中国组织工程研究 ›› 2026, Vol. 30 ›› Issue (17): 4472-4486.doi: 10.12307/2026.183
• 组织构建循证医学 evidence-based medicine in tissue construction • 上一篇 下一篇
缺血预处理影响运动表现的系统评价与多层次荟萃分析
张益林1,徐 恺2,殷明越2,孔 昊1,刘承豪1,谢 云1
- 1天津体育学院运动训练学院,天津市 301617;2上海体育大学竞技运动学院,上海市 200438
-
收稿日期:2025-06-06接受日期:2025-09-17出版日期:2026-06-18发布日期:2025-12-03 -
通讯作者:谢云,博士,教授,博士生导师,天津体育学院运动训练学院,天津市 301617 -
作者简介:张益林,男,2000年生,四川省广元市人,汉族,天津体育学院在读硕士,主要从事运动训练科学化中的运动表现研究。 并列第一作者:徐恺,男,1998年生,安徽省蒙城县人,汉族,上海体育大学在读硕士,主要从事优化运动任务中的运动表现研究。 并列第一作者:殷明越,男,2000年生,四川省成都市人,汉族,上海体育大学在读硕士,主要从事优化心脏代谢健康的新兴运动策略及机制研究。
Effects of ischemic preconditioning on sport performance: a systematic review and multilevel meta-analysis
Zhang Yilin1, Xu Kai2, Yin Mingyue2, Kong Hao1, Liu Chenghao1, Xie Yun1
- 1School of Sports Training, Tianjin University of Sport, Tianjin 301617, China; 2School of Sports Performance, Shanghai University of Sport, Shanghai 200438, China
-
Received:2025-06-06Accepted:2025-09-17Online:2026-06-18Published:2025-12-03 -
Contact:Xie Yun, PhD, Professor, Doctoral supervisor, School of Sports Training, Tianjin University of Sport, Tianjin 301617, China -
About author:Zhang Yilin, MS candidate, School of Sports Training, Tianjin University of Sport, Tianjin 301617, China Xu Kai, MS candidate, School of Sports Performance, Shanghai University of Sport, Shanghai 200438, China Yin Mingyue, MS candidate, School of Sports Performance, Shanghai University of Sport, Shanghai 200438, China Zhang Yilin, Xu Kai and Yin Mingyue contributed equally to this work.
摘要:

文题释义:
缺血预处理方案:指缺血与再灌注的组数与持续时间,例如3×5 min方案,即缺血5 min,再灌注5 min,共3组。
安慰剂:指假性缺血与再灌注,通常施加较小甚至可忽略不计的压力值于肢体近心端。
运动表现:此研究通过一系列综合指标来代替运动表现,包括平衡能力、跳跃、力量、最大氧亏累积、输出功率、重复次数、计时赛成绩、力竭测试时间和摄氧量。
目的:运动表现提升一直是体育科学关注的焦点。缺血预处理作为一种非药物干预手段已被证实可提升运动表现,然而其效果在不同研究中存在分歧,影响因素尚不明确。此项研究旨在对缺血预处理结合运动的原创研究进行系统荟萃分析,探讨其实际效应及潜在调节机制。
方法:依据《系统综述与元分析优先报告条目》规范,于2024-09-04检索Web of Science核心合集、PubMed、Embase与中国知网数据库,以“ischemic preconditioning,performance,sport,缺血预处理”等为关键词。纳入标准:①非疾病人群;②缺血预处理对照为假性缺血预处理或无缺血处理;③结局指标包括平衡、跳跃、力量、氧亏、功率、重复次数、计时成绩、力竭时间与摄氧量等;④研究类型为随机对照试验或随机交叉研究。采用Cochrane Risk of Bias 2.0与GRADE评估偏倚风险与证据等级;使用R 4.3.3中的“meta”“metafor”以及“clubSandwich”包进行多层次效应合并、发表偏倚检验、亚组及回归分析。
结果:共纳入90篇文献,1 439名受试者,年龄在18-70岁。①相比假性缺血预处理或空白对照,缺血预处理可有效提高运动表现[ES=0.13,95%CI(0.06,0.21),P < 0.01,Q=427,I2-Level 2=0%,I2-Level 3=9.13%,I2-Level 4=5.74%,PI(-0.18,0.44),低证据等级]。②亚组组间分析发现缺血预处理组 vs.空白对照组的效果提升显著大于(P=0.02)缺血预处理组 vs. 假性缺血预处理组[ESCON=0.22,95%CI(0.12,0.33),P < 0.01;ESSHAM=0.10,95%CI (0.02,0.18),P < 0.01]。③不同能量代谢特点(无氧或有氧运动)、运动经验水平、性别组间未发现显著差异。④缺血预处理方案中,发现仅1篇的1×5 min方案显著大于其余所有方案(P=0.01)。组内差异发现,仅3×5 min [ES=0.14,95%CI (0.03,0.26),P < 0.01]、4×5 min[ES=0.10,95%CI (0.00,0.21),P=0.02]方案在统计学上显著。⑤久坐不动者[ES=0.14,95%CI(-0.10,0.39,P=0.03]、休闲活动者[ES=0.15,95%CI(0.03,0.27),P=0.02]、发展或训练中受试者 [ES=0.19,95%CI (0.04,0.33),P=0.01]的运动表现显著提高;高度训练或国家级运动员、精英或国际级运动员,以及世界级运动员的运动表现变化均不显著。仅男性受试者[ES=0.20,95%CI (0.10,0.30),P < 0.01]在统计学上显著。
