Chinese Journal of Tissue Engineering Research ›› 2023, Vol. 27 ›› Issue (4): 646-654.doi: 10.12307/2022.743
Previous Articles Next Articles
3D printing personalized osteotomy guide technology versus conventional total knee arthroplasty on the accuracy of lower limb force alignment: a meta-analysis
Chai Hao1, Yang Deyong1, Zhang Lei2, Shu Li1
- 1First Department of Joint Surgery, Sixth Affiliated Hospital of Xinjiang Medical University, Urumqi 830002, Xinjiang Uygur Autonomous Region, China; 2First Department of Surgery, Hospital Affiliated to Xinjiang Production and Construction Corps of Chinese People’s Armed Police Forces, Urumqi 830002, Xinjiang Uygur Autonomous Region, China
-
Received:2021-10-22Accepted:2021-12-22Online:2023-02-08Published:2022-06-23 -
Contact:Shu Li, Master, Associate chief physician, First Department of Joint Surgery, Sixth Affiliated Hospital of Xinjiang Medical University, Urumqi 830002, Xinjiang Uygur Autonomous Region, China -
About author:Chai Hao, Attending physician, First Department of Joint Surgery, Sixth Affiliated Hospital of Xinjiang Medical University, Urumqi 830002, Xinjiang Uygur Autonomous Region, China -
Supported by:Special Scientific Research Project for Young Medical Science and Technology Talents in Health of Xinjiang Uygur Autonomous Region, No. WJWY-202024 (to SL)
CLC Number:
Cite this article
Chai Hao, Yang Deyong, Zhang Lei, Shu Li. 3D printing personalized osteotomy guide technology versus conventional total knee arthroplasty on the accuracy of lower limb force alignment: a meta-analysis[J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 646-654.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks

2.1 文献检索结果 初检并阅读题录后得到相应文献775篇,经过阅读题目及摘要后,初步纳入125篇文献,仔细阅读全文,排除质量较低的文献95篇,最后30篇文献符合纳入标准[12-41],筛选流程见图2。"


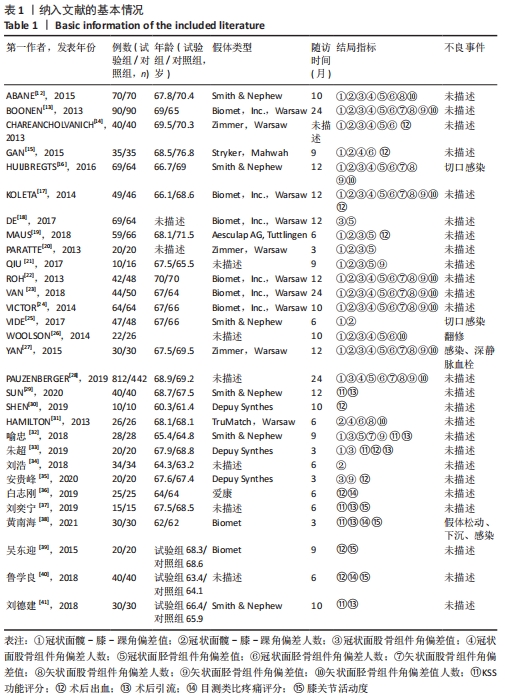
纳入研究的基本情况见表1。 "
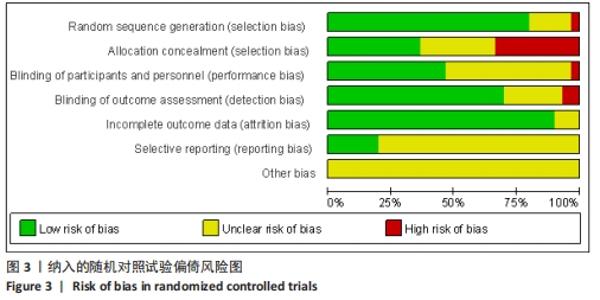
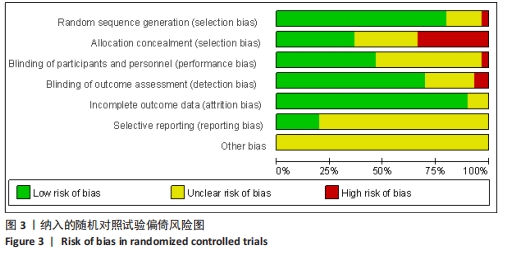
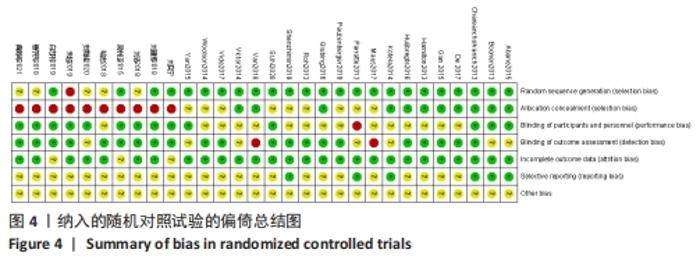
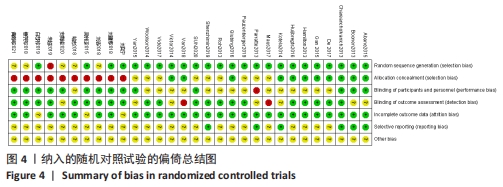
纳入的研究均为随机对照试验,使用Cochrane偏倚风险评估图及偏倚风险总结图进行文献质量评估,见图3,4。 "
"
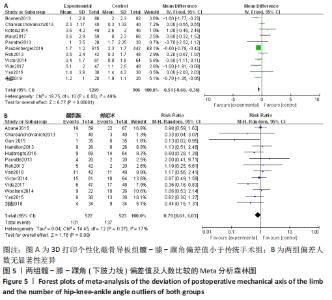
2.2 Meta分析结果 2.2.1 各组髋-膝-踝角(下肢力线)偏差值及人数(偏离理想角度±3°)差异 有11个研究比较了冠状位髋-膝-踝角(下肢力线)偏差值[13-14,17,19-20,22,24-25,27-28,33]。异质性检验结果表明,各研究间有中度异质性(I2=49%),采用固定效应模型进行合并分析,Meta分析结果显示,2种手术方法冠状面髋-膝-踝角(下肢力线)偏差值差异有显著性意义(MD=-0.51,95%CI:-0.66至-0.36,P < 0.000 01),截骨导板组髋-膝-踝角(下肢力线)偏差值小于传统手术组。有13个研究比较了冠状面髋-膝-踝角偏离理想角度±3°的人数[12,14-15,16,20,22-27,31,34]。异质性检验结果表明,各研究间有低度异质性(I2=17%),采用固定效应模型进行合并分析,Meta分析结果显示,此2种手术方法髋-膝-踝角偏离理想角度±3°的人数差异无显著性意义(RR=0.79,95%CI:0.61-1.03,P=0.08)。具体结果见图5。"
