Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (21): 3393-3400.doi: 10.3969/j.issn.2095-4344.0516
Previous Articles Next Articles
Microvesicles and exosomes in the lung diseases
Luo Deng1, Ran Wen-zhuo2, Ye Ying-chun1, Gao Ling1
- 1Department of Endocrinology, Eastern Branch of Renmin Hospital, Wuhan University, Wuhan 430000, Hubei Province, China; 2Clinical Laboratory, Wuhan No. 1 Hospital, Wuhan 430023, Hubei Province, China
-
Revised:2018-03-27Online:2018-07-28Published:2018-07-28 -
Contact:Ye Ying-chun, Master, Attending physician, Department of Endocrinology, Eastern Branch of Renmin Hospital, Wuhan University, Wuhan 430000, Hubei Province, China -
About author:Luo Deng, Ph.D., Attending physician, Department of Endocrinology, Eastern Branch of Renmin Hospital, Wuhan University, Wuhan 430000, Hubei Province, China -
Supported by:Independent Research Project of Wuhan University of China, No. 2042017kf0084; Natural Science Foundation of Hubei Province, No. 2018CFB230
CLC Number:
Cite this article
Luo Deng, Ran Wen-zhuo, Ye Ying-chun, Gao Ling. Microvesicles and exosomes in the lung diseases[J]. Chinese Journal of Tissue Engineering Research, 2018, 22(21): 3393-3400.
share this article

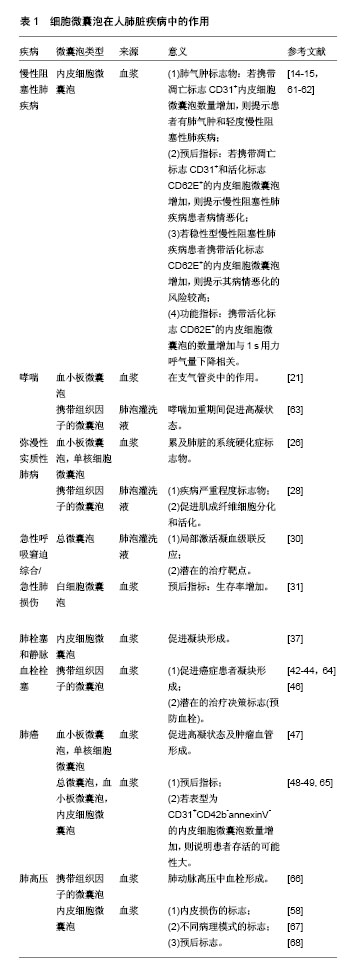
2.1 微囊泡/外泌体的形成和特性 生理和病理情况下,多种细胞(如上皮细胞、成体干细胞、肿瘤细胞等)都可产生微囊泡/外泌体[2]。细胞在受到物理化学刺激后,胞吞形成早期胞内体,随着与高尔基体和内质网的相互作用,包膜内发生内陷,形成多囊泡体,多囊泡体与细胞膜融合后再通过胞吐作用,将多囊泡体中的囊泡释放到胞外而形成了直径不同的微囊泡(100-2 000 nm)或外泌体(40-100 nm)。外泌体的分泌依赖于骨架蛋白的活化,微囊泡的释放除了依赖于骨架蛋白活化外,还需借助于胞内钙离子浓度。微囊泡富含磷脂酰丝氨酸,外泌体富含四分子交联体蛋白(CD63、CD81和CD9)、热休克蛋白(HSP60、HSP70和HSP90)、肿瘤易感基因101 (TSG101)等特异性表面分子,微囊泡/外泌体可以通过细胞的生物活性分子(胞内体蛋白、膜蛋白、核酸等)直接与受体细胞之间实现信息传递[3]。 2.2 微囊泡/外泌体的功能 微囊泡/外泌体的主要功能是细胞间的信息传递,由于其具有脂质双分子层包膜,可有效避免所运载生物活性物质的降解,通过受体与靶细胞相互作用或直接与细胞膜融合或胞吞作用,将内含物传递到受体细胞。具体主要通过以下几种方式作用于受体细胞。 2.2.1 作为复合物信号直接刺激靶细胞 血小板来源的微囊泡因其膜上具有丰富的磷脂酰丝氨酸,因此在凝血过程中可为凝血因子的聚集提供磷脂表面[4-6]。血小板活化后,会释放携带组织因子的微囊泡,这些微囊泡可与巨噬细胞、中性粒细胞和其他表达P-选择素的血小板相互作用[7]。 2.2.2 在细胞间传递受体或活性脂质 微囊泡可以将黏附分子CD41从血小板转移到内皮细胞或肿瘤细胞中[8-9],便赋予内皮细胞或肿瘤细胞黏附特性。源于肿瘤细胞的微囊泡携带Fas配体可诱导活化的T细胞发生凋亡,从而实现肿瘤细胞的免疫逃逸[10]。 2.2.3 通过传递胞内蛋白调节靶细胞功能 内毒素刺激单核细胞后,通过释放包含caspase-1的微囊泡诱导血管平滑肌细胞死亡,这种细胞间诱导凋亡的实质便是微囊泡将caspase-1蛋白的功能直接作用于靶细胞上[11]。 2.2.4 介导遗传信息水平传递 共培养条件下,表观遗传变化这一现象时有报道,它发生的机制便可用遗传信息在细胞间发生转移及传递来解释。而且有研究显示,肿瘤细胞来源的微囊泡不仅可以传递表面决定簇,还可以将mRNA传递给单核细胞[12]。内皮祖细胞来源的微囊泡与内皮细胞表面的整合素发生作用,使mRNA在两者间往复传递,从而激活血管生成程序[13]。 2.3 微囊泡/外泌体参与的肺脏疾病 2.3.1 慢性阻塞性肺病 最近研究发现内皮微囊泡可作为肺气肿和慢性阻塞性肺病的致病效应物或预后指征[14],研究将受试者分为健康非吸烟者及吸烟者,其中吸烟者又分为肺功能、一氧化碳扩散量正常者和肺功能正常但一氧化碳扩散量低者。肺功能正常但一氧化碳扩散量低的吸烟者正处于肺气肿初期,此时发现这些吸烟者的内皮微囊泡水平明显升高,因此内皮微囊泡水平升高或许可视为早期肺气肿的标志。 另有研究发现在慢性阻塞性肺病恶化时,凋亡和激活的内皮微囊泡明显增加[15],进一步研究发现内皮微囊泡中CD62E+基线水平高,提示内皮细胞更易活化,换句话说,这样的慢性阻塞性肺病患者病情恶化的可能性增加。 Takahashi团队[15]指出CD31+和CD62E+的内皮细胞微囊泡即凋亡和活化的内皮细胞微囊泡水平升高可提示慢性阻塞性肺病恶化。未检测血管紧张素转化酶的表达,因为多数内皮细胞微囊泡不表达血管性血友病因子,在病情恶化时,无论是凋亡还是炎症/活化,肺毛细血管所受的影响最大,而且该研究还指出,CD62E+内皮微囊泡水平升高也预示患者有恶化的倾向,可作为预后的指征。该团队后期研究发现,CD62E+内皮细胞微囊泡水平的变化与第1秒用力呼气量呈明显负相关,提示内皮细胞持续激活和炎症将严重降低慢性阻塞性肺病患者的肺功能[16]。 因此,可以通过检测内皮细胞微囊泡分析肺脏内皮细胞的活化和凋亡,进而判断慢性阻塞性肺病病情变化,这也说明慢性阻塞性肺病是一种内皮成分变化引起的疾病,尤多见于肺脏与心血管的合并症[17]。