结论:缺血预处理对运动表现的提升效果微弱,且存在显著的安慰剂效应(心理作用)。缺血预处理方案(缺血再灌注时长)也是影响运动表现的一个调节因子,其中3×5 min或4×5 min的方案效果最佳。运动经验水平较低的男性反应更为显著,但性别、经验以及年龄作为调节因子尚无明确统计学结果支持。未来研究应加强对安慰剂效应的控制,采用标准化的缺血和再灌注方案深入探索缺血预处理的独立效应与适用边界。
https://orcid.org/0009-0003-3285-0851(张益林);https://orcid.org/0009-0005-1960-671X(谢云)
中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
中图分类号:
引用本文
张益林, 徐 恺, 殷明越, 孔 昊, 刘承豪, 谢 云. 缺血预处理影响运动表现的系统评价与多层次荟萃分析[J]. 中国组织工程研究, 2026, 30(17): 4472-4486.
Zhang Yilin, Xu Kai, Yin Mingyue, Kong Hao, Liu Chenghao, Xie Yun. Effects of ischemic preconditioning on sport performance: a systematic review and multilevel meta-analysis[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(17): 4472-4486.
2.2 纳入研究特征 附表1-3提供了90篇纳入文献的详细研究特征列表[5,10-21,23-27,29-30,32-33,35-39,59,67-128],涵盖人口统计学因素和缺血预处理相关参数。90篇文献均为随机交叉试验或随机对照试验,共涉及1 439名参与者,其中包括1 033名男性和210名女性,另有196名参与者的性别在研究中未明确报告。根据运动持续时间75 s的标准[45-46],46篇文献被归类为无氧运动研究(附表1)[11-16,23-24,26-27,29-30,69-102],41篇文献被归类为有氧运动研究(附表2)[5,10,17-21,32-33,35-39,59,103-128],3篇文献同时报告了无氧和有氧运动的结果(附表3)[25,67-68]。
2.3 偏倚风险 所有纳入研究的总体偏倚风险被评估为“存在一些担忧”。根据RoB 2.0工具,主要原因是:①未报告参与者的基线特征;②受试者未完全参与,导致部分结果数据缺失(图2)。
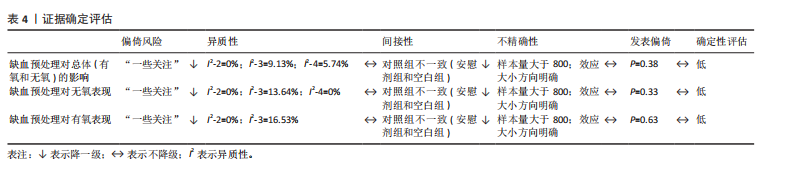
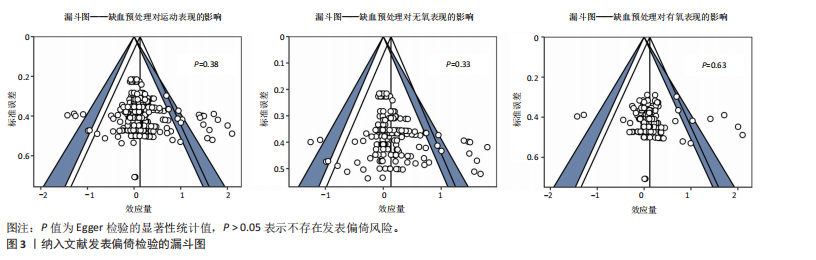
2.4 发表偏倚与证据等级质量评估 漏斗图显示对称分布,且Egger检验结果不显著(图3),表明此研究不存
在发表偏倚风险。
鉴于不存在发表偏倚和较高异质性(图3),同时样本量为1 439(超过800),因此未进行降级。然而,偏倚风险被认为“存在一些担忧”,导致证据质量从高降至中。此外,观察到“间接性”不一致,参考组为假性缺血预处理和空白对照,因此进一步降级。最终,此研究的证据等级被降2级,最终评定为低(表4)。
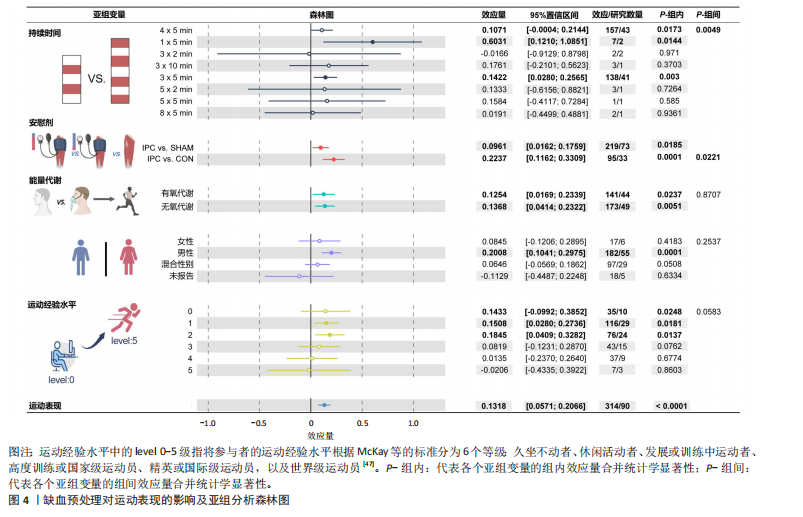
2.5 缺血预处理对运动表现的效应量 纳入90篇文献(314项效应,1 439名受试者)荟萃分析发现(图4),缺血预处理结合运动能够显著提高运动表现但效果较小[ES=0.13,95%CI(0.06,0.21),P < 0.01,Q=427,I2-Level 2=0%,I2-Level 3=9.13%,I2-Level 4=5.74%,PI(-0.18,0.44)]。
2.6 亚组分析结果
2.6.1 能量代谢类型对缺血预处理的效果 不同能量代谢特点(无氧、有氧运动)不是缺血预处理的调节因素,组间差异在统计学上不显著(P=0.87)。组内分析无论是无氧运动[ES=0.14,95%CI(0.04,0.23),P < 0.01]还是有氧运动[ES=0.13,95%CI(0.02,0.23),P=0.01],缺血预处理都能显著提高运动表现。
2.6.2 对照组对缺血预处理效果的影响 研究发现,不同对照组(假性缺血预处理和空白对照)会显著影响缺血预处理的运动表现(P=0.02),缺血预处理相对于空白对照(ESCON=0.22,95%CI (0.12,0.33),P < 0.01)的效果提升显著大于假性缺血预处理[ESSHAM=0.10,95%CI (0.02,0.18),P < 0.01]。
2.6.3 缺血与再灌注持续时间对缺血预处理的影响 组间差异显示缺血与再灌注持续时间可能是影响缺血预处理的调节因素(P=0.049),其中1×5 min[ES=0.60,95%CI(0.12,1.09),P=0.01]的方案显著大于其余所有方案。组内分析发现,仅3×5 min [ES=0.14,95%CI (0.03,0.26),P < 0.01] 以及4×5 min[ES=0.11,95%CI(0.00,0.21),P=0.02]的方案在统计学上显著。

