Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (19): 3097-3102.doi: 10.3969/j.issn.2095-4344.0259
Previous Articles Next Articles
Current status of postoperative quality of life in patients with tibial plateau fracture
Yuan Liang1, Lü Yang2, Zhou Fang2
- 1Peking University International Hospital, Beijing 102206, China; 2Peking University Third Hospital, Beijing 100191, China
-
Online:2018-07-08Published:2018-07-08 -
Contact:Zhou Fang, M.D., Chief physician, Professor, Peking University Third Hospital, Beijing 100191, China -
About author:Yuan Liang, M.D., Physician, Peking University International Hospital, Beijing 102206, China -
Supported by:the National Natural Science Foundation of China (General Program), No. 51473004
CLC Number:
Cite this article
Yuan Liang, Lü Yang, Zhou Fang. Current status of postoperative quality of life in patients with tibial plateau fracture[J]. Chinese Journal of Tissue Engineering Research, 2018, 22(19): 3097-3102.
share this article
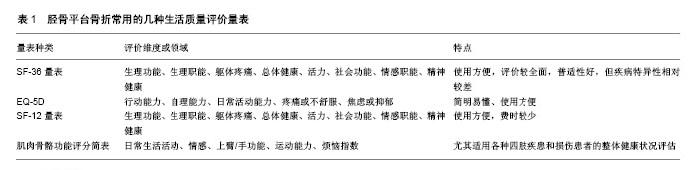
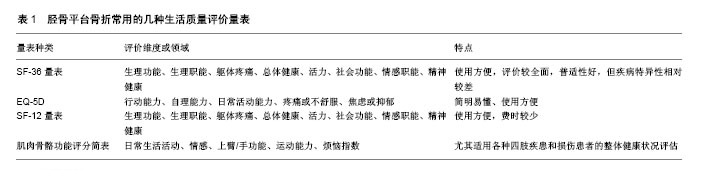
2.1 健康相关生活质量研究的发展简史 20世纪70年代末,社会学领域中“生活质量”的概念被引入到医学研究中,来探究疾病以及和疾病相关的因素对人生存状态的影响,从而使健康相关生活质量(Health Related Quality of Life, HRQoL)的研究得以兴起[3-4],健康相关生活质量逐渐成为评价健康状态的新手段。健康相关生活质量是在一定的文化背景和价值理念中,测定在疾病、意外、伤害以及医疗干预的条件下与个人生活事件相联系的主观健康状态和个体满意程度[5-7]。健康相关生活质量的评价内容包含了生理、心理、社会生活等方面的内容,全面地对一个人整体生活质量进行了考察,不仅关心患者的客观生理功能,同时还强调主观感受,不仅关注患者生存时间,同时还重视生活质量的高低。因而对患者健康相关生活质量的研究巧妙地弥补了传统评价方法无法全面评价健康结局的不足[8]。 目前随着健康相关生活质量研究在医疗领域的兴起,越来越多的骨科医师将健康相关生活质量视为骨科手术后疗效评估的重要内容[9-13]。健康生活质量研究在骨科领域成为一个方兴未艾的研究方向。在骨科领域研究健康相关生活质量的文献中,通常也将健康相关生活质量直接简称为“生活质量”。 2.2 生活质量评价工具 2.2.1 常用的生活质量评价工具 目前常用的生活质量评价工具有The MOS 36-item short-form health survey(SF-36量表)[14]、EuroQol(EQ-5D)及Short Form-12 Health Survey (SF-12量表)[15-16],其他的还有如肌肉骨骼功能评分简表(SMFA)、世界卫生组织生存质量测定量表(WHOQOL-100)、世界卫生组织生存质量测定简表(WHOQOL-BREF)、良好状态量表(QWB)、诺丁汉健康调查表(NHP)等等[17]。在这些工具中,SF-36量表是应用最多的一种。检索PubMed数据库得到自1988年以来98篇涉及胫骨平台骨折患者生活质量评价的文献,其中90%以上都是应用SF-36量表作为评价工具。 2.2.2 用于胫骨平台骨折的评价工具 对于胫骨平台骨折,以上几种生活质量评价工具,一般认为都能使用,SF-36量表应用最多,其次还有SF-12量表、EuroQol(EQ-5D)以及SMFA,见表1,但针对胫骨平台骨折这一特定的疾病,其评价准确性是否都能满足临床需要,还需要系统研究。 SF-12量表是在SF-36量表的基础上简化而来,和SF-36量表相比,SF-12量表简化了问卷所含的条目,可以有效缩短生活质量调查时间,对于大多数患者可在不需要帮助的情况下3 min之内完成问卷的填写。虽然经过了简化,但SF-12量表评价的维度与SF-36量表一致,也包括8个维度和2个综合测量,具体见后文。 EuroQol(EQ-5D)中文名称为欧洲五维健康量表,其最大的优势是简明易懂、使用方便。EuroQol(EQ-5D)主要从行动能力(Mobility)、自理能力(Self-care)、日常活动能力(Usual activities)、疼痛或不舒服(Pain/ Discomfort)、焦虑或抑郁(Anxiety/Depression)等5个维度对生活质量进行综合评价。此量表包括问卷和效用值换算表两个部分,通过问卷调查能够描述被测试者的健康状态和生活质量状况,然后用效用值换算表可以将问卷的结果换算成EQ-5D指数得分,从而进行量化分析。 