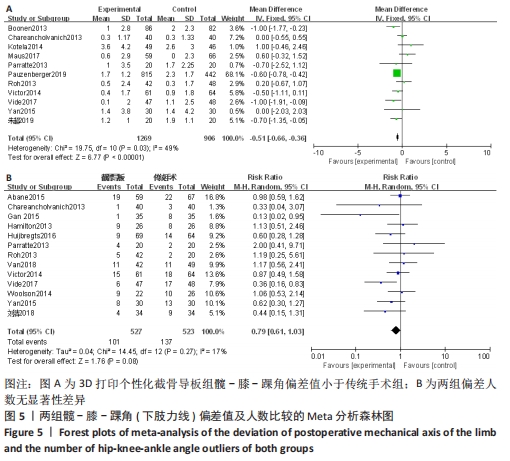
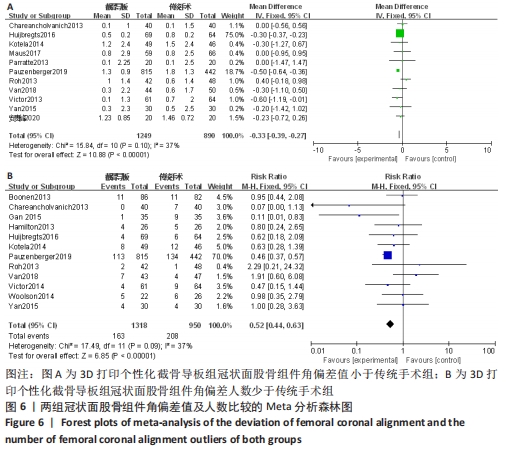
2.2.2 各组冠状面股骨组件角偏差值及人数(偏离理想角度±3°)差异 有11个研究比较了冠状面股骨组件角偏差值[14,16-17,19-20,22-24,27-28,35]。异质性检验结果表明,各研究间异质性较低(I2=37%),采用固定效应模型进行合并分析,Meta分析结果显示,2种手术方法冠状面股骨组件角偏差值差异有显著性意义(MD=-0.33,95%CI:-0.39至-0.27,P < 0.000 01),截骨导板组冠状面股骨组件角偏差值小于传统手术组。有12项研究比较了冠状面股骨组件偏离理想角度±3°的人数[13-17,22-24,26-28,31]。异质性检验结果表明,各研究间为低度异质性(I2=37%),采用固定效应模型进行合并分析,Meta分析结果显示,2种手术方法冠状面股骨组件角偏离理想角度±3°的人数差异有显著性意义(RR=0.52,95%CI:0.44-0.63,P < 0.000 01),冠状面股骨组件角偏离理想角度±3°的人数少于传统手术组。见图6。"

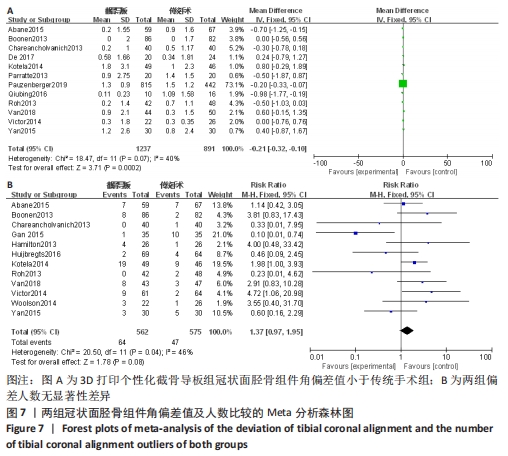
2.2.3 各组冠状面胫骨组件角偏差值及人数(偏离理想角度±3°)差异 有12项研究比较了冠状面胫骨组件角偏差值[12-14,17-18,20-24,27-28]。异质性检验结果表明,各研究间有中度异质性(I2=40%),采用固定效应模型进行合并分析,Meta分析结果显示,2种手术方法冠状面胫骨组件角偏差值差异有显著性意义(MD=-0.21,95%CI:-0.32至-0.10,P=0.000 2),截骨导板组冠状面胫骨组件角偏差值小于传统手术组。共12项研究比较了冠状面胫骨组件偏离理想角度±3°的人数[12-17,22-24,26-27,31]。 异质性检验结果表明,各研究间有中度异质性(I2=46%),采用固定效应模型进行合并分析,Meta分析结果显示,2种手术方法冠状面胫骨组件角偏离理想角度±3°的人数差异无显著性意义(RR=1.37,95%CI:0.97-1.95,P=0.08),见图7。"
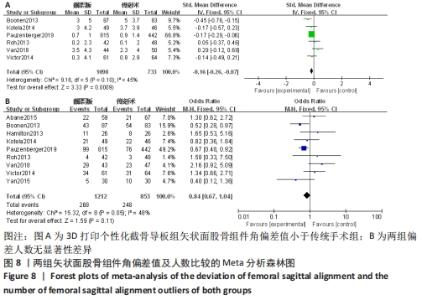
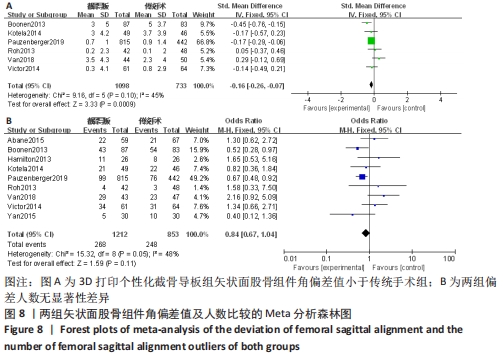
2.2.4 各组矢状面股骨组件角偏差值及人数(偏离理想角度±3°)差异 有6项研究比较了矢状面股骨组件角偏差值[13,17,22-24,27-28]。异质性检验结果表明,各研究间为中度异质性(I2=45%),采用固定效应模型进行合并分析,Meta分析结果显示,2种手术方法矢状面股骨组件角偏差值差异有显著性意义(SMD=-0.16,95%CI:-0.26至-0.07,P=0.000 9),截骨导板组矢状面股骨组件角偏差值小于传统手术组。有9项研究比较了矢状面股骨组件偏离理想角度±3°的人数[12-13,17,22-24,27-28,31]。异质性检验结果表明,各研究间有中度异质性(I2=48%),采用固定效应模型进行合并分析,Meta分析结果显示,2种手术方法矢状面股骨组件角偏离理想角度±3°的人数差异无显著性意义(RR=0.84,95%CI:0.67-1.04,P=0.11)。具体结果见图8。"
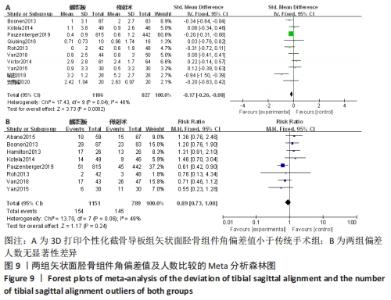
2.2.5 各组矢状面胫骨组件角偏差值及人数(偏离理想角度±3°)的差异 有10项研究比较了矢状面胫骨组件角偏差值[13,17,21-24,27-28,32,35]。异质性检验结果表明,各研究间有中度异质性(I2=48%),采用固定效应模型进行合并分析,Meta分析结果显示,2种手术方法矢状面胫骨组件角偏差值差异有显著性意义(MD=-0.17,95%CI:-0.26至-0.08,P=0.000 2),截骨导板组矢状面胫骨组件角偏差值小于传统手术组。8项研究比较了矢状面胫骨组件偏离理想角度±3°的人数[12-13,17,22-23,27-28,31]。异质性检验结果表明,各研究间为中度异质性(I2=49%),采用固定效应模型进行合并分析,Meta分析结果显示,2种手术方法矢状面胫骨组件角偏离理想角度±3°的人数差异无显著性意义(RR=0.89,95%CI:0.73-1.08,P=0.24)。具体结果见图9。"

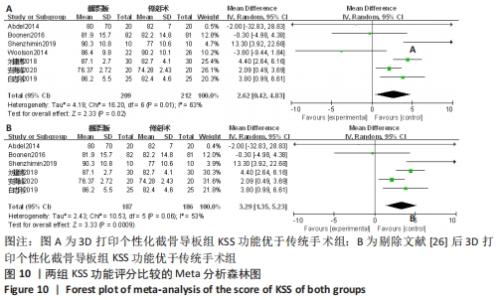
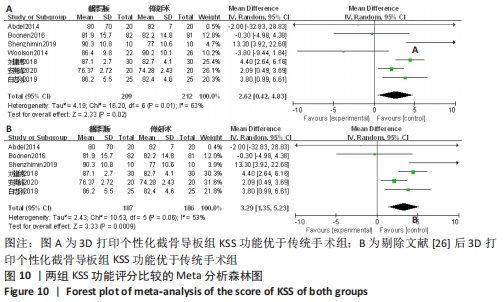
2.2.6 各组KSS功能评分差异 有7项研究比较了KSS功能评分[12-13,26,29,35-36,41]。异质性检验结果表明,各研究间异质性偏高(I2=63%,P=0.01),通过逐一剔除的方法对纳入文献进行敏感性分析,将1篇文献剔除时异质性下降最大(I2=53%,P=0.06)[26],但结果未发生改变,提示研究结果较为稳定。仔细阅读文献,考虑可能是假体类型及是否进行术后功能锻炼造成的异质性,采用随机效应模型进行合并分析,结果显示,此2种手术方法KSS功能评分差异有显著性意义(MD=3.29,95%CI:1.35-5.23,P=0.000 9),截骨导板组KSS功能优于传统手术。具体结果见图10。"
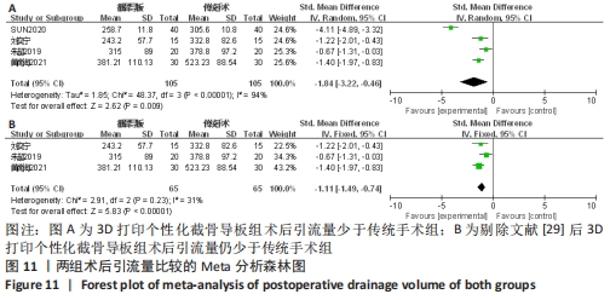
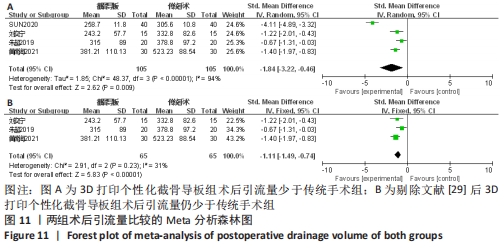