近期提出了一个肺脏、内皮、骨髓和脂肪组织网络的整体模型,其中肺脏是外部传感器,内皮是内部传感器,骨髓和脂肪组织则是应答元件[18],将它们联系起来的介质很可能就是微囊泡。有研究曾发现脂肪组织分泌的瘦素[19]、空气污染物均可以诱导巨噬细胞和内皮细胞产生微囊泡[20]。 2.3.2 哮喘 哮喘通常呈现不同形式的气道炎症,涉及到一系列的细胞分子介质参与。近来一项研究显示,哮喘患者比健康者具有更多的血小板来源的微囊泡[21],提示血小板微囊泡在气道炎症中具有潜在的致病作用。有研究观察病毒感染在哮喘患者凝血平衡中的作用,结果显示鼻病毒感染后的哮喘患者肺泡灌洗液(BALF)中含有组织因子的微囊泡数量增加,携带组织因子的微囊泡可能会使感染了病毒的哮喘患者局部凝血功能亢进[22]。哮喘患者肺泡灌洗液中外泌体标志物水平升高,肺泡灌洗液外泌体可能通过升高气道上皮因子和白三烯的水平而引起炎症反应[23]。 白细胞介素13能够引起哮喘小鼠的上皮细胞外泌体分泌明显增多,这些上皮细胞来源的外泌体可以诱导未分化巨噬细胞的增殖,应用外泌体抑制剂GW4869后,可以减少增殖的单核细胞数目并有效减轻哮喘症状[24]。用卵清蛋白喂养的小鼠,其血清或血清来源的外泌体腹腔注射给未成年小鼠可以有效改善过敏体质[25]。上述研究说明,靶向外泌体或使用外泌体可作为预防和治疗哮喘的潜在方法。 2.3.3 弥漫性实质性肺病 目前对于弥漫性实质性肺病的病因及致病机制知之甚少,因此微囊泡在弥漫性实质性肺病中应用的研究很有限。以往研究曾观察到42例进行性硬化症患者的血小板微囊泡和单核细胞微囊泡水平高于健康对照者,尤其是硬化症患者中有间质性肺病的患者会检测出更高水平的血小板微囊泡和单核细胞微囊泡,提示微囊泡水平可作为间质性肺病发展的标志,选择治疗方案时可作为参考[26]。 凝血和肺纤维化关系密切[27],鉴于微囊泡在凝血过程中的作用,有研究观察微囊泡在肺纤维化患者体内的变化,19例患者的肺泡灌洗液中微囊泡的数量增加,且微囊泡携带的组织因子促凝活性较高[28],而且特发性肺纤维化患者的微囊泡组织因子活性比非特发性肺纤维化患者强;另外,特发性肺纤维化患者微囊泡组织因子含量与用力肺活量呈负相关;体外培养的肺泡上皮细胞在过氧化氢刺激下产生的促凝活性微囊泡增多。凝血因子Ⅹ的合成及转化为活化形式皆可发生在特发性肺纤维化过程中,因子Ⅹa除了可以将凝血酶原剪切成凝血酶,还可以剪切控制成纤维细胞向肌成纤维细胞分化的信号即剪切成纤维细胞上的蛋白酶激活受体1 (PAR-1),特发性肺纤维化局部凝血因子Ⅹ的合成及Ⅹa的表达都增加[29]。简单概括,即氧化应激诱导促凝反应,产生携带组织因子的微囊泡促进局部凝血因子Ⅹ的合成及Ⅹa的产生,因此也就间接促进蛋白酶激活受体1介导的肺纤维化的发生。 2.3.4 急性肺损伤/急性呼吸窘迫综合征(ALI/ARDS) 急性肺损伤时肺脏内会呈现一系列局部炎症,这与凝血级联反应活化及肺泡内纤维蛋白沉积密切相关。根据以往实验中观察到急性呼吸窘迫综合征会出现组织因子途径活化的迹象,BASTARACHE团队发现急性呼吸窘迫综合征患者肺内水肿液含有的微囊泡高于心源性水肿患者,而具有更高的促凝活性,这是因为急性呼吸窘迫综合征患者水肿液中组织因子浓度升高,恰与微囊泡增多的趋势一致,提示急性呼吸窘迫综合征患者水肿液中微囊泡里包含组织因子。进一步研究还发现死于急性呼吸窘迫综合征的患者比存活者肺泡上皮内的微囊泡多,推测微囊泡在激活血液凝固、促进肺泡内纤维蛋白沉积中起关键作用[30]。因此,急性呼吸窘迫综合征患者肺泡上皮来源的微囊泡数量可以作为患者预后的指标,并可能成为未来治疗急性呼吸窘迫综合征的潜在靶点。另一项研究分析52例急性呼吸窘迫综合征患者血浆和肺泡灌洗液中白细胞、中性粒细胞、内皮细胞和血小板中的微囊泡水平与对照组受试者之间的差异,结果显示,血浆中白细胞微囊泡水平高的呼吸窘迫综合征患者预后更好[31],循环水平的白细胞微囊泡与血小板、单核细胞微囊泡不同,白细胞微囊泡具有保护性,在败血症和感染性休克中可以保护血管张力[32]。近年发现,骨髓间充质干细胞外泌体可减轻内毒素诱导的小鼠急性肺损伤,将间充质干细胞分别进行缺氧处理0,30,60,90 min后,从培养上清中提取了外泌体随即应用于内毒素急性肺损伤小鼠模型中,其中缺氧60 min处理组急性肺损伤小鼠肺泡灌洗液中白细胞和中性粒细胞下降最显著;另外将缺氧60 min处理组的外泌体应用于内毒素刺激的RAW264.7细胞,能明显降低肿瘤坏死因子α水平,并升高白细胞介素10含量,提示间充质干细胞可通过外泌体减轻内毒素急性肺损伤[33]。另有研究报道,给予内毒素急性肺损伤小鼠气管注射人间充质干细胞来源的微囊泡48 h之后,可以通过改变受损肺泡KGF的表达而改善急性肺损伤的症状(减轻水肿,降低蛋白通透),减轻炎症(减少肺泡灌洗液中炎症细胞的浸润)[34]。杨尧等[35]观察尾静脉注射人脐带间充质干细胞外泌体对内毒素诱导大鼠急性肺损伤有治疗作用,发现经治疗后急性肺损伤大鼠血清促炎因子白细胞介素6、肿瘤坏死因子α和白细胞介素1β降低,抗炎因子白细胞介素10升高。 2.3.5 肺栓塞 促凝微囊泡在静脉血栓栓塞症(venous thromboembolism, VTE)中的作用现已受到广泛关注。研究发现静脉血栓栓塞症患者血浆内皮细胞微囊泡(EMPs)明显增加[36],提示在血块形成过程中存在内皮细胞微囊泡与白细胞的相互作用,因此内皮细胞微囊泡或许可作为预防治疗血栓事件的潜在靶点。 但也有不同观点,另一研究则发现急性肺栓塞患者的内皮细胞微囊泡和血小板微囊泡水平与对照组无差异[37],只有当对照组没有心血管事件发生风险时,循环水平的内皮细胞微囊泡和血小板微囊泡在静脉血栓栓塞症患者和对照组之间才存在差异,如果对照组受试者有心血管事件发生的风险时,则两组无差异。这一研究提示,循环水平的微囊泡只能作为心血管危险因素的标志。 近来的研究还显示,静脉血栓栓塞症患者总磷脂酰丝氨酸阳性的微囊泡循环水平高于对照组[38],而且微囊泡水平与静脉血栓栓塞症发生呈正相关。这是因为微囊泡的组成成分为促进血栓形成提供了生物活性物质,这也说明循环水平微囊泡可导致静脉血栓栓塞症发生。 上述研究都没有关注携带组织因子微囊泡在血块形成中的作用,而微囊泡中组织因子在其中的作用是不容忽视的。一项回顾性研究显示,肺栓塞疑似患者的携带组织因子微囊泡数量明显高于对照组,但其中的组织因子活性却没有大的差异[39]。肺栓塞患者如果患上癌症则其微囊泡组织因子的活性会增强,因此微囊泡组织因子活性并不是静脉血栓栓塞症事件的特征,而是癌症的表征。另一项前瞻性研究显示,深静脉血栓患者无论是否发生肺栓塞,呈现出一致的结论[40],即微囊泡组织因子活性并不是血栓形成的根源。 静脉血栓栓塞症与癌症的关系目前已很明确[41],对于静脉血栓栓塞症癌转移患者,微囊泡组织因子的活性高于单纯的癌症患者、健康者及特发性静脉血栓栓塞症患者,提示肿瘤衍生的微囊泡可能启动了癌症患者体内的血块形成级联反应从而致病[42]。