发转移性肺功能受损的发生率为10.5%-13%;经颅多普勒超声检测到,胫骨或股骨肿瘤性骨折行扩髓时骨髓和脂肪致患者继发脑膜中动脉栓塞的发生率为20%[8,32]。扩髓-灌洗-吸引器不仅可清除位于髓腔内的骨肿瘤,而且具有减少扩髓时发生脂肪栓塞和肿瘤栓塞的风险。因此,扩髓-灌洗-吸引器结合髓内钉固定可以预防和治疗股骨或胫骨恶性肿瘤。Cipriano等[8]报道21例股骨恶性肿瘤采用扩髓-灌洗-吸引器扩髓、交锁髓内钉固定治疗,每例患者通过扩髓-灌洗-吸引器产生平均体积为75 mL扩髓物,其中肿瘤平均含量为16.7 mL,没有发生栓塞,虽然术中2例发生钻头颈部断裂,后来取出,患者并无不良影响。结果显示,股骨肿瘤或病理性骨折采用扩髓-灌洗-吸引器结合髓内钉固定,扩髓-灌洗-吸引器可清除髓腔肿瘤组织,防止恶性细胞的全身传播,可以减少远处转移的风险。 2.3.5 清除髓腔骨水泥 髋关节置换后股骨侧骨水泥假体的翻修需要清除髓腔内骨水泥;负载抗生素骨水泥填塞髓腔是治疗髓腔感染或髓内型骨髓炎的有效方法,感染控制后部分患者需要取出髓腔内填塞的骨水泥。以往因缺乏有效工具,彻底清除髓腔内残留骨水泥较为困难,有时甚至需要将骨骼开窗才能取出残留骨水泥。扩髓-灌洗-吸引器钻头非常锋利,是清除髓腔残留骨水泥一种有效方法[1,4-6,9]。Lowe等[9]报道应用扩髓-灌洗-吸引器清除清除髓腔骨水泥3例,效果良好,但目前报道很少,主要是应用病例较少的缘故。 2.4 并发症和缺陷 主要并发症是医源性骨折或穿孔和出血较多,其次是异位骨化、钻头断裂或残留和感染 等[2-8,33-37]。取骨部位切口感染发生率极低,但出血或潜在出血较多,有诱发心血管疾病报道[36]。Cox等[5]总结87例应用扩髓-灌洗-吸引器治疗者并发症发生率为3.45%。McCall等[33]报道21例长骨节段性骨缺损采用扩髓-灌洗-吸引器治疗,异位骨化发生率9.52%。绝大多数文献报道,扩髓-灌洗-吸引器并发症发生率为3%-10%,大多数的并发症可采取保守方法得到控制。但是,Jakma等[34]认为扩髓-灌洗-吸引器并发症发生率比绝大多数文献报道的要高,他们报道32例节段性骨缺损骨不连或骨髓炎应用扩髓-灌洗-吸引器治疗,扩髓-灌洗-吸引器并发症发生率为31%(包括骨缺损不愈合、肺栓塞、心肌梗死和裂缝骨折等),其中术后疼痛发生率为18%,认为扩髓-灌洗-吸引器治疗骨不连和骨髓炎虽然总体上疗效较好,但存在学习曲线,初期阶段应用的并发症发生率较高,术前充分准备、细致手术技术和围手术期密切监测可以降低并发症发生率。 扩髓-灌洗-吸引器为一次性装置,使用费用较大;术中需要多次透视,X射线辐射较多;骨骼畸形、髓腔较小和小于12岁的儿童为禁忌证,故适应证有限;出血或潜在出血较多,有输血可能,也增加了使用成本,这些缺陷增加了扩髓-灌洗-吸引器的推广难度。 "
| [1] Green J.History and development of suction-irrigation-reaming.Injury.2010;41(41 Supple2): S24-31.[2] Miller MA,Ivkovic A,Porter R,et al.Autologous bone grafting on steroids:preliminary clinical results.A novel treatment for nonunions and segmental bone defects.Int Orthop. 2011; 35(4):599-605.[3] Lowe JA,Rocca GJ,Murtha Y,et al.Complications associated with negative pressure reaming for harvesting autologous bone graft:a case series.J Orthop Trauma.2010;24(1):46-52.[4] Barlow,Brian T,Kevin M.Technique and indications for the retrograde use of the reamer-irrigator-aspirator.Current Orthopaedic Practice.2014;25(Issue)183-188.[5] Cox G,Jones E,Mcgonagle D,et al.Reamer-irrigator-aspirator indications and clinical results: a systematic review.Inter Orthopaedics.2011;35(7):951-956.[6] Kuhn KM,Barlow BT,Dromsky D.The Reamer-Irrigator-Aspirator: roles and evidence supporting its use in current orthopaedic practice.Surgery Curr Res. 2014; 4(2):167-172.[7] Zalavras CG,Singh A,Patzakis MJ.Novel technique for medullary canal debridement in tibia and femur osteomyelitis.Clin Orthop Relat Res.2007;461(461):31-34.[8] Cipriano CA,Arvanitis LD,Virkus WW.Use of the reamer-irrigator-aspirator may reduce tumor dissemination during intramedullary fixation of malignancies.Orthopedics. 2012;35(1):48-52.[9] Lowe JA,Vosburg C,Murtha YM,et al.A new technique for removing intramedullary cement.J Orthop Trauma. 2011; 25(12):762-766.[10] Higgins TF,Casey V,Bachus K.Cortical heat generation using an irrigating/aspirating single-pass reaming vs conventional stepwise reaming.J Orthop Trauma.2007;21(3):192-197.[11] Husebye EE,Lyberg T,Madsen JE,et al.The influence of a one-step reamer-irrigator-aspirator technique on the intramedullary pressure in the pig femur.Injury. 2006;37(10): 935-940.[12] Wang RY,Li R,Zdero R,et al.The physiologic and pathologic effects of the reamer irrigator aspirator on fat embolism outcome:an animal study.J Orthopaedic Trauma. 