SMFA比较适用于运动系统尤其是各种四肢疾患和损伤患者的整体健康状况评估。此量表包括了功能评价的34个条目和由于功能障碍所导致烦恼评价的12个条目。其中,功能评价的条目又被分成了问题出现的严重程度及频度两大类。根据各条目中问题性质的区别可分为以下5个领域,包括:①日常生活活动;②情感;③上臂/手功能;④运动能力;⑤烦恼指数。在实际应用过程当中,可对受试者的每一个领域分别进行评分。SMFA在不影响评价系统敏感性的情况下,简化了调查研究的过程,既可以用于治疗效果的评价,也能够适用于患者健康状况和生活质量的评价,而且均可靠、有效。 Dattani等[11]对SF-36量表、SMFA以及西大略湖和麦克马斯特大学骨关节炎量表(the Western Ontario McMaster Osteoarthritis Questionnaires,WOMAC)进行了对比分析,认为在胫骨平台骨折患者中用SF-36量表可能会更好。 2.2.3 SF-36量表 SF-36量表是20世纪80年代末美国波士顿健康研究所在美国医疗结果调查问卷的基础上研制的生活质量调查量表,被广泛用于普通人群生活质量监测、卫生政策评价、临床研究等[14, 18-21],并且在20世纪90年代初被遴选为国际生活质量评价项目的测评工具[18, 22]。SF-36量表包括2个大类即生理健康、心理健康,从8个不同的维度进行评价[14],包括生理功能、生理职能、躯体疼痛、总体健康、活力、社会功能、情感职能及精神健康,每个维度包括不同的条目,一共包含36个条目。目前SF-36量表已被翻译成多个语言版本,海峡两岸暨香港的学者分别进行了翻译汉化研究工 作[23-30],在国内广泛使用的中文版本是由浙江大学公共卫生教研室翻译研制的[28-29]。 SF-36评分的高低能够直接反映患者健康状况和生活质量的好坏,得分高说明健康状况和生活质量好,得分低说明健康状况和生活质量差。各维度的得分结果可以与常模进行比较,解释不同评分值的临床意义。SF-36可由受试者自行填写完成,或者通过电话随访、面对面随访完成该量表所有内容的测试。SF-36测试过程中,以下几个问题需要特别注意:①要注意不同条目的评定时间并不完全一致,有些条目是过去4周,有些条目则是过去1年;②调查员在回收调查问卷时要逐条核实,受试者是否回答了所有问题,如未回答全部问题,要注意询问理由;③要让受试者充分理解反向评分条目的含义,并正确填写问卷,防止填错;④对于不能够完全理解SF-36量表测试内容的受试者,不宜将其作为测试对象;⑤调查员不能给予受试者提示性的诱导。"
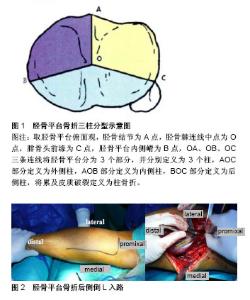
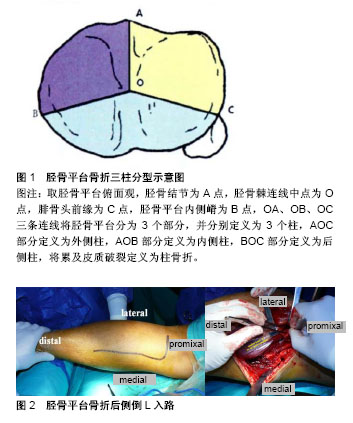
2.3 胫骨平台骨折手术治疗后患者生活质量 胫骨平台作为膝关节最重要的组成部分,骨折以后将直接影响膝关节功能,使患者活动明显受限,对患者日常生活、工作和学习造成严重影响,可能对患者的心理也会带来不同程度的打击。传统的评价工具对骨折复位程度、膝关节功能进行评价固然能够对手术效果做出很高的评价,反过来进一步指导对不同的骨折采取不同的手术策略,但他们共同的缺点是难以反映出这类外伤对患者心理和精神层面的影响。而对患者术后生活质量的测量恰恰能弥补这一不足,能更全面地反映治疗效果的优劣,更有利于加深对胫骨平台骨折治疗的认识。 2.3.1 高能量损伤的复杂胫骨平台骨折 目前针对胫骨平台骨折患者手术后生活质量的研究,大部分集中在高能量损伤的复杂胫骨平台骨折,这可能与这类骨折对患者生活影响更大有关系。 (1)外固定架治疗的高能量损伤的复杂胫骨平台骨折:早在1995年,Marsh等[31]学者在研究用外固定加有限内固定的方法治疗复杂胫骨平台骨折时,就将患者术后的生活质量作为重要的评价指标,并用SF-36量表进行评分,进行了平均38个月的随访,发现用该方法治疗的复杂胫骨平台骨折患者,康复以后生活质量评分与匹配的相应年龄组人群差别不大。认为这种方法治疗复杂胫骨平台骨折是可行的、满意的。 2002年Weigel等[32]也对一组高能量损伤的胫骨平台骨折行外固定架固定加有限内固定治疗的患者进行研究,平均随访长达98个月,发现这一组患者术后生活质量并没有比匹配的正常年龄组有明显降低,同时与自身相比较术后生活质量评分并没有比术前有明显下降。这与Marsh等[31]学者所得到结果类似。随后2003年Ali等[33]报道了一组60岁以上用Sheffield外固定器固定联合经皮螺钉内固定治疗的胫骨平台双髁骨折(OTA-41C2和OTA-41C3型)病例研究结果,仍然用SF-36量表进行生活质量评估,平均随访38个月,发现这一组患者生理功能、活力以及精神健康3个维度得分比相应年龄组正常人群要低,但是只有精神健康得分和相应年龄组正常人群相比差异有显著性意义,其他几个维度的得分差异均无显著性意义。 然而到了2005年Chin等[34]报告了明显不同的结果,他们对一组平均年龄43.8(27-68)岁的高能量损伤复杂胫骨平台患者应用环形外固定架(Tensioned Fine-wire Fixation)治疗,平均随访28个月,结果提示除了精神健康这一维度以外,SF-36量表其他维度的得分都较正常人群要明显降低,但由于此项研究中病例数量较少,仅有18例患者完成了SF-36量表评估,因此结论的可靠性还有待验证。 (2)外固定架与切开复位内固定治疗效果对比:2006年澳大利亚创伤骨科学会发布了一项多中心前瞻性随机对照研究结果[35],这项研究对标准的切开复位内固定、环形外固定架外固定联合有限内固定两种策略治疗胫骨平台双髁骨折(Schatzker Ⅴ、Ⅵ型)的疗效进行了对比,2组患者平均年龄分别为43.3岁和46.2岁,用SF-36量表评价患者的生活质量,发现在受伤后2年2组患者的SF-36量表所有维度的得分都比各自的对照组明显降低,而将这2组患者进行对比,则发现躯体疼痛评分在环形外固定架治疗组受影响更小,其他各维度得分在这2组患者中差异均无显著性意义。 