2.6.4 运动经验水平对缺血预处理的影响 组间差异显示运动经验水平不是缺血预处理的调节因素(P > 0.05)。组内分析显示,仅运动经验水平低(0-2级)受试者在统计学上显著,运动水平较高(3-5级)的受试者均不显著,其效果分别为:水平0[ES=0.14,95%CI (-0.10,0.39),P=0.03]、水平1[ES=0.15,95%CI(0.03,0.27),P=0.02]、水平2[ES=0.19,95%CI(0.04,0.33),P=0.01]。
2.6.5 性别对缺血预处理的影响 组间比较显示性别不是缺血预处理干预效果的显著调节因素(P=0.25)。组内分析表明,仅男性受试者在缺血预处理后表现提升达到统计显著性[ES=0.20,95%CI (0.10,0.30),P < 0.01],而女性组未表现出明显效应。
2.7 回归分析结果 年龄对缺血预处理提升运动表现、无氧表现以及有氧表现的影响较小,该影响在统计上均不显著(P > 0.05)。回归系数β分别为0.000 9、0.001 7和0.003 1。
| [1] GIRARD O, AMANN M, AUGHEY R, et al. Position statement--altitude training for improving team-sport players’ performance: current knowledge and unresolved issues. Br J Sports Med. 2013;47 Suppl 1(Suppl 1):i8-16. [2] CARU M, LEVESQUE A, LALONDE F, et al. An overview of ischemic preconditioning in exercise performance: A systematic review. J Sport Health Sci. 2019;8(4): 355-369. [3] DAVIDS CJ, ROBERTS LA, BJØRNSEN T, et al. Where Does Blood Flow Restriction Fit in the Toolbox of Athletic Development? A Narrative Review of the Proposed Mechanisms and Potential Applications. Sports Med. 2023;53(11):2077-2093. [4] BLAZEVICH AJ, BABAULT N. Post-activation Potentiation Versus Post-activation Performance Enhancement in Humans: Historical Perspective, Underlying Mechanisms, and Current Issues. Front Physiol. 2019;10:1359. [5] CRISAFULLI A, TANGIANU F, TOCCO F, et al. Ischemic preconditioning of the muscle improves maximal exercise performance but not maximal oxygen uptake in humans. J Appl Physiol. 2011;111(2):530-536. [6] MURRY CE, JENNINGS RB, REIMER KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation. 1986;74(5):1124-1136. [7] MURRY CE, RICHARD VJ, REIMER KA, et al. Ischemic preconditioning slows energy metabolism and delays ultrastructural damage during a sustained ischemic episode. Circ Res. 1990;66(4):913-931. [8] REIMER KA, MURRY CE, JENNINGS RB. Cardiac adaptation to ischemia. Ischemic preconditioning increases myocardial tolerance to subsequent ischemic episodes. Circulation. 1990;82(6):2266-2268. [9] REIMER KA, MURRY CE, YAMASAWA I, et al. Four brief periods of myocardial ischemia cause no cumulative ATP loss or necrosis. Am J Physiol. 1986;251(6 Pt 2):H1306-1315. [10] DE GROOT PC, THIJSSEN DH, SANCHEZ M, et al. Ischemic preconditioning improves maximal performance in humans. Eur J Appl Physiol. 2010;108(1):141-146. [11] FERREIRA TN, SABINO-CARVALHO JL, LOPES TR, et al. Ischemic Preconditioning and Repeated Sprint Swimming: A Placebo and Nocebo Study. Med Sci Sports Exerc. 