2012;26(9): 132-137.[13] Pape HC,Zelle BA,Hildebrand F,et al.Reamed femoral nailing in sheep:does irrigation and aspiration of intramedullary contents alter the systemic response?.J Bone Joint Surg(Am). 2005;87(11):2515-2522.[14] Volgas DA,Burch T,Stannard JP,et al.Fat embolus in femur fractures:a comparison of two reaming systems.Injury. 2010; 41(Suppl 2):S90-93. [15] Han F,Peter L,Lau ETC,et al.Reamer Irrigator Aspirator bone graft harvesting: complications and outcomes in an Asian population.Injury.2015;46(10):2042-2051.[16] Dawson J,Kiner D,Nd GW,et al.The reamer irrigator aspirator as a device for harvesting bone graft compared with iliac crest bone graft:union rates and complications.J Orthopaedic Trauma.2014;28 (10):584-590.[17] Beck A,Nehrbass D,Stoddart MJ,et al.The use of Reamer Irrigator Aspirator (RIA) autograft harvest in the treatment of critical-sized iliac wing defects in sheep:investigation of dexamethasone and beta-tricalcium phosphate augmentation. Bone.2013;53(2):554-565.[18] Qvick LM,Ritter CA,Mutty CE,et al.Donor site morbidity with reamer-irrigator-aspirator (RIA) use for autogenous bone graft harvesting in a single centre 204 case series.Injury. 2013; 44(10):1263.[19] Calori GM, Colombo M,Mazza EL,et al.Incidence of donor site morbidity following harvesting from iliac crest or RIA graft. Injury. 2014;45(Suppl 6):S116-120.[20] Jakoi AM,Iorio JA,Cahill J.Autologous bone graft harvesting: a review of grafts and surgical techniques.Musculoskel Surg. 2015;99(3:171-178.[21] Toosi S,Naderi-Meshkin H,Kalalinia F,et al.Comparative characteristics of mesenchymal stem cells derived from Reamer-irrigator-aspirator,iliac crest bone marrow,and adipose tissue.Cell Mol Biol.2016;62(10):68-74.[22] Porter RM,Liu F,Pilapil C,et al.Osteogenic potential of reamer irrigator aspirator (RIA) aspirate collected from patients undergoing hip arthroplasty.J Orthop Res.2009;27(1):42-49.[23] Churchman SM,Kouroupis D,Boxall SA,et al.Yield optimisation and molecular characterisation of uaspirator waste bag.Eur Cell Mater.2013;13(26):252-262.[24] Cox G,McGonagle D,Boxall SA,et al.The use of the reamer-irrigator-aspirator to harvest mesenchymal stem cells.J Bone Joint Surg(Br).2011;93B(4):517-524.[25] Van dBR, Blokhuis TJ.Increased osteogenic capacity of Reamer/Irrigator/Aspirator derived mesenchymal stem cells.Injury.2014;45(12):2060.[26] Hammer TO,Wieling R,Green JM,et al.Effect of re-implanted particles from intramedullary reaming on mechanical properties and callus formation.A laboratory study.J Bone Joint Surg(Br).2007; 89B(11):1534-1538.[27] Stafford PR,Norris BL.Reamer-irrigator-aspirator bone graft and bi Masquelet technique for segmental bone defect nonunions:a review of 25 cases.Injury.2010;41(Suppl 2):S72.[28] Kanakaris N,Gudipati S,Tosounidis T,et al.The treatment of intramedullary osteomyelitis of the femur and tibia using the Reamer-Irrigator-Aspirator system and antibiotic cement rods. Bone Joint J.2014;96B:783-788.