此后的诸多关于高能量损伤胫骨平台骨折(或胫骨平台双髁骨折)的研究[36-39],多数也都得出了与澳大利亚创伤骨科学会的这项多中心前瞻性随机对照研究相似的结论,认为高能量损伤胫骨平台骨折患者治疗后生活质量可能会比同年龄段正常人群的生活质量明显降低。其中,Ahearn等[36]对55例不稳定胫骨平台双髁骨折患者采用切开复位锁定钢板内固定或者环形外固定架固定联合有限切开内固定治疗,用SF-36量表评估患者生活质量,发现这两种方法治疗的患者生活质量都较正常人有明显下降。只有El-Sayed等[37]报道的对高能量损伤的胫骨平台内外侧平台骨折用有限切开内固定加Ilizarov外固定架治疗后随访结果显示,患者生活质量与相应年龄组正常人群相差并不大。甚至有研究认为,不管是高能量损伤还是低能量损伤的胫骨平台骨折,手术后患者生活质量都会比正常人明显降低[38-40]。 2.3.2 不同年龄段胫骨平台骨折患者生活质量 对不同年龄段的人群,也有学者进行了研究。Frenyo等[41]对一组超过70岁的老年胫骨平台骨折患者进行分析,认为对于这个年龄段的患者采用闭合复位、微创固定能使患者获得更好的功能和生活质量。Stevens等[42]学者对47例移位的胫骨平台骨折进行切开复位内固定的患者进行了5年以上的随访,按年龄分组对患者生活质量进行评价和分析。发现40岁以下的患者,无论是何种骨折类型,其生活质量的各项评分,包括各个维度以及综合测量,与相应的正常人群无明显差异。但在40岁以上的患者中,有33%低能量损伤和55%高能量损伤的胫骨平台骨折患者术后生活质量较正常人明显降低。 2.3.3 新理念、新策略指导下的治疗 其他的学者也从不同的角度对胫骨平台骨折患者手术后生活质量进行了评价。罗从风等[43]学者在提出胫骨平台骨折三柱分型时用SF-36量表对患者术后生活质量进行了评估(图1),研究结果显示按照三柱分型制定手术策略,患者术后能获得较满意的生活质量。项小霞[44]研究了早期康复训练对胫骨平台骨折手术患者生活质量的影响,随访结果显示在医护人员的指导和监督下,早期进行康复锻炼的患者最终能获得更好的生活质量。Garner等[45]对胫骨平台骨折愈合后拆除内植物是否能让患者获益进行了研究,重点关注了膝关节功能和生活质量,发现拆除内植物后,患者生活质量会有所提升,但膝关节疼痛并不一定能得到有效缓解。Ollivier等[46]对胫骨平台骨折球囊扩张成形术进行了研究,认为对有压缩的外侧平台骨折采用球囊扩张复位、可吸收磷酸钙骨水泥填充是安全有效的,但从生活质量角度来看,患者生活质量评分并不令人满意。Qiu等[47]对倒“L”入路治疗胫骨平台骨折疗效研究时也采用了SF-36量表评价患者生活质量(图2),结果显示这种手术入路治疗的患者术后生活质量评分比较好。Cui等[48]评价了关节镜辅助闭合复位或微创复位固定的手术疗效,随访结果显示关节镜辅助手术组术后生活质量比常规手术组要高,但没有与相应年龄组的正常人群进行比较,也没有报告骨折分型情况以及不同分型之间的比较分析。Elsøe等[49]报告了AO 41-B2、B3型胫骨平台骨折采用经皮螺钉固定的疗效分析,用EQ-5D评价生活质量,平均随访2.5年,提示采用这种方法治疗的AO 41-B2、B3型胫骨平台骨折患者术后生活质量并没有比正常人群降低。"
| [1] Kokkalis ZT, Iliopoulos ID, Pantazis C, et al. What's new in the management of complex tibial plateau fractures? Injury. 2016;47(6): 1162-1169.[2] 顾立强. 胫骨平台骨折的分类与功能评价[J]. 中华创伤骨科杂志, 2004, 6(3): 323-327.[3] Hays RD, Anderson R, Revicki D. Psychometric considerations in evaluating health-related quality of life measures. Qual Life Res.1993; 2(6): 441-449.[4] Cox DR, Jones DR. Quality-of-Life Assessment: Can We Keep It Simple? J Royal Statist Soc.1992;155(3): 353-393.[5] Cella DF, Cherin EA. Quality of life during and after cancer treatment. Comprehens Ther. 1988;14(5): 69-75.[6] Schipper H. Guidelines and caveats for quality of life measurement in clinical practice. Oncology.1990;4(5): 51-57; discussion 70.[7] Orley J, Kuyken W. The Development of the World-Health-Organization Quality-of-Life Assessment Instrument - Preliminary Data. Qual Life Res. 1994;3(1): 53-54.[8] Ellwood PM. Shattuck lecture--outcomes management. A technology of patient experience. N Engl J Med. 1988;318(23):1549-1556.