类似的研究也明确指出,微囊泡组织因子活性与癌症有关,在静脉血栓栓塞症发生时过度活跃[43-45]。上述发现提示这些微囊泡源于肿瘤细胞,在静脉血栓栓塞症发展过程中起致病作用,或可作为潜在的生物标记,以用于肿瘤患者选择理想的预防治疗方案。在一项Ⅱ期随机试验中,选择66例不可手术患者为观察对象,其中微囊泡组织因子活性高的患者分别给予预防剂量的依诺肝素及安慰剂,2个月后发现,经过依诺肝素治疗的患者静脉血栓栓塞症发生率降低(与低水平的微囊泡组织因子活性的发生率类似)[46],说明微囊泡组织因子活性可以作为静脉血栓栓塞症发生风险的预测标志,并作为癌症患者抗凝治疗的靶点选择。 2.3.6 肺癌 早些年研究中发现,肺癌患者的血小板微囊泡和单核细胞微囊泡数量多于健康者,且癌症患者血小板活化标志物表达也增加,提示微囊泡与血管并发症存在密切关联[47]。微囊泡还可作为肺癌患者的预后指标,循环总微囊泡在非小细胞肺癌患者体内升高,如果原来微囊泡基线水平高,则预后较好[48];也有研究通过107例非小细胞肺癌患者的血小板微囊泡和内皮细胞微囊泡的测定,揭示相关的预后结果[49]。循环外泌体中的microRNA可作为肺癌的诊断标志[50-51],尿液来源外泌体LRG-1的表达也可作为诊断非小细胞肺癌的颇具前景的手段[52]。外泌体在细胞间扮演通讯员的角色,可在肿瘤微环境中执行促进癌细胞生长、刺激血管新生、活化基质成纤维细胞、抑制机体免疫反应等诸多功能。顺铂可使A549细胞的外泌体分泌增强,将此外泌体加入A549细胞,可降低其对顺铂的敏感性,这一过程可能是细胞间通过外泌体内miRNA和mRNA信息传递而实现的[53]。A549细胞可以摄取人结直肠癌细胞的外泌体,从而使外泌体内的生物活性物质得以传递和共享[54]。 血小板来源的微囊泡可以促进A549细胞增殖并增加促血管生成基因的表达,小鼠静脉注射其血小板来源的微囊泡后会明显增强迁移性,提示血小板微囊泡在肿瘤生长、迁移和血管生成中起重要作用[55]。来源于人肾癌干细胞的微囊泡应用于肺癌小鼠模型中,发现可促进肺癌转移前微环境和血管生成[56]。贫血小板血浆中的组织因子阳性微囊泡预示肺癌向远处转移[57]。 2.3.7 肺动脉高压 对于肺动脉高压患者,微囊泡可作为病理诊断依据及预后指标。20例肺动脉高压患者的内皮细胞微囊泡及内含的组织因子活性高于健康者,且越是病情严重的患者内皮微囊泡数量及所含组织因子的活性就越高[58]。低氧可通过肺内巨噬细胞的替代激活使促炎介质释放而引起肺内炎症反应,最终导致低氧性肺高压,常用作肺动脉高压动物模型。来源于小鼠间充质干细胞培养基中的外泌体能抑制低氧性肺高压过程中巨噬细胞的浸润、促炎和促增殖介质的产生。静脉给予间充质干细胞的外泌体可抑制血管重塑,如果耗竭间充质干细胞外泌体或成纤维细胞来源外泌体则会失去上述功能。而且,间充质干细胞外泌体可以抑制低氧活化信号转导及STAT3的激活,以低氧诱导的人肺动脉上皮细胞为研究对象,来源于人脐带间充质干细胞的外泌体便可抑制细胞模型中的STAT3信号[59]。王英宏等[60]发现大鼠骨髓间充质干细胞外泌体可降低肺动脉高压大鼠平均肺动脉压和右心室压,对野百合碱诱导的肺动脉高压有治疗作用。 综上所述,微囊泡可作为呼吸系统气道炎症性疾病的主要致病因素、诊断依据或治疗靶点,具体详见表1[14-15,21,26,28,30-31,42-44,46-49,58,61-68]。 2.4 存在的问题和局限 近年来,微囊泡/外泌体的作用在肺病研究中虽然取得了一定的进展,但在应用前尚有亟待解决的问题:使微囊泡/外泌体合成并分泌的有效刺激需要探究加以明确;目前应用间充质干细胞外泌体作为治疗手段的基础实验初见成效,但间充质干细胞外泌体因不同器官来源而特性各异,在进行大规模临床前试验时则受限于来源器官,而且外泌体的治疗剂量及培养来源细胞的反应容器规格仍需确定;外泌体的作用机制仍不清楚,其中哪类活性物质作用于疾病过程中的哪个靶细胞有待研究。 目前很多研究提示微囊泡/外泌体内的miRNA对于肺病诊断、预防和治疗尤为重要,但在研究中却存在着诸多问题和困难:①筛查分析miRNA,可以很容易发现发病过程中很多miRNA的表达皆发生变化,但具体哪个miRNA才是罪魁祸首,目前缺少确立关键miRNA的金标准;②体液和外泌体miRNA目前尚没有标准的提取分离方法;③目前正常的组织和体液样本采集miRNA的质量控制标准还有待完善;④关于miRNA的信息量很大,明确它们的网络关系,将用于诊断和治疗的miRNA进行分类应用还有待于深入研究。"
| [1] Wolf P. The nature and significance of platelet products in human plasma. Br J Haematol. 1967;13(3):269-288.[2] Pugholm LH, Revenfeld AL, Søndergaard EK, et al. Antibody-Based Assays for Phenotyping of Extracellular Vesicles. Biomed Res Int. 2015;2015:524817.[3] Biancone L, Bruno S, Deregibus MC, et al. Therapeutic potential of mesenchymal stem cell-derived microvesicles. Nephrol Dial Transplant. 2012;27(8):3037-3042.[4] Ratajczak J, Wysoczynski M, Hayek F, et al. Membrane-derived microvesicles: important and underappreciated mediators of cell-to-cell communication. Leukemia. 2006;20(9):1487-1495.[5] Zwaal RF, Comfurius P, Bevers EM. Scott syndrome, a bleeding disorder caused by defective scrambling of membrane phospholipids. Biochim Biophys Acta. 2004;1636 (2-3):119-128.[6] Cocucci E, Racchetti G, Meldolesi J. Shedding microvesicles: artefacts no more. Trends Cell Biol. 2009;19(2):43-51.[7] Polgar J, Matuskova J, Wagner DD. The P-selectin, tissue factor, coagulation triad. J Thromb Haemost. 