Chinese Journal of Tissue Engineering Research ›› 2023, Vol. 27 ›› Issue (16): 2580-2586.doi: 10.12307/2023.172
Previous Articles Next Articles
Selection and biological characteristics of repair materials for skull base reconstruction
Huai Peng1, Zhang Yipeng2, Wang Xi1, Wang Wei1, Wang Liang1, Chen Lei1
- 1Department of Neurosurgery, Tianjin Fifth Central Hospital, Tianjin 300450, China; 2Department of Pathology, PKUCare CNOOC Hospital, Tianjin 300452, China
-
Received:2022-03-16Accepted:2022-06-18Online:2023-06-08Published:2022-11-11 -
Contact:Chen Lei, MD, Chief physician, Department of Neurosurgery, Tianjin Fifth Central Hospital, Tianjin 300450, China -
About author:Huai Peng, Master, Department of Neurosurgery, Tianjin Fifth Central Hospital, Tianjin 300450, China
CLC Number:
Cite this article
Huai Peng, Zhang Yipeng, Wang Xi, Wang Wei, Wang Liang, Chen Lei. Selection and biological characteristics of repair materials for skull base reconstruction[J]. Chinese Journal of Tissue Engineering Research, 2023, 27(16): 2580-2586.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
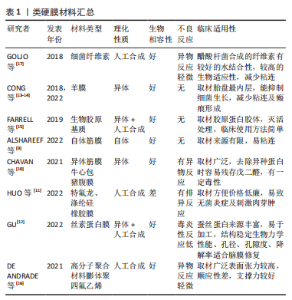
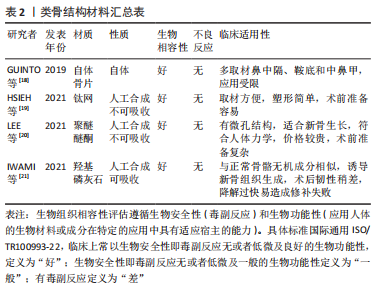
2.1 颅底修补材料研究概述 随着近年来颅底修补材料的改进及新型材料的研发,神经内镜下术后颅底修补的多重重建临床经验的总结,类似颅底生理解剖的硬膜-骨质-黏膜的重建方式更符合人体的生理结构,也有助于硬膜、骨质、黏膜的再生。颅底生物材料的发展也是基于此逐步更迭,因此临床上也大量衍生了许多类硬膜、类骨质的生物材料用作颅底修补的多重重建[9-21],在临床应用的适应证上、和人体的生物相容性方面诸多生物材料有着自己的优缺点,见表1,2。"

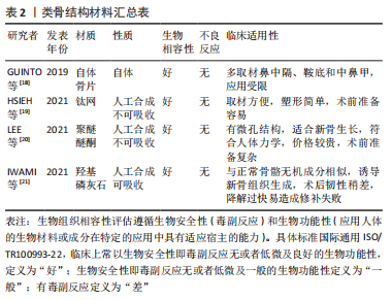
"
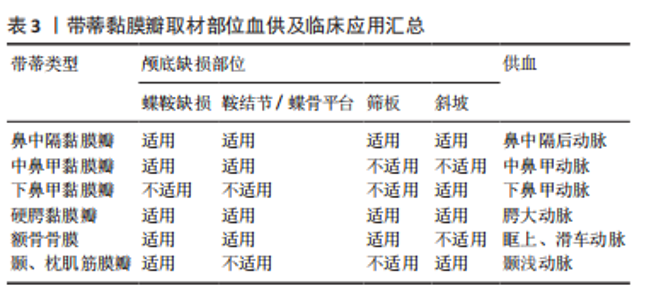
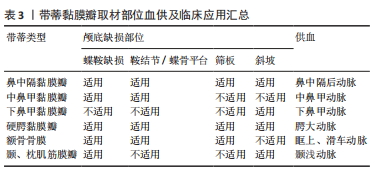
2.2 颅底重建原则 大部分学者认为重建的基本原则是针对低流量脑脊液漏应用脂肪、筋膜、人工脑膜及医用胶等进行多层颅底重建[22-24],对高流量脑脊液漏应用带蒂鼻中隔黏膜瓣的多层颅底重建技术修补。颅底重建的目的是把开放性的漏口变闭合,多层复合重建,提供暂时凭障,为组织再生提供支撑就是在颅内外结构之间建立可靠的屏障,避免脑脊液漏及颅内感染,同时颅底重建还包括闭塞肿瘤切除后遗留的死腔,避免积液和感染。大部分学者提出3N原则,即开放变闭合(NO water)、各层不能有间隙(NO gaps)、材料平整、清除黏膜和骨嵴(NO encumbrance),而颅底重建的关键点是缺损部分瘢痕化,这也是颅底重建修补成功的标志[25-27]。 2.3 颅底重建方法 2.3.1 一般修复 硬膜/蛛网膜完整,术中无脑脊液漏,修补以人工硬膜为主。有研究发现如果术者术中未发现脑脊液漏或无蛛网膜损伤,则仅在瘤腔内充填明胶海绵,骨性鞍底使用组织粘合胶重建鞍底,甚至不需要填塞[28-29]。 2.3.2 游离材料多层复合重建 如硬膜/蛛网膜缺损< 1 cm,低流量脑脊液漏,颅底重建选择脂肪、肌肉及筋膜为主,即先取大腿外侧或腹部适量皮下脂肪、肌肉(肌肉要尽可能捣成糊状)、筋膜及人工硬膜,自脑脊液漏口发生处由脂肪、肌肉浆、人工硬膜、肌筋膜逐层填满,由内向外,最外层以适量生物蛋白胶加固,最后碘仿纱条支撑。 脂肪组织不亲水,遇到脑脊液后因其脂性缘故可在表面形成张力,防止脑脊液渗漏,而且有柔软平滑、质地均匀的特点,填塞修补更加方便。有研究应用脂肪组织修补脑脊液漏口,作为颅底修补的第一层取得良好的效果,脂肪组织不仅仅能够起到物理填塞的作用,可以阻止脑脊液的渗漏,还验证了脂肪组织能促进和硬脑膜缺损的融合的作用[30-31]。 有研究报道了运用密封垫片技术进行颅底重建[32-34],即浴缸塞原理,其研究认为该技术不仅能为颅底缺损提供有效持久的支撑,同时还能减少脑脊液聚集。到目前为止,随着该技术的应用,临床上也证实了其在脑脊液漏相应颅底修补中的可靠性,现在应用密封垫片技术治疗脑脊液漏和颅底缺损成为神经外科医师普遍共识。 2.3.3 带蒂黏膜瓣修复 硬膜或蛛网膜缺损>1 cm,与脑池或脑室相通的高流量脑脊液漏,目前大部分学者提倡多层修补[29,35],先用自体脂肪填塞蛛网膜漏口,应用速即纱包裹捣碎的肌肉糜填塞,人工硬脑膜贴附于硬膜下,阔筋膜平铺于鞍底硬脑膜外,生物蛋白胶封闭起部分支撑作用,最后用带蒂鼻中隔黏膜瓣为主(带蒂中、下鼻甲黏膜瓣等)覆盖,带蒂其血供源于蝶腭动脉的鼻中隔支黏膜瓣往往延展性较好,根据颅底缺损需要可修剪成不同的大小和形状,而且最突出的优点是修补后的带蒂黏膜瓣因为带有血供,会与颅底蝶窦黏膜生长为一体,达到修补效果最大化,带蒂黏膜瓣边缘要求与鞍底紧密贴附,不留空隙,有助黏膜生长。蝶窦和鼻腔碘仿纱条填塞支撑。 鼻中隔黏膜的面积不小,但在颅底缺损较大,加上蝶窦气化较为明显时,鼻中隔黏膜瓣的取材就不仅局限于鼻中隔,即可以向鼻腔底,甚或下鼻甲,可以获得比较大的鼻中隔黏膜瓣面积。有研究应用CT扫描进行黏膜瓣术前设计,提供了一个非常好的简单设计手段[36-37]。