[9] 周非非,孙宇,党耕町. 颈椎病外科治疗效果评价方法的进展[J]. 中国脊柱脊髓杂志,2008,18(1): 70-73.[10] 周非非,孙宇,王少波,等. 颈椎病外科治疗结果评价体系的探讨[J]. 中国脊柱脊髓杂志, 2008,18(1):55-59.[11] Dattani R, Slobogean GP, O’Brien PJ, et al. Psychometric analysis of measuring functional outcomes in tibial plateau fractures using the Short Form 36 (SF-36), Short Musculoskeletal Function Assessment (SMFA) and the Western Ontario McMaster Osteoarthritis (WOMAC) questionnaires. Injury. 2013;44(6): 825-829.[12] Dehghan N, McKee MD, Jenkinson RJ, et al. Early weightbearing and range of motion versus non-weightbearing and immobilization after open reduction and internal fixation of unstable ankle fractures: a randomized controlled trial. J Orthop Trauma. 2016;30(7): 345-352.[13] Honkavaara N, Al-Ani AN, Campenfeldt P, et al. Good responsiveness with EuroQol 5-Dimension questionnaire and Short Form (36) Health Survey in 20-69 years old patients with a femoral neck fracture: A 2-year prospective follow-up study in 182 patients. Injury. 2016;47(8): 1692-1697.[14] Ware JE, Snow KK, Mark K, et al. SF-36 Health Survey: Manual and Interpretation Guide. Boston: New England Medical Center, The Health Institute, 1993.[15] Group E. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy (Amsterdam, Netherlands).1990;16(3): 199-208.[16] Lam CL, Tse EY, Gandek B. Is the standard SF-12 health survey valid and equivalent for a Chinese population?. Qual Life Res. 2005;14(2): 539-547.[17] 张世民. 骨折分类与功能评定[M]. 北京: 人民军医出版社, 2008.[18] Aaronson NK, Acquadro C, Alonso J, et al. International Quality of Life Assessment (IQOLA) Project. Qual Life Res.1992;1(5): 349-351.[19] Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med Care. 1992;30(6): 473-483.[20] McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993; 31(3): 247-263.[21] McHorney CA, Ware JE Jr, Lu JF, et al. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care.1994;32(1): 40-66.[22] Gandek B, Ware JE Jr. Methods for validating and norming translations of health status questionnaires: the IQOLA Project approach. International Quality of Life Assessment. J Clin Epidemiol. 1998; 51(11): 953-959.[23] Lam CL, Gandek B, Ren XS, et al. Tests of scaling assumptions and construct validity of the Chinese (HK) version of the SF-36 Health Survey. J Clin Epidemiol. 1998;51(11): 1139-1147.[24] Lam C, Lauder I, Lam T, et al. Population based norming of the Chinese (HK) version of the SF-36 Health Survey. Hong Kong Pract. 1999;21(10): 460-470.