2.2.7 各组术后引流量差异 有3项研究比较了术后引流量[33,37-38]。异质性检验结果表明,各研究间异质性高(I2=94%, P < 0.000 01),通过逐一剔除的方法对纳入文献进行敏感性分析, 将1篇文献剔除后异质性明显下降(I2=31%,P=0.23) [29],但结果未发生改变,提示研究结果较为稳定,仔细阅读文献,考虑可能是手术时间和假体类型等因素所造成的异质性,采用固定效应模型进行合并分析,Meta分析结果显示,此2种手术方法术后引流量差异有显著性意义(SMD=-1.11,95%CI:-1.49至-0.74,P < 0.000 1)。截骨导板组术后引流量少于传统手术。具体结果见图11。"
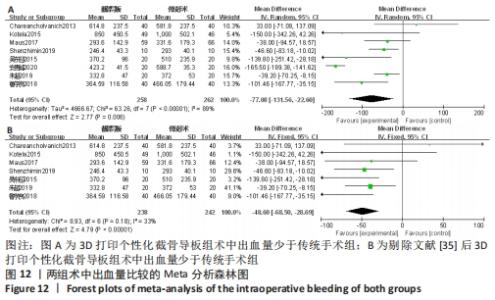
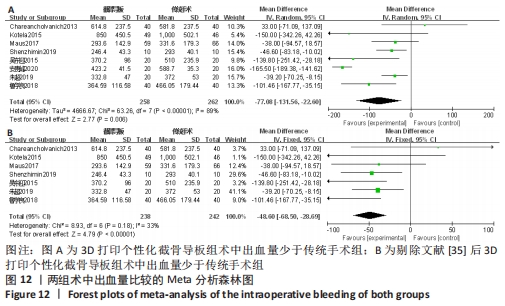
2.2.8 各组术中出血量差异 有8项研究比较了术中出血量[14,17,19,29,33,35,39-40]。异质性检验结果表明,各研究间异质性高(I2=89%,P < 0.000 01),通过逐一剔除的方法对纳入文献进行敏感性分析,将1篇文献剔除后异质性明显下降(I2=33%,P=0.18)[35],但结果未发生改变,提示研究结果较为稳定,仔细阅读文献,考虑可能是手术熟练程度和止血带使用等因素所造成的异质性,采用固定效应模型进行合并分析,结果显示,此2种方法术中出血量差异有显著性意义(MD=-48.60,95%CI:-68.50至-28.69,P < 0.000 1)。截骨导板组术中出血少于传统手术。具体结果见图12。"
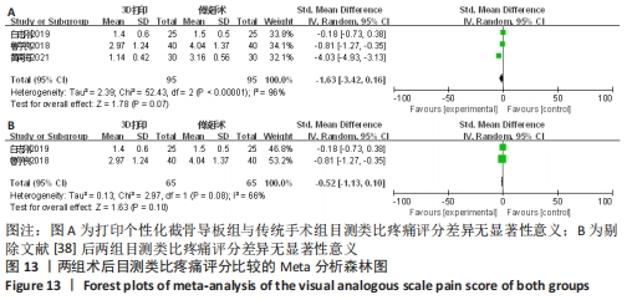
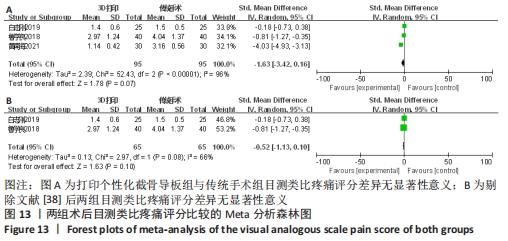
2.2.9 各组目测类比疼痛评分差异 有3项研究比较了目测类比疼痛评分[36,38,40]。异质性检验结果表明,各研究间异质性高(I2=96%),通过逐一剔除的方法对纳入文献进行敏感性分析,将1篇文献剔除后异质性明显下降 (I2=66%,P=0.08)[38],但结果未发生改变,提示研究结果较为稳定,仔细阅读文献,考虑可能是随访时间不同等因素所造成的异质性,故采用随机效应模型进行合并分析,Meta分析结果显示,2种手术方法术后目测类比疼痛评分差异无显著性意义(SMD=-0.52,95%CI:-1.13-0.10,P=0.10)。具体结果见图13。"
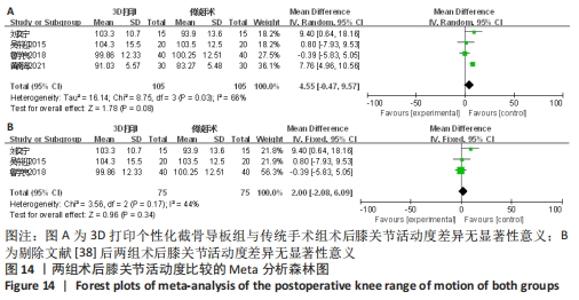
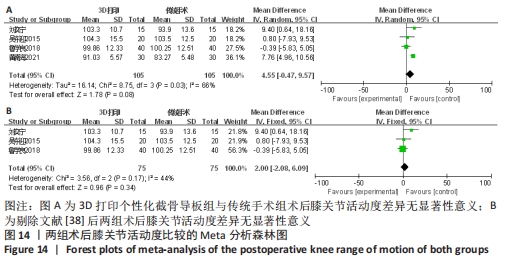
2.2.10 各组膝关节活动度差异 有4项研究比较了术后膝关节活动度[37-40]。异质性检验结果表明,各研究间异质性较高(I2=66%,P=0.03),通过逐一剔除的方法对纳入文献进行敏感性分析,发现剔除一篇文献后异质性显著下降(I2=44%,P=0.17) [38],但结果未发生改变,提示研究结果较为稳定,仔细阅读文献,考虑可能是假体类型不同和随访时间不同所造成的异质性,采用固定效应模型进行合并分析,结果显示,此2种方法术后膝关节活动度差异无显著性意义(MD=2.00,95%CI:-2.08-6.09,P=0.34)。具体结果见图14。"

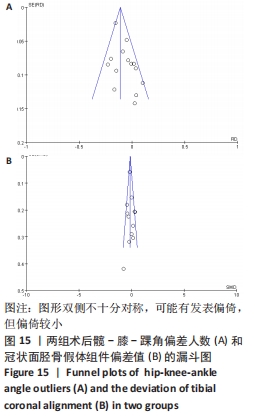
2.3 纳入文献发表偏倚分析 以纳入研究最多的髋-膝-踝角偏离理想角度±3°的人数指标做漏斗图,可见图形双侧不十分对称,可能有发表偏倚,但偏倚较小,见图15A。再以主要结局指标之一的冠状面胫骨假体组件偏差值做漏斗图,可见图形双侧不十分对称,可能有发表偏倚,但偏倚较小,见图15B。"
| [1] EVERHART JS, ABOULJOUD MM, KIRVEN JC, et al. Full-thickness cartilage defects are important independent predictive factors for progression to total knee arthroplasty in older adults with minimal to moderate osteoarthritis: data from the osteoarthritis initiative. J Bone Joint Surg (Am). 2019; 101(1):56-63. [2] KOBAYASHI S, NIKI Y, HARATO K, et al. Rheumatoid arthritis patients achieve better satisfaction but lower functional activities as compared to osteoarthritis patients after total knee arthroplasty. J Arthroplasty. 2019;34(3):478-482. [3] GUI Q, ZHANG X, LIU L, et al. Cost-utility analysis of total knee arthroplasty for osteoarthritis in a regional medical center in China. Health Econ Rev. 2019;9(1):15. [4] ZHOU FX, XUE F, ZHANG SQ. The application of 3D printing patient specific instrumentation model in total knee arthroplasty. Saudi J Biol Sci. 2020;27(5): 1217-1221. [5] HAFEZ MA, CHELULE KL, SEEDHOM BB, et al. Computer-assisted total knee arthroplasty usingpatient -specific templating. Clin Orthop Relat Res. 2006;444:184-192. [6] RENSON