2016;48(10):1967-1975. [12] MAROCOLO M, DA MOTA GR, PELEGRINI V, et al. Are the Beneficial Effects of Ischemic Preconditioning on Performance Partly a Placebo Effect? Int J Sports Med. 2015;36(10):822-825. [13] CARVALHO L, BARROSO R. Ischemic Preconditioning Improves Strength Endurance Performance. J Strength Cond Res. 2019;33(12):3332-3337. [14] DA SILVA NOVAES J, DA SILVA TELLES LG, MONTEIRO ER, et al. Ischemic Preconditioning Improves Resistance Training Session Performance. J Strength Cond Res. 2021;35(11):2993-2998. [15] PETHICK J, CASSELTON C, WINTER SL, et al. Ischemic Preconditioning Blunts Loss of Knee Extensor Torque Complexity with Fatigue. Med Sci Sports Exerc. 2021; 53(2):306-315. [16] PEREIRA HM, DE LIMA FF, SILVA BM, et al. Sex differences in fatigability after ischemic preconditioning of non-exercising limbs. Biol Sex Differ. 2020;11(1):59. [17] BAILEY TG, BIRK GK, CABLE NT, et al. Remote ischemic preconditioning prevents reduction in brachial artery flow-mediated dilation after strenuous exercise. Am J Physiol Heart Circ Physiol. 2012;303(5):H533-538. [18] BAILEY TG, JONES H, GREGSON W, et al. Effect of Ischemic Preconditioning on Lactate Accumulation and Running Performance. Med Sci Sports Exerc. 2012; 44(11):2084-2089. [19] CHEUNG CP, SLYSZ JT, BURR JF. Ischemic Preconditioning: Improved Cycling Performance Despite Nocebo Expectation. Int J Sports Physiol Perform. 2020;15(3): 354-360. [20] CRUZ RS, DE AGUIAR RA, TURNES T, et al. Effects of ischemic preconditioning on maximal constant-load cycling performance. J Appl Physiol (1985). 2015;119(9):961-967. [21] PAULL EJ, VAN GUILDER GP. Remote ischemic preconditioning increases accumulated oxygen deficit in middle-distance runners. J Appl Physiol. 2019;126(5):1193-1203. [22] 苏玉莹,李卫.远程缺血预处理对运动表现的影响及其生理机制研究进展[J].中国体育科技,2024,60(10):31-39. [23] GIBSON N, WHITE J, NEISH M, et al. Effect of ischemic preconditioning on land-based sprinting in team-sport athletes. Int J Sports Physiol Perform. 2013;8(6):671-676. [24] JEAN-ST-MICHEL E, MANLHIOT C, LI J, et al. Remote preconditioning improves maximal performance in highly trained athletes. Med Sci Sports Exerc. 2011;43(7):1280-1286. [25] WILLIAMS N, RUSSELL M, COOK CJ, et al. Effect of Ischemic Preconditioning on Maximal Swimming Performance. J Strength Cond Res. 2021;35(1):221-226. [26] RICHARD P, BILLAUT F. Time-Trial Performance in Elite Speed Skaters After Remote Ischemic Preconditioning. Int J Sports Physiol Perform. 2018;13(10): 1308-1316. [27] LINDNER TD, SCHOLTEN SD, HALVERSON JM, et al. The Acute Effects of Ischemic Preconditioning on Power and Sprint Performance. S D Med. 2021;74(5):210-219. [28] NIESPODZINSKI B, MIESZKOWSKI J, KOCHANOWICZ M, et al. Effect of 10 consecutive days of remote ischemic preconditioning on local neuromuscular performance. J Electromyogr Kinesiol. 