[25] Lu JFR, Tseng HM, Tsai YJ. Assessment of Health-related Quality of Life in Taiwan (I): Development and Psychometric Testing of SF-36 Taiwan Version. Taiwan J Public Health. 2003;22(6): 501-511.[26] Tseng HM, Lu JFR, Tsai YJ. Assessment of Health Related Quality of Life (II): Norming and Validation of SF-36 Taiwan Version. Taiwan J Public Health. 2003;22(6): 512-518.[27] 方积乾,万崇华,史明丽,等. 生存质量研究概况与测定量表[J]. 现代康复,2000,4(8):1123-1126,1133.[28] 李鲁,王红妹,沈毅,等. SF-36健康调查量表中文版的研制及其性能测试[J]. 中华预防医学杂志, 2002,36(2): 38-42.[29] Li L, Wang HM, Shen Y. Chinese SF-36 Health Survey: translation, cultural adaptation, validation, and normalisation. J Epidemiol Community Health. 2003;57(4):259-263.[30] 刘朝杰,李宁秀,任晓晖,等. 36条目简明量表在中国人群中的适用性研究[J]. 四川大学学报医学版, 2001,32(1):39-42.[31] Marsh JL, Smith ST, Do TT. External fixation and limited internal fixation for complex fractures of the tibial plateau. J Bone Joint Surg. 1995;77(5): 661-673.[32] Weigel DP, Marsh JL. High-energy fractures of the tibial plateau. Knee function after longer follow-up. J Bone Joint Surg Am. 2002; 84-A(9): 1541-1551.[33] Ali AM, Burton M, Hashmi M, et al. Treatment of displaced bicondylar tibial plateau fractures (OTA-41C2&3) in patient older than 60 years of age. J Orthop Trauma. 2003;17(5):346-352.[34] Chin TY, Bardana D, Bailey M, et al. Functional outcome of tibial plateau fractures treated with the fine-wire fixator. Injury. 2005;36(12): 1467-1475.[35] Society COT. Open reduction and internal fixation compared with circular fixator application for bicondylar tibial plateau fractures. Results of a multicenter, prospective, randomized clinical trial. J Bone Joint Surg Am. 2006;88(12): 2613-2623.[36] Ahearn N, Oppy A, Halliday R, et al. The outcome following fixation of bicondylar tibial plateau fractures. Bone Joint J. 2014;96B(7): 956-962.[37] El-Sayed MMH, Khanfour AA. Management of high-energy bicondylar tibial plateau fractures by minimal internal fixation and the ilizarov frame: The knee function. Eur Orthop Traumatol. 2014;5 (2): 109-114.[38] Timmers TK, van der Ven DJ, de Vries LS, et al. Functional outcome after tibial plateau fracture osteosynthesis: a mean follow-up of 6 years. Knee. 2014;21(6): 1210-1215.[39] Warschawski Y, Elbaz A, Segal G, et al. Gait characteristics and quality of life perception of patients following tibial plateau fracture. Arch Orthop Trauma Surg. 2015;135(11): 1541-1546.