[29] Gualdrini G,Barchetti M,Trono M,et al.Intramedullary reaming in the treatment of chronic osteomyelitis of the femur and tibia.La Chirurgia Degli Organi Di Movimento.2000;85(3):257.[30] Granes R,Maurer TB,Mueller U,et al.Intrameduallary reaming as treatment of chronic osteomyelitis of long bones-a 10 to 15 years follow-up.J Veterinary Emergency Critical Care. 2006; 24(2):134-134.[31] Tosounidis TH,Calori GM,Giannoudis PV.The use of Reamer-irrigator-aspirator in the management of long bone osteomyelitis:an update.Eur J Trauma Emerg Surg. 2016; 42(4):417-423.[32] Dalgorf D,Borkhoff CM,Stephen DJ,et al.Venting during prophylactic nailing for femoral metastases:current orthopedic practice.Can J Surg.2003;46(6):427-431.[33] McCall TA,Brokaw DS,Jelen BA,et al.Treatment of large segmental bone defects with reamer-irrigator-aspirator bone graft:technique and case series.Orthop Clin North Am. 2010; 41(1):63-73.[34] Jakma TSC,Roling MA,Punt B,et al.More adverse events than expected in the outcome after use of the reamer-irrigator-aspirator.Eur J Trauma Emerg Surg. 2013; 40(3):337-341.[35] Marchand LS,Rothberg DL,Kubiak EN, et al.Is This autograft worth it?: The blood loss and transfusion rates associated with reamer irrigator aspirator bone graft harvest.J Orthop Trauma.2017;31(4):205-209.[36] Donders JC,Baumann HM,Stevens MF,et al. Hemorrhagic-induced cardiovascular complications during reamer-irrigator-aspirator-assisted femoral nonunion treatment.J Orthop Trauma.2016;30(9):e294-298.[37] Sagi HC,Young ML,Gerstenfeld L,et al.Qualitative and quantitative differences between bone graft obtained from the medullary canal (with a Reamer/Irrigator/Aspirator) and the iliac crest of the same patient.J Bone Joint Surg(Am). 2012; 94(23):2128-2135.[38] Kuehlfluck P,Moghaddam A,Helbig L,et al.RIA fractions contain mesenchymal stroma cells with high osteogenic potency.Injury.2015;46(Suppl 8):S23-32. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [3] | Hua Haotian, Zhao Wenyu, Zhang Lei, Bai Wenbo, Wang Xinwei. Meta-analysis of clinical efficacy and safety of antibiotic artificial bone in the treatment of chronic osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 970-976. |
| [4] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [5] | Li Xingping, Xiao Dongqin, Zhao Qiao, Chen Shuo, Bai Yiguang, Liu Kang, Feng Gang, Duan Ke. Preparation and properties of copper-loaded antibacterial functional film on titanium surface [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 553-557. |
| [6] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [7] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [8] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [9] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [10] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [11] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [12] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [13] | Zeng Xianghong, Liang Bowei. A new strategy for the treatment of osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 431-437. |
| [14] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [15] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||