L, POILVACHE P, VAND WH. Improved alignment and operating room efficiency with patient-specific instrumentation for TKA. Knee. 2014;21(6): 1216-1220. [7] ANDERL W, PAUZENBERGER L, KÖLBLINGER R, et al. Patient-specific instrumentation improved mechanical alignment, while early clinical outcome was comparable to conventional instrumentation in TKA. Knee Surg Sports Traumatol Arthrosc. 2016; 24(1):102-111. [8] LUSTIG S, SCHOLES C, OUSSEDIK S, et al. Unsatisfactory accuracy with VISIONAIRE patient-specific cutting jigs for total knee arthroplasty. J Arthroplasty. 2014;29(1): 249-250. [9] RANDELLI PS, MENON A, PASQUALOTTO S, et al. Patient-specific instrumentation does not affect rotational alignment of the femoral component and perioperative blood loss in total knee arthroplasty: a prospective, randomized, controlled trial. J Arthroplasty. 2019;34(7):1374-1381. [10] 韩衍龙,哈巴西·卡肯,赵巍,等.3D打印技术辅助全膝关节置换临床疗效的Meta分析[J].生物骨材料与临床研究, 2021,18(5):47-56. [11] KIZAKI K, SHANMUGARAJ A, YAMASHITA F, et al. Total knee arthroplasty using patient-specific instrumentation for osteoarthritis of the knee: a meta-analysis. BMC Musculoskelet Disord. 2019;20(1):561. [12] ABANE L, ANRACT P, BOISGARD S, et al. A comparison of patient‐specific and conventional instrumentation for total knee arthroplasty: a multicentre randomised controlled trial. Bone Jt J. 2015;97-B:56-63. [13] BOONEN B, SCHOTANUS MG, KERENSB, et al. Intra-operative results and radiological outcome of conventional and patient-specific surgery in total knee arthroplasty:a multicentre, randomised controlled trial.Knee Surg Sports Traumatol Arthrosc. 2013; 21(10):2206-2212. [14] CHAREANCHOLVANICH K, NARKBUNNAM R, PORNRATTANAMANEEWONG C. A prospective randomised controlled study of patient-specific cutting guides compared with conventional instrumentation in total knee replacement. Bone Joint J. 2013;95(3): 354-359. [15] GAN Y, DING J, XU Y, et al. Accuracy and efficacy of osteotomy in total knee arthroplasty with patient-specific navigational template. Int J Clin Exp Med. 2015;8(8):12192-12201. [16] HUIJBREGTS HJ, KHAN RJ, FICK DP, et al. Component alignment and clinical outcome following total knee arthroplasty:a randomised controlled trial comparing an intramedullary alignment system with patient-specific instrumentation. Bone Jt J. 2016;98-B(8):1043-1049. [17] KOTELA A, KOTELA I. Patient-specific computed tomography based instrumentation in total knee arthroplasty: a prospective randomized controlled study. Int Orthop. 