在CT工作站里手术前CT扫描上,首先测量黏膜瓣贴覆颅底的最大径线长度,然后根据CT扫描的冠状位和矢状位,计算出获得最大径线鼻中隔黏膜瓣的取材部位。其中,比较重要的是鼻中隔最前缘到蝶窦前下的直线距离,其次是冠状位上显示可以获得的鼻中隔黏膜瓣上下最大距离,即宽度;并与蝶窦上下径和周径比较,判断黏膜瓣是否满足颅底修复之用。如果鼻中隔黏膜上下径(即宽度)不能覆盖颅底缺损,可以向鼻腔底甚至下鼻甲外侧面延伸,获得更宽黏膜瓣。他们在实验和临床应用中发现,如果取整个鼻中隔黏膜,即从鼻中隔最前缘到后缘,其长度可以适用于几乎所有的患者。设计和制做黏膜瓣时,注意防止黏膜瓣干燥挛缩。黏膜瓣周边多取6 mm;为保留嗅觉功能,嗅区黏膜需保留部分,黏膜瓣后上距颅底要留出距离筛顶约10 mm宽度黏膜。制作好的黏膜瓣可一直放在鼻咽部,用纱条覆盖保护直到颅底切除手术过程结束。手术中注意要小心处理骨质向翼管侧的移动,确保不损伤供血血管即蝶腭动脉。鞍区手术切除过程完成后,清理鞍区,包括蝶窦内衬黏膜,然后将留置在鼻咽部的黏膜瓣翻转到鞍区,覆盖于鞍底缺损区。取出蝶窦黏膜,是为了保证黏膜瓣能够与骨面充分接触,便于黏膜瓣贴覆颅底,这也是手术成功的重要前提条件[38-39]。 带蒂鼻中隔黏膜瓣的多层颅底重建技术虽然取得良好的效果,但是它的应用也有局限性,例如无法先切除病变后取黏膜瓣,尤其是比较大的病变切除,多数情况下切除病变不一定会出现脑脊液漏,但是一旦术中出现高流量脑脊液漏,除非提前已制备黏膜瓣,否则可能由于黏膜瓣供血动脉破坏或者操作过程中鼻腔黏膜损伤而造成无瓣可取。常规制备黏膜瓣,往往会造成术中无脑脊液漏患者术后鼻腔黏膜的不必要损伤。因此有学者提出对于这种情况,可以采用改良补救鼻中隔黏膜瓣,可以先切除病变后取黏膜瓣[40-41],具体操作:先行蝶窦开口上缘沿鼻中隔黏膜瓣上横切口,保留黏膜瓣蒂部血管,鼻中隔后部黏膜放置于下鼻道及后鼻孔,在不影响术中操作空间的情况下,手术过程中可始终保留黏膜瓣的蒂部,切除病变后如出现脑脊液漏则转为制作完整的黏膜瓣,如无脑脊液漏则直接将其复位。 2.3.4 蝶窦鞍底黏膜骨瓣 有学者提出黏膜骨瓣的应用,多应用于无脑脊液漏或低流量脑脊液漏[42]。在暴露鞍底黏膜后,辨识鞍底结构,骨性标志,常采用“C”形切开鞍底黏膜,按术前规划黏膜下磨钻成形鞍底骨瓣,最后将游离好的骨瓣向底边翻转,并将黏膜及骨瓣尽量向下推,形成半游离的黏膜骨瓣。其主要优点:尽可能保持鞍底正常生理结构,操作相对简单,蝶窦鞍底黏膜骨瓣翻转复位成功后,能为术后颅底重建提供材料及力学支撑,理论上又可达到解剖学复位从而有助术后黏膜恢复。其局限性是更蝶窦气化正相关,气化良好的蝶窦是此种术式的解剖学基础,气化良好的蝶窦还为术中黏膜骨瓣成形和翻转等操作提供足够空间。 2.3.5 硬膜缝合 鉴于缝合通道狭长,缝合过程比较复杂困难,需要特殊器械,目前多以间断缝合为主,硬膜-硬膜间、硬膜-筋膜/人工硬膜间缝合,大部分不能做到水密缝合,但是可以变开放为闭合,并且提供支撑。期待有更好的器械改进,如果将来能做到水密缝合,那么颅底重建将不再是经鼻神经内镜手术的难题。 2.4 修补材料分类及生物学特性 2.4.1 软组织修补材料 自体软组织修补材料:脂肪、肌肉、筋膜、带蒂或游离组织瓣、骨膜。脂肪组织斥水,人工硬膜贴敷性好,肌肉、筋膜支撑性好、组织相容性好、不易被吸收,肌肉粘连性好、不易吸收。 人工软组织修补材料:①不可吸收:涤纶橡胶膜等人工硬膜;组织相容性差;②可吸收:③胶原人工硬膜、异体真皮无细胞基质等,组织相容性较好,但是支撑力较差。 2.4.2 骨性修补材料 自体骨片材料:源自术中鼻中隔、中鼻甲、鞍底的游离骨片,均取自自体,但是受生理结构限制,临床应用局限性较大。 人工骨性修补材料: (1)不可吸收人工骨性修补材料:钛网、多孔聚乙烯(Polyethylene,PE),聚醚醚酮(Polyetheretherketone,PEEK)等,其中PEEK材料,因为其诸多优点用作医学上人骨的替代材料有逐步取代钛合金材料的趋势。其优点概括起来包括以下几点:耐高温、自润滑、易加工、高机械强度、低溶出性、可耐反复高压灭菌、与人体组织相融性好。 有研究尝试在神经内镜经鼻蝶手术术后应用PEEK材料修补颅底骨质缺损,这种修补方式类似于临床常见的凸面的颅骨缺损修补[43-44],但是相对于其他颅骨修补材料,PEEK材料修补更可靠,与人体组织的组织相容性更好,临床应用中很少出现排斥反应,同时因为PEEK材料为人工合成的聚醚醚酮,自身有微孔结构,这种微孔结构有助于新生骨组织长入,从而与自身骨组织更好地结合。因为PEEK材料类似于人体骨骼的韧性及变形性具有更相似人体骨骼的力学性能,例如在人体受力时,PEEK材料因为其高机械强度为人体提供高强度支撑力及保护的同时,又可以与人体骨骼一样,对受到的外力做出相应的微变形,并且在外力消失后恢复原有的形状。避免了不能做出微变形以适应外力作用,在人体受到外力作用时一旦超出其可承受范围,可能造成变形或直接损坏,对人体造成二次伤害。另外,PEEK材料可根据术中需要在术前加工成所需的任意大小和形状,达到较大程度契合不规则的缺损,再辅以生物胶粘合边缘,可达到较为满意的水密密封程度,满足颅底缺损修补尤其是术中发生脑脊液漏修补的需求。PEEK材料作为修补材料其缺点也比较明显,目前其费用高昂,对于颅底修补,术前准备也比较复杂。 (2)可吸收人工骨性修补材料:羟基磷灰石、聚乳酸、聚内消旋乳酸、聚二恶烷酮等,组织相容性较好,中间孔隙有利骨组织生长,但是韧性稍差。 2.4.3 常用人工硬膜比较 临床内镜术后颅底重建的重中之重是封闭颅内外沟通,在颅内外间建立可靠的密闭屏障,避免脑脊液漏从而从根源上预防颅内感染,颅底重建的重点之一就是硬膜修补。因此,这就要求硬膜修补材料要能发挥类似人脑硬膜的生物学功能,又要有组织相容性和良好的力学支撑,这也是近年对硬膜修补替代材料研究的重点方向。 人工合成的材料分为人工合成聚合物和自然聚合物。人工合成聚合物包括聚乙二醇水凝胶、聚乳酸和聚己内酯等,其优点是力学性能更好,并且最后可以降解成无毒性的小分子,但是人工合成聚合物也有可能造成局部组织反应、瘢痕过度增生以及出血一系列的缺陷;自然聚合物包括:胶原蛋白、明胶、纤维蛋白原等。自然聚合物相对来说其力学性能差,不能单独使用,因其支撑力有限单独使用容易造成脑脊液漏,有的虽然其生物相容性好,但是其降解又往往不可控。 有研究通过电纺丝方法制造的原理,发明了胶原蛋白纳米纤维材料作为颅底多层修补的替代材料,其基本分为3层,最内层选择聚乳酸,中间层应用聚乳酸-聚己内酯复合材料,最外层是胶原蛋白[45-46],其优点是:最内层的聚乳酸接触脑组织层减少了与脑组织的黏附,降低了炎症的发生,中间层应用的聚乳酸-聚己内酯复合材料,起到防水作用,有效降低脑脊液漏的发生率,最外层使用胶原蛋白,能加强细胞间黏附,促进细胞增殖。