2005;3(8): 1590-1596.[8] Barry OP, Praticò D, Savani RC, et al. Modulation of monocyte-endothelial cell interactions by platelet microparticles. J Clin Invest. 1998;102(1):136-144.[9] Janowska-Wieczorek A, Majka M, Kijowski J, et al. Platelet-derived microparticles bind to hematopoietic stem/progenitor cells and enhance their engraftment. Blood. 2001;98(10):3143-3149.[10] Kim JW, Wieckowski E, Taylor DD, et al. Fas ligand-positive membranous vesicles isolated from sera of patients with oral cancer induce apoptosis of activated T lymphocytes. Clin Cancer Res. 2005;11(3):1010-1020.[11] Sarkar A, Mitra S, Mehta S, et al. Monocyte derived microvesicles deliver a cell death message via encapsulated caspase-1. PLoS One. 2009;4(9):e7140.[12] Baj-Krzyworzeka M, Szatanek R, Weglarczyk K, et al. Tumour-derived microvesicles carry several surface determinants and mRNA of tumour cells and transfer some of these determinants to monocytes. Cancer Immunol Immunother. 2006;55(7):808-818.[13] Deregibus MC, Cantaluppi V, Calogero R, et al. Endothelial progenitor cell derived microvesicles activate an angiogenic program in endothelial cells by a horizontal transfer of mRNA. Blood. 2007;110(7):2440-2448.[14] Gordon C, Gudi K, Krause A, et al. Circulating endothelial microparticles as a measure of early lung destruction in cigarette smokers. Am J Respir Crit Care Med. 2011;184(2): 224-232.[15] Takahashi T, Kobayashi S, Fujino N, et al. Increased circulating endothelial microparticles in COPD patients: a potential biomarker for COPD exacerbation susceptibility. Thorax. 2012;67(12):1067-1074.[16] Takahashi T, Kobayashi S, Fujino N, et al. Annual FEV1 changes and numbers of circulating endothelial microparticles in patients with COPD: a prospective study. BMJ Open. 2014;4(3):e004571.[17] Barberà JA. Chronic obstructive pulmonary disease: a disease of the endothelium. Am J Respir Crit Care Med. 2013;188(1):5-7.[18] Agustí A, Barberà JA, Wouters EF, et al. Lungs, bone marrow, and adipose tissue. A network approach to the pathobiology of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;188(12):1396-1406.[19] Petrini S, Neri T, Lombardi S, et al. Leptin induces the generation of procoagulant, tissue factor bearing microparticles by human peripheral blood mononuclear cells. Biochim Biophys Acta. 2016;1860(6):1354-1361.[20] Neri T, Pergoli L, Petrini S, et al. Particulate matter induces prothrombotic microparticle shedding by human mononuclear and endothelial cells. Toxicol In Vitro. 2016;32:333-338.[21] Duarte D, Taveira-Gomes T, Sokhatska O, et al. Increased circulating platelet microparticles as a potential biomarker in asthma. Allergy. 2013;68(8):1073-1075.[22] Majoor CJ, van de Pol MA, Kamphuisen PW, et al. Evaluation of coagulation activation after rhinovirus infection in patients with asthma and healthy control subjects: an observational study. Respir Res. 2014;15:14.