2021;60:102584. [29] DE SOUZA HLR, ARRIEL RA, MOTA GR, et al. Does ischemic preconditioning really improve performance or it is just a placebo effect? PLoS One. 2021;16(5):e0250572. [30] VALENZUELA PL, MARTÍN-CANDILEJO R, SÁNCHEZ-MARTÍNEZ G, et al. Ischemic Preconditioning and Muscle Force Capabilities. J Strength Cond Res. 2021; 35(8):2187-2192. [31] SLYSZ JT, BURR JF. Impact of 8 weeks of repeated ischemic preconditioning on running performance. Eur J Appl Physiol. 2019;119(6):1431-1437. [32] SEEGER JPH, TIMMERS S, PLOEGMAKERS DJM, et al. Is delayed ischemic preconditioning as effective on running performance during a 5km time trial as acute IPC? J Sci Med Sport. 2017;20(2):208-212. [33] PARADIS-DESCHÊNES P, LAPOINTE J, JOANISSE DR, et al. Similar Recovery of Maximal Cycling Performance after Ischemic Preconditioning, Neuromuscular Electrical Stimulation or Active Recovery in Endurance Athletes. J Sports Sci Med. 2020;19(4):761-771. [34] MIESZKOWSKI J, STANKIEWICZ B, KOCHANOWICZ A, et al. Effect of Ischemic Preconditioning on Marathon-Induced Changes in Serum Exerkine Levels and Inflammation. Front Physiol. 2020;11: 571220. [35] COCKING S, WILSON MG, NICHOLS D, et al. Is There an Optimal Ischemic-Preconditioning Dose to Improve Cycling Performance? Int J Sports Physiol Perform. 2018;13(3):274-282. [36] BEHRENS M, ZSCHORLICH V, MITTLMEIER T, et al. Ischemic Preconditioning Did Not Affect Central and Peripheral Factors of Performance Fatigability After Submaximal Isometric Exercise. Front Physiol. 2020; 11:371. [37] CLEVIDENCE MW, MOWERY RE, KUSHNICK MR. The effects of ischemic preconditioning on aerobic and anaerobic variables associated with submaximal cycling performance. Eur J Appl Physiol. 2012;112(10):3649-3654. [38] GOLDSMITH M, SIEGLER J, GREEN S. Targeted effect of ischemic preconditioning on the gas exchange threshold in healthy males and females. Eur J Appl Physiol. 2024;124(9):2697-2706. [39] KAUR G, BINGER M, EVANS C, et al. No influence of ischemic preconditioning on running economy. Eur J Appl Physiol. 2017;117(2):225-235. [40] SOUZA HLR, OLIVEIRA GT, MEIRELES A, et al. Does ischemic preconditioning enhance sports performance more than placebo or no intervention? A systematic review with meta-analysis. J Sport Health Sci. 2024;14:101010. [41] TEIXEIRA AL, GANGAT A, BOMMARITO JC, et al. Ischemic Preconditioning Acutely Improves Functional Sympatholysis during Handgrip Exercise in Healthy Males but not Females. Med Sci Sports Exerc. 