自此基础上有生物科技公司研发了主要成分为聚左旋乳酸纤维的中空、互相连接的3D结构材料。这种材料人体细胞可生长进入并且逐步形成组织,最后这种材料逐渐被机体吸收,而且它还有较强的组织相容性,能较少与脑组织黏附。研究发现其纤维的植入呈现出3D网状结构,并且与人体自身硬膜组织的胞外基质环境极为相似,在其植入后的不同阶段,浸润的免疫细胞少、免疫反应低,并且与脑组织无粘连,同时与传统修补材料相比,其力学性能更好,研究证明了该材料在颅底重建运用中的组 织相容性、易塑形性与促进硬膜快速重生的能力[47-48]。 异种生物膜材料:牛、猪、羊心包;猪小肠黏膜;猪胸、腹膜等。优点:抗原性显著降低,光滑、柔软易于裁剪缝合。缺点:戊二醛处理,去除异种蛋白同时,少量醛基可致无菌性炎症,降解速度慢,阻挡新生组织生长。只能缝合使用。 脱细胞真皮基质:牛、猪脱细胞基质。优点:天然胶原空间网状结构,利于纤维细胞附着和增殖,促进血管化的进程,缺点:猪真皮基质上分布小孔,致密性低于戊二醛处理材料。使用时可缝可粘。 提取胶原:牛肌腱(胶原海绵)、马跟腱(胶原基质胶体)。优点:黏合力强,缺点:力学性能差,容易发生破损,降解快。只能黏合使用。 2.4.4 形状记忆合金支架-薄膜瓣复合体 有研究将形状记忆合金支架-薄膜瓣复合体补片安装在硬性通条前端,转换硬性通条前后部为垂直状态、合拢手柄、使补片纳入硬性通道前端之杯状扩大内近端并固定,在硬性通道的引导下预置于颅底缺损区,张开手柄,补片依靠形状记忆合金支架的超弹性等自身特性和上下两个半环状挡片的机械推动作用、脱出硬性通道前端杯状扩大部,恢复硬性通条前后部的直线状态、使球形扩大之指状突起缩回,补片解脱于目标位置、封闭颅底缺损区,同时完成颅底骨性与膜性重建[49-50]。 2.4.5 封闭剂 生物蛋白胶(纤维蛋白黏合剂):①品牌:护固莱士、倍绣、安可欣、天绣、丰联、创恤封、悦灵胶、安可胶;②成分:纤维蛋白、凝血酶;③来源:哺乳动物血液;④特点:组织相容性好,完全降解,医用,水密性差;⑤功能:止血、密封、防粘 连、促愈合、缓释剂。 医用化学胶(耳脑胶):①品牌:白云、康派特等;②来源:化学合成;③成分:α-氰基丙烯酸酯等;④特点:组织相容性好,不降解,局部硬结,水密性差;⑤功能:黏合性好,止血。 2.4.6 带蒂组织瓣 带蒂黏膜瓣血供源于蝶腭动脉的鼻中隔支黏膜瓣往往延展性较好,根据颅底缺损需要可修剪成不同的大小和形状,其优点是修补后的带蒂黏膜瓣因为带有血供,会与颅底蝶窦黏膜生长为一体,达到修补效果最大化,带蒂黏膜瓣边缘要求与鞍底紧密贴附,不留空隙,有助黏膜生长,见表3。"
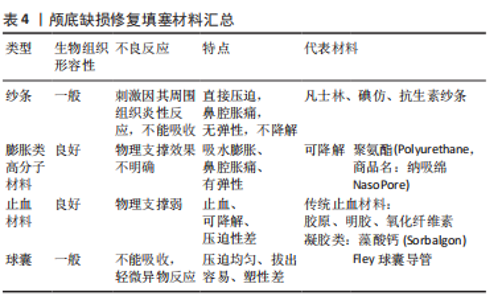
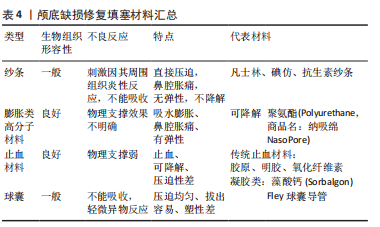
2.4.7 填塞材料 临床上,目前多以疏水组织+人工硬膜完成颅底缺损修复,修补支撑力不强,术后颅压波动脑脊液漏的风险较大,为弥补支撑力不足,临床医生通常应用填塞材料加强支撑,见表4。"
| [1] CAI X, YANG J, ZHU J, et al. Reconstruction strategies for intraoperative CSF leak in endoscopic endonasal skull base surgery: systematic review and meta-analysis. Br J Neurosurg, 2021. doi: 10.1080/02688697.2020.1849548. [2] AHN S, PARK J, KIM D, et al. Surgical experience in prevention of postoperative csf leaks using abdominal fat grafts in endoscopic endonasal transsphenoidal surgery for pituitary adenomas. J Neurol Surg B Skull Base. 2021;82(5):522-527. [3] ALBONETTE-FELICIO T, MARTINEZ-PEREZ R, VANKOEVERING K, et al. Soft gasket seal reconstruction after endoscopic endonasal transtuberculum resection of craniopharyngiomas. World Neurosurg. 2021. doi: 10.1016/j.wneu.2021.12.058. [4] BOWEN A, ELTAHIR A, GOATES A, et al. The posterior septal nasal floor mucosal flap for cranial base reconstruction. Laryngoscope. 2022. doi: 10.1002/lary.30079. [5] CERAUDO M, CAVALLO L, ROSSI D, et al. Role of anterior nasal packing in endoscopic skull base surgery: Italian survey. World Neurosurg. 2021;154:e406-e415. [6] ALOKBY G, ALAMARI K, ABDULLAH J, et al. Endoscopic reconstruction of skull base defects using tutoplast. Allergy Rhinol. 2021. doi: 10.1177/21526567211009200. [7] BAUSSART B, RACY E, GAILLARD S. Double pedicled nasoseptal flap for skull base repair after endoscopic expanded endonasal approach. Acta Neurochir. 