[23] Torregrosa Paredes P, Esser J, Admyre C, et al. Bronchoalveolar lavage fluid exosomes contribute to cytokine and leukotriene production in allergic asthma. Allergy. 2012; 67(7):911-919.[24] Kulshreshtha A, Ahmad T, Agrawal A, et al. Proinflammatory role of epithelial cell-derived exosomes in allergic airway inflammation. J Allergy Clin Immunol. 2013;131(4):1194-1203.[25] Almqvist N, Lönnqvist A, Hultkrantz S, et al. Serum-derived exosomes from antigen-fed mice prevent allergic sensitization in a model of allergic asthma. Immunology. 2008;125(1):21-27.[26] Nomura S, Inami N, Ozaki Y, et al. Significance of microparticles in progressive systemic sclerosis with interstitial pneumonia. Platelets. 2008;19(3):192-198.[27] Crooks MG, Hart SP. Coagulation and anticoagulation in idiopathic pulmonary fibrosis. Eur Respir Rev. 2015; 24(137):392-399.[28] Novelli F, Neri T, Tavanti L, et al. Procoagulant, tissue factor-bearing microparticles in bronchoalveolar lavage of interstitial lung disease patients: an observational study. PLoS One. 2014;9(4):e95013.[29] Scotton CJ, Krupiczojc MA, Königshoff M, et al. Increased local expression of coagulation factor X contributes to the fibrotic response in human and murine lung injury. J Clin Invest. 2009;119(9):2550-2563.[30] Bastarache JA, Fremont RD, Kropski JA, et al. Procoagulant alveolar microparticles in the lungs of patients with acute respiratory distress syndrome. Am J Physiol Lung Cell Mol Physiol. 2009;297(6):L1035-1041.[31] Guervilly C, Lacroix R, Forel JM, et al. High levels of circulating leukocyte microparticles are associated with better outcome in acute respiratory distress syndrome. Crit Care. 2011;15(1):R31.[32] Mostefai HA, Meziani F, Mastronardi ML, et al. Circulating microparticles from patients with septic shock exert protective role in vascular function. Am J Respir Crit Care Med. 2008;178(11):1148-1155.[33] Li L, Jin S, Zhang Y. Ischemic preconditioning potentiates the protective effect of mesenchymal stem cells on endotoxin-induced acute lung injury in mice through secretion of exosome. Int J Clin Exp Med. 2015;8(3):3825-3832.[34] Zhu YG, Feng XM, Abbott J, et al. Human mesenchymal stem cell microvesicles for treatment of Escherichia coli endotoxin-induced acute lung injury in mice. Stem Cells. 2014;32(1):116-125.[35] 杨尧,朱耀斌,李志强,等.间充质干细胞外泌体对大鼠急性肺损伤的保护作用[J]. 中华实用诊断与治疗杂志,2017,31(7): 628-631.[36] Chirinos JA, Heresi GA, Velasquez H, et al. Elevation of endothelial microparticles, platelets, and leukocyte activation in patients with venous thromboembolism. J Am Coll Cardiol. 2005;45(9):1467-1471.[37] Bal L, Ederhy S, Di Angelantonio E, et al. Factors influencing the level of circulating procoagulant microparticles in acute pulmonary embolism. Arch Cardiovasc Dis. 2010;103(6-7):394-403.[38] Bucciarelli P, Martinelli I, Artoni A, et al. Circulating microparticles and risk of venous thromboembolism. Thromb Res. 2012;129(5):591-597.