2014;38(10):2099-2107. [18] DE RV, PELLIKAAN P, DHOLLANDER A, et al. Three-dimensional analysis of accuracy of component positioning in total knee arthroplasty with patient specific and conventional instruments: a randomized controlled trial. Knee. 2017;24(6):1469-1477. [19] MAUS U, MARQUES CJ, SCHEUNEMANN D, et al. No improvement in reducing outliers in coronal axis alignment with patient-specific instrumentation. Knee Surg Sports Traumatol Arthrosc. 2018;26(9):2788-2796. [20] PARRATTE S, BLANC G, BOUSSEMART T, et al. Rotation in total knee arthroplasty:no difference between patient-specific and conventional instrumentation. Knee Surg Sports Traumatol Arthrosc. 2013;21(10): 2213-2219. [21] QIU B, LIU F, TANG BS, et al. Clinical study of 3D imaging and 3D printing technique for patient-specific instrumentation in total knee Arthroplasty. J Knee Surg. 2017; 30(8):822-828. [22] ROH YW, KIM TW, LEE S, et al. Is TKA using patient-specific instruments comparable to conventional TKA? A randomized controlled study of one system. Clin Orthop Relat Res. 2013;471(12):3988-3995. [23] VAN JL, SNORRASON F, RÖHRL SM. No radiological and clinical advantages with patient-specific positioning guides in total knee replacement. Acta Orthop. 2018;89(1): 89-94. [24] VICTOR J, DUJARDIN J, VANDENNEUCKER H, et al. Patient-specific guides do not improve accuracy in total knee arthroplasty: a prospective randomized controlled trial. Clin Orthop Relat Res. 2014;472(1):263-271. [25] VIDE J, FREITAS TP, RAMOS A, et al. Patient-specific instrumentation in total knee arthroplasty: simpler, faster and more accurate than standard instrumentation-a randomized controlled triall. Knee Surg Sports Traumatol Arthrosc. 2017;25(8):2616-2621. [26] WOOLSON ST, HARRIS AH, WAGNER DW, et al. Component alignment during total knee arthroplasty with use of standard or custom instrumentation:a randomized clinical trial using computed tomography for postoperative alignment measurement. J Bone Jt Surg Am. 2014;96(5):366-372. [27] YAN CH, CHIU KY, NG FY, et al. Comparison between patient-specific instruments and conventional instruments and computer navigation in total knee arthroplasty: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc. 2015;23(12):3637-3645. [28] PAUZENBERGER L, MUNZ M,BRANDL G, et al. Patient-specific instrumentation improved three-dimensional accuracy in total knee arthroplasty: a comparative radiographic analysis of 1257 total knee arthroplasties. J Orthop Surg Res. 2019; 14(1):437. [29] SUN ML, ZHANG Y, PENG Y, et al. Accuracy of a novel 3D-printed patient-specific