2023;55(7):1250-1257. [42] PAGE MJ, MCKENZIE JE, BOSSUYT PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. [43] STERNE JAC, SAVOVIĆ J, PAGE MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366:l4898. [44] CUMPSTON M, LI T, PAGE MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019;2019(10):ED000142. [45] GASTIN PB. Energy system interaction and relative contribution during maximal exercise. Sports Med Auckl NZ. 2001;31(10):725-741. [46] INCOGNITO AV, BURR JF, MILLAR PJ. The Effects of Ischemic Preconditioning on Human Exercise Performance. Sports Med. 2016;46(4):531-544. [47] MCKAY AKA, STELLINGWERFF T, SMITH ES, et al. Defining Training and Performance Caliber: A Participant Classification Framework. Int J Sports Physiol Perform. 2021;17(2):317-331. [48] SLYSZ JT, PETRICK HL, MARROW JP, et al. An examination of individual responses to ischemic preconditioning and the effect of repeated ischemic preconditioning on cycling performance. Eur J Sport Sci. 2020;20(5):633-640. [49] HEDGES LV, OLKIN I. Statistical methods for meta-analysis. Pittsburgh:Academic Press. 2014. [50] VAN DEN NOORTGATE W, LÓPEZ-LÓPEZ JA, MARÍN-MARTÍNEZ F, et al. Three-level meta-analysis of dependent effect sizes. Behav Res Methods. 2013;45(2):576-594. [51] HEDGES LV, TIPTON E, JOHNSON MC. Robust variance estimation in meta-regression with dependent effect size estimates. Res Synth Methods. 2010;1(1):39-65. [52] CHEUNG MW. A Guide to Conducting a Meta-Analysis with Non-Independent Effect Sizes. Neuropsychol Rev. 2019;29(4):387-396. [53] FERNÁNDEZ-CASTILLA B, ALOE AM, DECLERCQ L, et al. Estimating outcome-specific effects in meta-analyses of multiple outcomes: A simulation study. Behav Res Methods. 2021;53(2):702-717. [54] JUKIC I, CASTILLA AP, RAMOS AG, et al. The Acute and Chronic Effects of Implementing Velocity Loss Thresholds During Resistance Training: A Systematic Review, Meta-Analysis, and Critical Evaluation of the Literature. Sports Med. 2023;53(1): 177-214. [55] VEMBYE MH, JAMES EP. Power approximations for overall average effects in meta-analysis with dependent effect sizes. J Educ Behav Stat. 2023;48(1):70-102. [56] TIPTON E, PUSTEJOVSKY JE. Small-Sample Adjustments for Tests of Moderators and Model Fit Using Robust Variance Estimation in Meta-Regression. J Educ Behav Stat. 2015;40(6):604-634. [57] VIECHTBAUER W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36:1-48. [58] PUSTEJOVSKY JE, TIPTON E. Meta-analysis with Robust Variance Estimation: Expanding the Range of Working Models. Prev Sci. 2022;23(3):425-438. [59] TURNES T, DE AGUIAR RA, DE OLIVEIRA CRUZ RS, et al. Impact of ischaemia-reperfusion cycles during ischaemic preconditioning on 2000-m rowing ergometer performance. Eur J Appl Physiol. 