[39] Garcia Rodriguez P, Eikenboom HC, Tesselaar ME, et al. Plasma levels of microparticle-associated tissue factor activity in patients with clinically suspected pulmonary embolism. Thromb Res. 2010;126(4):345-349.[40] Thaler J, Koppensteiner R, Pabinger I, et al. Microparticle-associated tissue factor activity in patients with acute unprovoked deep vein thrombosis and during the course of one year. Thromb Res. 2014;134(5): 1093-1096.[41] Connolly GC, Francis CW. Cancer-associated thrombosis. Hematology Am Soc Hematol Educ Program. 2013;2013: 684-691.[42] Tesselaar ME, Romijn FP, Van Der Linden IK, et al. Microparticle-associated tissue factor activity: a link between cancer and thrombosis. J Thromb Haemost. 2007; 5(3):520-527.[43] Campello E, Spiezia L, Radu CM, et al. Endothelial, platelet, and tissue factor-bearing microparticles in cancer patients with and without venous thromboembolism. Thromb Res. 2011;127(5):473-477.[44] Manly DA, Wang J, Glover SL, et al. Increased microparticle tissue factor activity in cancer patients with Venous Thromboembolism. Thromb Res. 2010;125(6): 511-512.[45] Zwicker JI, Liebman HA, Neuberg D, et al. Tumor-derived tissue factor-bearing microparticles are associated with venous thromboembolic events in malignancy. Clin Cancer Res. 2009;15(22):6830-6840.[46] Zwicker JI, Liebman HA, Bauer KA, et al. Prediction and prevention of thromboembolic events with enoxaparin in cancer patients with elevated tissue factor-bearing microparticles: a randomized-controlled phase II trial (the Microtec study). Br J Haematol. 2013;160(4):530-537.[47] Kanazawa S, Nomura S, Kuwana M, et al. Monocyte-derived microparticles may be a sign of vascular complication in patients with lung cancer. Lung Cancer. 2003;39(2):145-149.[48] Fleitas T, Martínez-Sales V, Vila V, et al. Circulating endothelial cells and microparticles as prognostic markers in advanced non-small cell lung cancer. PLoS One. 2012; 7(10):e47365.[49] Wang CC, Tseng CC, Hsiao CC, et al. Circulating endothelial-derived activated microparticle: a useful biomarker for predicting one-year mortality in patients with advanced non-small cell lung cancer. Biomed Res Int. 2014;2014:173401.[50] Cazzoli R, Buttitta F, Di Nicola M, et al. microRNAs derived from circulating exosomes as noninvasive biomarkers for screening and diagnosing lung cancer. J Thorac Oncol. 2013;8(9):1156-1162.[51] Rosell R, Wei J, Taron M. Circulating MicroRNA Signatures of Tumor-Derived Exosomes for Early Diagnosis of Non-Small-Cell Lung Cancer. Clin Lung Cancer. 2009;10(1): 8-9.[52] Arscott WT, Camphausen KA. Analysis of urinary exosomes to identify new markers of non-small-cell lung cancer. Biomark Med. 2011;5(6):822.[53] Xiao X, Yu S, Li S, et al. Exosomes: decreased sensitivity of lung cancer A549 cells to cisplatin. PLoS One. 2014; 9(2):e89534.[54] Chiba M, Kimura M, Asari S. Exosomes secreted from human colorectal cancer cell lines contain mRNAs, microRNAs and natural antisense RNAs, that can transfer into the human hepatoma HepG2 and lung cancer A549 cell lines. Oncol Rep. 2012;28(5):1551-1558.