intramedullary guide to control femoral component rotation in total knee arthroplasty. Orthop Surg. 2020;12(2):429-441. [30] SHEN ZM, WANG H, DUAN YQ, et al. Application of 3D printed osteotomy guide plate-assisted total knee arthroplasty intreatment of valgus knee deformity. J Orthop Surg Res. 2019;14(1):327. [31] HAMILTON WG, PARKS NL, SAXENA A. Patient-specific instrumentation does not shorten surgical time: a prospective, randomized trial. J Arthroplasty. 2013;28(8 Suppl):96-100. [32] 喻忠,刘帅,顾强,等.3D打印个性化导航定位导板在全膝关节表面置换中的应用[J].中国数字医学,2018,13(2):2-4. [33] 朱超,王斌,殷建,等.个性化截骨工具辅助下人工全膝关节置换与传统人工全膝关节置换手术精确度及临床疗效比较[J].生物骨科材料与临床研究,2019, 16(3):54-58. [34] 刘浩,吴博,郑清源,等.个性化股骨远端截骨导向器与传统手术工具在微创入路膝关节置换中的应用对比[J].中华保健医学杂志,2018,20(3):198-202. [35] 安贵峰,王明月.3D打印截骨导板在人工全膝关节置换中的临床应用研究[J].中国实用医药,2020,15(17):98-100. [36] 白志刚,刘泽欣,宋强,等.3D打印技术在全膝关节置换中的临床应用研究[J].宁夏医学杂志,2019,41(10):879-881. [37] 刘奕宁,刘利春,李晓彬,等.3D打印截骨导板在TKA术中的应用效果分析[J].中国骨与关节损伤杂志,2019,34(2):142-145. [38] 黄南海,吴晓鹏,周晓春.3D打印截骨导板用于全膝关节置换术的临床价值分析[J].中外医疗,2021,40(6):41-44. [39] 吴东迎,袁峰,吴继彬,等.3D打印截骨导板在人工全膝关节置换中的应用[J].中华骨科杂志,2015,35(9):921-926. [40] 鲁学良,熊明月,刘振辉,等.3D打印截骨导板在人工全膝关节置换中的应用研究[J].中国临床实用医学,2018,9(3):57-59. [41] 刘德健,李彦林,蔡国锋,等.3D打印截骨导板辅助人工全膝关节置换术早期疗效分析[J].中国修复重建外科杂志, 2018,32(7):899-905. [42] MAHALUXMIVALA J, BANKES MJ, NICOLAI P, et al. The effect of surgeon experience on component positioning in 673 Press Fit Condylar posterior cruciate-sacrificing total knee arthroplasties. J Arthroplasty. 2001;16(5):635-640. [43] PULIERO B, FAVREAU H, EICHLER D, et al. Total knee arthroplasty in patients with varus deformities greater than ten degrees: survival analysis at a mean ten year follow-up. Int Orthop. 2019;43(2):333-341. [44] SUN H, LI S, WANG K, et al. Efficacy of portable accelerometer-based navigation devices versus conventional guides in total knee arthroplasty: a meta-analysis. J Knee Surg. 2020;33(7):691-703. [45] JOHNSTON H, ABDELGAIED A, PANDIT H, et al. The effect of surgical alignment and soft tissue conditions on the kinematics and wear of a fixed bearing total knee replacement. J Mech Behav Biomed Mater. 2019;100:103386. [46] 杨硕,冯硕,徐崇俊,等.全膝关节置换后下肢力线及假体力线与疗效和假体松动率的关系[J].中国组织工程,2019, 23(24):3780-3785. [47] HUANG TW, LEE CY, LIN SJ, et al. The influence of alignment on midterm outcome after total knee arthroplasty in patients with marked coronal femoral bowing. J Arthroplasty. 