2022;164(4):1111-1114. [8] CHASKES M, RABINOWITZ M. Safety of restarting continuous positive airway pressure (CPAP) therapy following endoscopic endonasal skull base surgery. World J Otorhinolaryngol Head Neck Surg. 2022;8(1):61-65. [9] ALSHAREEF M, ALROQI A, ALBAHARNA H, et al. Nasoseptal flap and rigid reconstruction in endoscopic endonasal skull base surgeries: the longitudinal experience of a single center. Ear Nose Throat J. 2022.doi:10.1177/01455613221099483. [10] CHAVAN S, POTDUKHE K, KALE V, et al. A comparitive study of endoscopic skull base reconstruction in CSF rhinorrea using nasoseptal flap with septal cartilage v/s fascia lata with fat. Indian J Otolaryngol Head Neck Surg. 2021;73(2):233-239. [11] HUO C, KING J, GOLDSCHLAGER T, et al. The effects of cerebrospinal fluid (CSF) diversion on post-operative CSF leak following extended endoscopic anterior skull base surgery. J Clin Neurosci. 2022;98:194-202. [12] GU D. Radioanatomical study of the skull base and septum in chinese:implications for using the HBF for endoscopic skull base reconstruction. Oxid Med Cell Longev. 2022. doi:10.1155/2022/9940239. [13] CONG Z, LIU K, WEN G, et al. Universal sellar anatomical reconstruction using the sellar floor flap after endoscopic pituitary adenoma surgery. Otolaryngol Head Neck Surg. 2018;158(4):774-776. [14] DUAN H, JIANG X, LI C, et al. Application of a three-dimensional printed model to localize a cranial cerebrospinal fluid leak: a case report. J Int Med Res. 2022;50(2):3000605221078412. [15] FARRELL N, KINGDOM T, GETZ A, et al. Development of chronic sphenoid sinusitis after sellar reconstruction with medpor porous polyethylene implant. World Neurosurg. 2019;123:e781-e786. [16] DE ANDRADE E, ALMEIDA J, BORGHEI-RAZAVI H, et al. Reconstruction after extended endonasal approaches to the anterior cranial base: surgical techniques and current results. J Neurosurg Sci. 2021;65(2): 151-159. [17] GOLJO E, KINBERG E, STEPAN K, et al. Reconstruction of a skull base defect after endoscopic endonasal resection of a pituitary adenoma: Sphenoid mucosal flaps. Am J Otolaryngol. 2018;39(2):253-256. [18] GUINTO G, NETTEL B, HERNáNDEZ E, et al. Osseous remodeling technique of the sella turcica:a new surgical option for primary empty sella syndrome. World Neurosurg. 2019;126:e953-e958. [19] HSIEH Y, GAO X, WANG X, et al. Therapeutic validation of venous pulsatile tinnitus and biomaterial applications for temporal bone reconstruction surgery using multi-sensing platforms and coupled computational techniques. Front Bioeng Biotechnol. 2021;9:777648. [20] LEE J, WICK E, CHICOINE M, et al. Endonasal free flap reconstruction combined with draf frontal sinusotomy for complex cerebrospinal fluid leak: a technical report & case series. Oper Neurosurg (Hagerstown). 