2018;118(8):1599-1607. [60] PARADIS-DESCHÊNES P, JOANISSE DR, MAURIÈGE P, et al. Ischemic Preconditioning Enhances Aerobic Adaptations to Sprint-Interval Training in Athletes Without Altering Systemic Hypoxic Signaling and Immune Function. Front Sports Act Living. 2020;2:41. [61] RICO-GONZÁLEZ M, PINO-ORTEGA J, CLEMENTE FM, et al. Guidelines for performing systematic reviews in sports science. Biol Sport. 2022;39(2):463-471. [62] PETERS JL, SUTTON AJ, JONES DR, et al. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J Clin Epidemiol. 2008;61(10):991-996. [63] EGGER M, DAVEY SMITH G, SCHNEIDER M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315(7109):629-634. [64] SCHÜNEMANN HJ, HIGGINS JPT, VIST GE, et al. Completing ‘Summary of findings’ tables and grading the certainty of the evidence//HIGGINS JPT, THOMAS J, CHANDLER J, et al. Cochrane Handbook for Systematic Reviews of Interventions. New York: John Wiley & Sons, Inc. 2019:375-402. [65] GUYATT G, OXMAN AD, AKL EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383-394. [66] SANTESSO N, CARRASCO-LABRA A, LANGENDAM M, et al. Improving GRADE evidence tables part 3: detailed guidance for explanatory footnotes supports creating and understanding GRADE certainty in the evidence judgments. J Clin Epidemiol. 2016;74:28-39. [67] ALBUQUERQUE MR, FLÔR CAG, RIBEIRO AIS, et al. Effects of Ischemic Preconditioning on Sport-Specific Performance in Highly Trained Taekwondo Athletes. Sports (Basel). 2024;12(7):179. [68] TELLES LGDS, BILLAUT F, CUNHA G, et al. Ischemic Preconditioning Improves Handgrip Strength and Functional Capacity in Active Elderly Women. Int J Environ Res Public Health. 2022;19(11):6628. [69] ALLOIS R, PAGLIARO P, ROATTA S. Ischemic Conditioning to Reduce Fatigue in Isometric Skeletal Muscle Contraction. Biology (Basel). 2023;12(3):460. [70] BARBOSA TC, MACHADO AC, BRAZ ID, et al. Remote ischemic preconditioning delays fatigue development during handgrip exercise. Scand J Med Sci Sports. 2015;25(3):356-364. [71] CARVALHO L, BARROSO R. Effects of ischemic preconditioning on the isometric test variables. Sci Sports. 2019;34(3): E225-E228. [72] CEYLAN B, FRANCHINI E. Ischemic preconditioning does not improve judo-specific performance but leads to better recovery in elite judo athletes. Sci Sports. 2022;37(4):322.e1-322.e7. [73] CEYLAN B, TAŞKIN HB, ŠIMENKO J. Effect of Ischemic Preconditioning on Acute Recovery in Elite Judo Athletes: A Randomized, Single-Blind, Crossover Trial. Int J Sports Physiol Perform. 