[40] Ebrahimzadeh MH, Birjandinejad A, Moradi A, et al. Clinical instability of the knee and functional differences following tibial plateau fractures versus distal femoral fractures. Trauma Mon. 2015;20(1): 20-25.[41] Frenyo S, Kecskemeti A, Szita J, et al. Operative management of fractures of the tibial plateau in old/very old patients. Acta Chirurgica Austriaca. 2000; 32(SUPPL161): 42-43.[42] Stevens DG, Beharry R, McKee MD, et al. The long-term functional outcome of operatively treated tibial plateau fractures. J Orthop Trauma. 2001;15(5): 312-320.[43] 罗从风,胡承方,高洪,等 基于CT的胫骨平台骨折的三柱分型[J]. 中华创伤骨科杂志,2009, 11(3): 201-205.[44] 项小霞. 早期康复训练对胫骨平台骨折膝关节功能恢复和生活质量的影响[J]. 国际护理学杂志, 2012,31(7):1248-1249.[45] Garner MR, Thacher RR, Ni A, et al. Elective removal of implants after open reduction and internal fixation of Tibial Plateau fractures improves clinical outcomes. Arch Orthop Trauma Surg. 2015;135 (11): 1491-1496.[46] Ollivier M, Turati M, Munier M, et al. Balloon tibioplasty for reduction of depressed tibial plateau fractures: Preliminary radiographic and clinical results. Int Orthop. 2016;40(9): 1961-1966.[47] Qiu WJ, Zhan Y, Sun H, et al. A posterior reversed L-shaped approach for the tibial plateau fractures - A prospective study of complications (95 cases). Injury. 2015;46(8): 1613-1618.[48] Cui Y, Wang W, Huang T, et al. Impact of arthroscopic percutaneous poking reduction-fixation on affected limb function and quality of life of patients with fracture of Tibial plateau. Int J Clin Exp Med.2016;9(6): 12115-12119.[49] Elsøe R, Larsen P, Rasmussen S, et al. High degree of patient satisfaction after percutaneous treatment of lateral tibia plateau fractures. Dan Med J. 2016;63(1):A5174. [50] McNamara IR, Smith TO, Shepherd KL, et al. Surgical fixation methods for tibial plateau fractures. Cochrane Database Syst Rev. 2015;(9):CD009679.[51] 袁亮,吕扬,周方,等. 胫骨平台骨折手术疗效三种评价体系相关性研究[J]. 中华创伤骨科杂志,2017,19(4):349-352.17:18 2018-7-16 |
| [1] | Pu Rui, Chen Ziyang, Yuan Lingyan. Characteristics and effects of exosomes from different cell sources in cardioprotection [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-. |
| [2] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [3] | Wang Haiying, Lü Bing, Li Hui, Wang Shunyi. Posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis: prediction of functional prognosis of patients based on spinopelvic parameters [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1393-1397. |
| [4] | Zhang Chao, Lü Xin. Heterotopic ossification after acetabular fracture fixation: risk factors, prevention and treatment progress [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1434-1439. |