[55] Janowska-Wieczorek A, Wysoczynski M, Kijowski J, et al. Microvesicles derived from activated platelets induce metastasis and angiogenesis in lung cancer. Int J Cancer. 2005;113(5):752-760.[56] Grange C, Tapparo M, Collino F, et al. Microvesicles released from human renal cancer stem cells stimulate angiogenesis and formation of lung premetastatic niche. Cancer Res. 2011;71(15):5346-5356.[57] Tseng JC, Chang LC, Jiang BY, et al. Elevated circulating levels of tissue factor-positive microvesicles are associated with distant metastasis in lung cancer. J Cancer Res Clin Oncol. 2014;140(1):61-67.[58] Bakouboula B, Morel O, Faure A, et al. Procoagulant membrane microparticles correlate with the severity of pulmonary arterial hypertension. Am J Respir Crit Care Med. 2008;177(5):536-543.[59] Lee C, Mitsialis SA, Aslam M, et al. Exosomes mediate the cytoprotective action of mesenchymal stromal cells on hypoxia-induced pulmonary hypertension. Circulation. 2012;126(22):2601-2611.[60] 王英宏,刘珍君,肖梦媛,等. 间充质干细胞源性外泌体对肺动脉高压大鼠的疗效观察[J]. 广东医科大学学报, 2017,35(5): 462-468.[61] Thomashow MA, Shimbo D, Parikh MA, et al. Endothelial microparticles in mild chronic obstructive pulmonary disease and emphysema. The Multi-Ethnic Study of Atherosclerosis Chronic Obstructive Pulmonary Disease study. Am J Respir Crit Care Med. 2013;188(1):60-68.[62] Takahashi T, Kobayashi S, Fujino N, et al. Annual FEV1 changes and numbers of circulating endothelial microparticles in patients with COPD: a prospective study. BMJ Open. 2014;4(3):e004571.[63] Majoor CJ, van de Pol MA, Kamphuisen PW, et al. Evaluation of coagulation activation after rhinovirus infection in patients with asthma and healthy control subjects: an observational study. Respir Res. 2014;15:14.[64] Zwicker JI, Liebman HA, Neuberg D, et al. Tumor-derived tissue factor-bearing microparticles are associated with venous thromboembolic events in malignancy. Clin Cancer Res. 2009;15(22):6830-6840.[65] Tseng CC, Wang CC, Chang HC, et al. Levels of circulating microparticles in lung cancer patients and possible prognostic value. Dis Markers. 2013;35(5):301-310.[66] Bakouboula B, Morel O, Faure A, et al. Procoagulant membrane microparticles correlate with the severity of pulmonary arterial hypertension. Am J Respir Crit Care Med. 2008;177(5):536-543.[67] Amabile N, Heiss C, Real WM, et al. Circulating endothelial microparticle levels predict hemodynamic severity of pulmonary hypertension. Am J Respir Crit Care Med. 2008; 177(11):1268-1275.[68] Amabile N, Heiss C, Chang V, et al. Increased CD62e(+) endothelial microparticle levels predict poor outcome in pulmonary hypertension patients. J Heart Lung Transplant. 2009;28(10):1081-1086. |
| [1] | Pu Rui, Chen Ziyang, Yuan Lingyan. Characteristics and effects of exosomes from different cell sources in cardioprotection [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-. |