2021;21(6):478-484. [21] IWAMI K, FUJII M, JINGUJI S, et al. Skull base reconstruction using a temporoparietal galeal flap in simultaneous transnasal and transcranial surgery for the prevention of carotid blowout syndrome:a report of 3 cases. J Neurol Surg B Skull Base. 2021;82:e236-e242. [22] JOLLY K, GUPTA K, EGBUJI O, et al. Endoscopic transsphenoidal surgery reconstruction using the fibrin sealant patch Tachosil. Br J Neurosurg. 2021. doi: 10.1080/02688697.2021.1905771. [23] KAWAGUCHI A, SHIN M, HASEGAWA H, et al. Endoscopic extended transclival approach for lower clival meningioma. World Neurosurg. 2022;164:117. [24] KUAN E, BIRKENBEUEL J, KOVACS A, et al. Patterns of opioid usage and predictors of utilization following endoscopic skull base surgery. Laryngoscope. 2022. doi:10.1002/lary.30164. [25] KAWSAR K, LAND T, TSERMOULAS G, et al. Novel surgical treatment of recurrent csf leak by temporoparietal temporalis myofascial flap: a series of 6 cases. World Neurosurg. 2021;147:1-6. [26] KHATIWALA R, SHASTRI K, PERIS-CELDA M, et al. Endoscopic endonasal reconstruction of high-flow cerebrospinal fluid leak with fascia lata “button” graft and nasoseptal flap: surgical technique and case series. J Neurol Surg B Skull Base. 2020;81(6):645-650. [27] KIM Y, KANG H, DHO Y, et al. Multi-layer onlay graft using hydroxyapatite cement placement without cerebrospinal fluid diversion for endoscopic skull base reconstruction. J Korean Neurosurg Soc. 2021;64(4):619-630. [28] LEHMANN A, VON SNEIDERN M, SHEN S, et al. Does reconstruction affect outcomes following exclusively endoscopic endonasal resection of benign orbital tumors: a systematic review with meta-analysis. World J Otorhinolaryngol Head Neck Surg. 2022;8(1):25-35. [29] LIN F, ZHANG Y, ZHAO P, et al. Grading system and surgical strategy for temporal bone diffuse-type tenosynovial giant cell tumor. Laryngoscope. 2022;132(6):1275-1284. [30] MARTINEZ-PEREZ R, KUNIGELIS K, WARD R, et al. Hydroxyapatite cement cranioplasty for reconstruction of translabyrinthine approach:aesthetic results, long-term satisfaction, quality of life, and complications. Acta Neurochir. 2022;164(3):669-677. [31] MAO S, LI M, LI D, et al. Septal floor rotational flap pedicled on ethmoidal arteries for endoscopic skull base reconstruction. Laryngoscope. 2019;129(12):2696-2701. [32] LUO C, LIU X, XIE S, et al. Experience and modification of skull base reconstruction results in lower complications rates. Acta Neurochir. 2022;164(4):1127-1133. [33] LIU S, TANG R, LI Z, et al. Analysis of risk factors for delayed iatrogenic cerebrospinal fluid otorrhinorrhea. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021;35(12):1111-1114. [34] LIU Q, WANG H, SUN X, et al. The endoscopic transnasal approach in management of the sinonasal tumor invading the anterior skull base. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021;56(1):11-17. [35] LIN Y, LIN H, CHO D. Tension pneumoventricle after endoscopic transsphenoidal surgery for rathke cleft cyst. World Neurosurg. 