| [5] | Zhou Jihui, Li Xinzhi, Zhou You, Huang Wei, Chen Wenyao. Multiple problems in the selection of implants for patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1440-1445. |
| [6] | Wang Debin, Bi Zhenggang. Related problems in anatomy mechanics, injury characteristics, fixed repair and three-dimensional technology application for olecranon fracture-dislocations [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1446-1451. |
| [7] | Ji Zhixiang, Lan Changgong. Polymorphism of urate transporter in gout and its correlation with gout treatment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1290-1298. |
| [8] | Yuan Mei, Zhang Xinxin, Guo Yisha, Bi Xia. Diagnostic potential of circulating microRNA in vascular cognitive impairment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1299-1304. |
| [9] | Wang Xianyao, Guan Yalin, Liu Zhongshan. Strategies for improving the therapeutic efficacy of mesenchymal stem cells in the treatment of nonhealing wounds [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1081-1087. |
| [10] | Wan Ran, Shi Xu, Liu Jingsong, Wang Yansong. Research progress in the treatment of spinal cord injury with mesenchymal stem cell secretome [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1088-1095. |
| [11] | Liao Chengcheng, An Jiaxing, Tan Zhangxue, Wang Qian, Liu Jianguo. Therapeutic target and application prospects of oral squamous cell carcinoma stem cells [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1096-1103. |
| [12] | Zhao Min, Feng Liuxiang, Chen Yao, Gu Xia, Wang Pingyi, Li Yimei, Li Wenhua. Exosomes as a disease marker under hypoxic conditions [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1104-1108. |
| [13] | Xie Wenjia, Xia Tianjiao, Zhou Qingyun, Liu Yujia, Gu Xiaoping. Role of microglia-mediated neuronal injury in neurodegenerative diseases [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1109-1115. |
| [14] | Li Shanshan, Guo Xiaoxiao, You Ran, Yang Xiufen, Zhao Lu, Chen Xi, Wang Yanling. Photoreceptor cell replacement therapy for retinal degeneration diseases [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1116-1121. |
| [15] | Jiao Hui, Zhang Yining, Song Yuqing, Lin Yu, Wang Xiuli. Advances in research and application of breast cancer organoids [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1122-1128. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||