2015;30(9):1531-1536. [48] OUSSEDIK S, ABDEL MP, VICTOR J, et al. Alignment in total knee arthroplasty. Bone Joint J. 2020;102-B(3):276-279. [49] RITTER MA, DAVIS KE, MEDING JB, et al. The effect of alignment and BMI on failure of total knee replacement. J Bone Joint Surg Am. 2011;93(17):1588-1596. [50] KIM YH, PARK JW, KIM JS, et al. The relationship between the survival of total knee arthroplasty and postoperative coronal, sagittal and rotational alignment of knee prosthesis. Int Orthop. 2014;38(2): 379-385. [51] KINZEL V, LEDGER M, SHAKESPEARE D. Can the epicondylar axis be defined accurately in total knee arthroplasty? Knee. 2005;12:293-296. [52] GROMOV K, KORCHI M, THOMSEN MG, et al. What is the optimal alignment of the tibial and femoral components in knee arthroplasty? Acta Orthopaedica. 2014; 85(5):480-487. [53] APLAN N, KADER DF. Rationale of the knee society clinical rating system. Clin Orthop Relat Res. 1989;248(248):13-14. [54] 张国宁,王友.膝关节评分标准的评估[J].中华外科杂志,2006,44(16):1141-1143. [55] LONGSTAFF LM, SLOAN K, STAMP N, et al. Good alignment after total knee arthroplasty leads to faster rehabilitation and better function. J Arthroplasty. 2009;24(4):570-578. [56] MAGNUSSEN RA, WEPPE F, DEMEY G, et al. Residual varus alignment does not compromise results of tkas in patients with preoperativevarus. Clin Orthop Relat Res. 2011;469(12):3443-3450. [57] YILDIZ C, KOCA K, KOCAK N, et al. Late tourniquet release and drain clamping reduces postoperative blood loss in total knee arthroplasty. HSS J. 2014;10(1):2-5. [58] KOH IJ, CHO WS, CHOI NY, et al. Causes,risk factors,and trends in failures after tka in korea over the past 5 years: a multicenter study. Clin Orthop Relat Res. 2014;472(1):316-326. |
| [1] | Li Yaping, Liu Hong, Gao Zhen, Chen Xiaolin, Huang Wujie, Jiang Zheng. Three-dimensional motion analysis of lower limb biomechanical performance in Tai Chi practitioners accompanied by knee joint pain [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 520-526. |
| [2] | Wei Bo, Yao Qingqiang, Tang Cheng, Li Xuxiang, Xu Yan, Wang Liming. Advantage of medial pivot prosthesis in total knee arthroplasty via medial subvastus approach [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 552-557. |
| [3] | Wan Guoli, Shi Chenhui, Wang Weishan, Li Ang, Shi Xunda, Cai Yi. Retrospective analysis of the influencing factors of chronic pain after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 558-564. |
| [4] | Gu Mingxi, Wang Bo, Tian Fengde, An Ning, Hao Ruihu, Wang Changcheng, Guo Lin. Comparison of early efficacy and safety of simultaneous and staged bilateral total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 565-571. |