2020; 135:228-232. [36] MATTAVELLI D, FIORENTINO A, TENGATTINI F, et al. Additive manufacturing for personalized skull base reconstruction in endoscopic transclival surgery: a proof-of-concept study. World Neurosurg. 2021; 155:e439-e452. [37] RAHIMLI T, HIDAYETOV T, RAJABOV T. Endoscopic endonasal approach to multilobular giant pituitary adenoma with cavernous sinus invasion and petroclival extension. World Neurosurg. 2021;147:128-129. [38] PIPKORN P, LEE J, ZENGA J, et al. Endoscopic adipofascial radial forearm free flap reconstruction of the skull base: a technical update. J Neurol Surg B Skull Base. 2021;82:e243-e247. [39] PERIS-CELDA M, CHASKES M, LEE D, et al. Optimizing sellar reconstruction after pituitary surgery with free mucosal graft: results from the first 50 consecutive patients. World Neurosurg. 2017;101: 180-185. [40] PAPAGIANNOPOULOS P, TONG C, BROWN H, et al. Comparison of high-flow CSF leak closure with nasoseptal flap following endoscopic endonasal approach in adult and pediatric populations. Int Forum Allergy Rhinol. 2022;12(3):321-323. [41] PALMA DíAZ M, MARTíNEZ ANDA J, GUERRERO SUAREZ P, et al. Endonasal endoscopic and hybrid surgery techniques for blunt trauma fractures of the skull base with cerebrospinal fluid leaks. J Craniofac Surg. 2021;32(7):2500-2507. [42] OOSTRA A, KOUTSARNAKIS C, GEORGALAS C. Advances in vascularized flaps for skull base reconstruction. Curr Opin Otolaryngol Head Neck Surg. 2021;29(1):36-43. [43] MORINAGA Y, AKUTSU H, KINO H, et al. Endoscopic endonasal dural reconstruction for a cerebrospinal fluid leak in the middle cranial fossa of a patient with gorham-stout disease with skull base defect.NMC Case Rep J. 2022;9:55-61. [44] MISSALE F, IOPPI A, ASCOLI A, et al. Cerebrospinal fluid leak repair:usefulness of intrathecal fluorescein for correct topographic identification of the skull base defects. World neurosurg. 2022;160: e267-e277. [45] TIANZHI Z, YINGWU S, ZIJIAN Y, et al. A Modified Technique to Harvest Integrated Zygomatic Arch-Temporal Bone Flap:Clinical Experience. Neurol India. 2022;70(1):325-330. [46] RAMOS-ZúñIGA R, LóPEZ-GONZáLEZ F, SEGURA-DURáN I. Bilaminar chitosan scaffold for sellar floor repair in transsphenoidal surgery. Front Bioeng Biotechnol. 2020;8:122. [47] REDDY R, GILL A, HWANG J, et al. Surgeon education through a surgical cost feedback system reduces supply cost in endoscopic skull base surgery. J Neurosurg. 2022;136(2):422-430. [48] STEIERT C, BEHRINGER S, KRAUS L, et al. Augmented reality-assisted craniofacial reconstruction in skull base lesions - an innovative technique for single-step resection and cranioplasty in neurosurgery. Neurosurg Rev. 2022. doi:10.1007/s10143-022-01784-6. [49] SHELESKO E, CHERNIKOVA N, KRAVCHUK A, et al. Multiple skull base defects:features of pathogenesis, diagnosis and treatment. Zh Vopr Neirokhir Im N N Burdenko. 