| [2] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [3] | Zhang Chao, Lü Xin. Heterotopic ossification after acetabular fracture fixation: risk factors, prevention and treatment progress [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1434-1439. |
| [4] | Zhou Jihui, Li Xinzhi, Zhou You, Huang Wei, Chen Wenyao. Multiple problems in the selection of implants for patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1440-1445. |
| [5] | Wang Debin, Bi Zhenggang. Related problems in anatomy mechanics, injury characteristics, fixed repair and three-dimensional technology application for olecranon fracture-dislocations [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1446-1451. |
| [6] | Ji Zhixiang, Lan Changgong. Polymorphism of urate transporter in gout and its correlation with gout treatment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1290-1298. |
| [7] | Yuan Mei, Zhang Xinxin, Guo Yisha, Bi Xia. Diagnostic potential of circulating microRNA in vascular cognitive impairment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1299-1304. |
| [8] | Wang Xianyao, Guan Yalin, Liu Zhongshan. Strategies for improving the therapeutic efficacy of mesenchymal stem cells in the treatment of nonhealing wounds [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1081-1087. |
| [9] | Wan Ran, Shi Xu, Liu Jingsong, Wang Yansong. Research progress in the treatment of spinal cord injury with mesenchymal stem cell secretome [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1088-1095. |
| [10] | Liao Chengcheng, An Jiaxing, Tan Zhangxue, Wang Qian, Liu Jianguo. Therapeutic target and application prospects of oral squamous cell carcinoma stem cells [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1096-1103. |
| [11] | Zhao Min, Feng Liuxiang, Chen Yao, Gu Xia, Wang Pingyi, Li Yimei, Li Wenhua. Exosomes as a disease marker under hypoxic conditions [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1104-1108. |
| [12] | Xie Wenjia, Xia Tianjiao, Zhou Qingyun, Liu Yujia, Gu Xiaoping. Role of microglia-mediated neuronal injury in neurodegenerative diseases [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1109-1115. |
| [13] | Li Shanshan, Guo Xiaoxiao, You Ran, Yang Xiufen, Zhao Lu, Chen Xi, Wang Yanling. Photoreceptor cell replacement therapy for retinal degeneration diseases [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1116-1121. |
| [14] | Jiao Hui, Zhang Yining, Song Yuqing, Lin Yu, Wang Xiuli. Advances in research and application of breast cancer organoids [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1122-1128. |
| [15] | Wang Shiqi, Zhang Jinsheng. Effects of Chinese medicine on proliferation, differentiation and aging of bone marrow mesenchymal stem cells regulating ischemia-hypoxia microenvironment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1129-1134. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||