| [5] | Zhang Jinbiao, Li Xiaoming, Xing Wanlin, Ma Fei, Yu Qiaoya, Dai Rongqin. Early warning efficacy of thrombus molecular markers after total knee arthroplasty in patients complicated with venous thromboembolism [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 572-577. |
| [6] | Xu Xiangjun, Wang Chao, Song Qunshan, Li Bingyan, Zhang Jichao, Wang Guodong, Dong Yuefu. Optimal angle for prosthesis implantation in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 612-618. |
| [7] | Yu Jiaan, Liu Xinwei, Lian Hongyu, Liu Kexin, Li Zitao. Medial open-wedge tibial osteotomy versus lateral closed-wedge tibial osteotomy for unicompartmental knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 632-639. |
| [8] | Xu Yangyang, He Peiliang, Meng Qingqi, Li Siming. A meta-analysis of the effects of continuous adductor canal block and continuous femoral nerve block on early activity after knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(4): 640-645. |
| [9] | Zhai Hongjie, Han Guanda, Li Lei, Dong Xiaohui, Jiang Zhiquan, Lou Feiyun. 3D printed polyetheretherketone material for skull defect repair [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(3): 380-384. |
| [10] | Jiang Haifang, Liu Rong, Hu Peng, Chen Wei, Wei Zairong, Yang Chenglan, Nie Kaiyu. Application of 3D printing technology in the precise and personalized treatment of cleft lip and palate [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(3): 413-419. |
| [11] | You Aijia, Li Wenjie, Zhou Junli, Li Chun. Systematic evaluation of six dressings on wound safety following total hip and knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(3): 486-492. |
| [12] | Zhao Feng, Fan Shaoqing, Cheng Xiaoyan, Li Xiaona, Li Changsheng, Ma Haojie. miR-132-3p targets and modulates Ptch1 to reduce neuropathic pain in mice with chronic constriction injury [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(2): 230-236. |
| [13] | Hu Fei, Wang Jie. Safety and efficacy of mesenchymal stem cells in the treatment of ischemic stroke: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2023, 27(1): 76-82. |
| [14] | Jing Jinpeng, Zhang Yue, Liu Xiaomin, Liu Yi. Traditional Chinese medicine injection for promoting blood circulation in prevention of deep vein thrombosis after orthopedic surgery: network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1467-1476. |
| [15] | Kan Houming, Fan Lijun, Chen Xuetai, Shen Wen. Application of platelet-rich plasma in neuropathic pain [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1286-1292. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||