2021;85(4):58-63. [50] SHAMAERAOTAN A, WEI J, MA D, et al. Immediate resection and reconstruction of encephalocele in the craniofacial region. J Craniofac Surg. 2022;33(2):e113-e116. [51] ROTARIU D, ZIYAD F, BUDU A, et al. The role of osirix based virtual endoscopy in planning endoscopic transsphenoidal surgery for pituitary adenoma. Turk Neurosurg. 2017;27(3):339-345. [52] ROCA E, PENN D, SAFAIN M, et al. Abdominal fat graft for sellar reconstruction: retrospective outcomes review and technical note. Oper Neurosurg. 2019;16(6):667-674. [53] TOSAKA M, PREVEDELLO D, YAMAGUCHI R, et al. Single-layer fascia patchwork closure for the extended endoscopic transsphenoidal transtuberculum transplanum approach: deep suturing technique and preliminary results. World Neurosurg. 2021;155:e271-e284. [54] TOTTEN D, MANZOOR N, YANCEY K, et al. Comparison of small intestinal submucosal graft and autologous tissue in prevention of CSF leak after posterior fossa craniotomy. J Neurol Surg B Skull Base. 2021;82(6):695-699. [55] TURRI-ZANONI M, AROSIO A, AGOSTI E, et al. Endoscopic-assisted orbital exenteration: technical feasibility and surgical results from a single-center consecutive series. J Craniomaxillofac Surg. 2022;50(2): 156-162. [56] WANG S, QIN Y, XIAO D, et al. Efficacy of sellar opening in the pituitary adenoma resection of transsphenoidal surgery influences the degree of tumor resection. BMC Med Imaging. 2017;17(1):45. [57] WANG S, QIN Y, XIAO D, et al. Imaging evaluation of the location and fenestration of sellar floor during endonasal transsphenoidal surgery in patients with pituitary adenomas. World Neurosurg. 2018; 116:e232-e238. [58] WANG Z, XIE Y, YANG R. Rapid reconstruction of craniotomy defects based on surgical navigation. Zhongguo Yi Liao Qi Xie Za Zhi. 2021; 45(3):246-249. [59] ZOGHEIB S, HANNA C, DAOU B, et al. Successful outcomes with flaps for recurrent cerebrospinal fluid leaks: a systematic review of the literature. J Plast Reconstr Aesthet Surg. 2022;75(4):1380-1388. [60] 王志强.严重颅底缺损模型建立及形状记忆合金支架-生物膜的研究[D].广州:南方医科大学,2012:1-103. |
| [1] | Gao Hongliang, Li Xusheng, Wang Zhenhu, Zhang Xiaomin, Li Peng, Zhang Tao, Liu Hua, Li Songkai. Three-dimensional finite element analysis of the treatment of lumbar spondylolysis with cannulated lag screw [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(22): 3451-3456. |
| [2] | Liu Chang, Liu Lei, Ma Chaoqun, Cao Chuanxu, Xu Changzhi. Influencing factors and current situation of parametric design of knee prosthesis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(22): 3587-3593. |
| [3] | Wang Zhangzheng, Mo Liang, Zhou Chi, Liu Yuhao, Yan Hongsong, He Wei. Influence of hip-preservation surgeries on subsequent total hip arthroplasty for osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(22): 3594-3601. |
| [4] | Wu Yihan, Wei Qiaoye, Pang Yu, Liu Zhongqiang. Proprioception characteristics of functional ankle instability: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(18): 2943-2952. |
| [5] | Wang Suping, Qiu Demei, Fan Zhonghe, Hu Bo. Bibliometrics and visual analysis of research in the field of rehabilitation for femoroacetabular impingement syndrome in the past decade [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(17): 2754-2762. |
| [6] | Guo Tingting, Cui Chaoqiang, Liu Baokun, Gu Hao, Zhou Dong. Application of endovascular steerable catheter system in interventional surgery [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(16): 2609-2615. |
| [7] | Wang Ling, Chen Peng, Wang Guanglan, Zheng Cheng. Effects of kinesio taping on chronic ankle instability: a systematic review and Meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(14): 2283-2290. |
| [8] | Li Wenjie, You Aijia, Zhou Junli, Fang Sujuan, Li Chun. Effects of different dressings in the treatment of burn wounds: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(7): 1141-1148. |
| [9] | Yu Jiaan, Liu Xinwei, Lian Hongyu, Liu Kexin, Li Zitao. Medial open-wedge tibial osteotomy versus lateral closed-wedge tibial osteotomy for unicompartmental knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 632-639. |
| [10] | Chai Hao, Yang Deyong, Zhang Lei, Shu Li. 3D printing personalized osteotomy guide technology versus conventional total knee arthroplasty on the accuracy of lower limb force alignment: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 646-654. |
| [11] | Wang Kaiyu, Hu Peng, Wei Zairong, Huang Guangtao, Zhou Jian, He Guijia, Nie Kaiyu. Use of expanders and implants in breast reconstruction complicated with infection [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(3): 461-469. |
| [12] | Liu Jie, Hua Qikai, Li Shanlang, Yu Jie, Su Hongjie, Ding Yi, Zhao Yongxin, Su Yongfeng, Chen Yan. Periosteum distraction for the treatment of diabetic foot ulcer: theoretical basis and clinical verification [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(32): 5236-5241. |
| [13] | Zhu Boheng, Peng Ying, Wang Hong. Mechanism and application of sterol regulatory element binding protein in wound healing [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(29): 4729-4734. |
| [14] | Hu Taotao, Chang Shusen, Wei Zairong. Macrophage polarization effectively promotes nerve regeneration after peripheral nerve injury through the M2 phenotypic regulation [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(14): 2285-2290. |
| [15] | Chen Zhengyu, Tong Jie, Li Xuelin, Yan Yiguo. Advantages and disadvantages of interbody implant materials in lumbar fusion [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(10): 1597-1603. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||