2023;18(2):180-186. [74] CHENG CF, KUO YH, HSU WC, et al. Local and Remote Ischemic Preconditioning Improves Sprint Interval Exercise Performance in Team Sport Athletes. Int J Environ Res Public Health. 2021;18(20):10653. [75] CRUZ RS, DE AGUIAR RA, TURNES T, et al. Effects of ischemic preconditioning on short-duration cycling performance. Appl Physiol Nutr Metab. 2016;41(8):825-831. [76] CRUZ R, TRAMONTIN AF, OLIVEIRA AS, et al. Ischemic preconditioning increases spinal excitability and voluntary activation during maximal plantar flexion contractions in men. Scand J Med Sci Sports. 2024;34(3):e14591. [77] DANTAS PAM, DA SILVA NOVAES J, PAZ CR, et al. Acute effect of Ischemic Preconditioning in different blood flow restriction compressions on the anaerobic performance of trained individuals. Nuevas Tend EN Educ Fis Deporte Recreacion. 2024;(54):721-727. [78] DE SANTANA VJ, DE OLIVEIRA DEANGELO CE, CURY SALEMI VM, et al. The Influence of Ischemic Preconditioning on Neuromuscular Performance. Rev Bras Med Esporte. 2021; 27(2):207-211. [79] GAO X, WANG A, FAN J, et al. The effect of ischemic preconditioning on repeated sprint cycling performance: a randomized crossover study. J Sports Med Phys Fitness. 2024;64(11):1147-1156. [80] GIBSON N, MAHONY B, TRACEY C, et al. Effect of ischemic preconditioning on repeated sprint ability in team sport athletes. J Sports Sci. 2015;33(11):1182-1188. [81] GRIFFIN PJ, HUGHES L, GISSANE C, et al. Effects of local versus remote ischemic preconditioning on repeated sprint running performance. J Sports Med Phys Fitness. 2019;59(2):187-194. [82] GUILHERME DA SILVA TELLES L, CRISTIANO CARELLI L, DUTRA BRÁZ I, et al. Effects of Ischemic Preconditioning as a Warm-Up on Leg Press and Bench Press Performance. J Hum Kinet. 2020;75:267-277. [83] HUANG BH, WANG TY, LU KH, et al. Effects of ischemic preconditioning on local hemodynamics and isokinetic muscular function. Isokinet Exerc Sci. 2020;28(1):73-81. [84] KATAOKA R, SONG JS, YAMADA Y, et al. The Impact of Different Ischemic Preconditioning Pressures on Pain Sensitivity and Resistance Exercise Performance. J Strength Cond Res. 2024;38(5):864-872. [85] KRAUS AS, PASHA EP, MACHIN DR, et al. Bilateral upper limb remote ischemic preconditioning improves peak anaerobic power. Open Sports Med J. 2015;9:1-6. [86] LIM AT, LIM J, GIRARD O, et al. Effect of ischemic preconditioning on badminton-specific endurance and subsequent changes in physical performance. Sci Sports. 2023; 38(1):102.e1-102.e7. [87] LISBÔA FD, TURNES T, CRUZ RS, et al. The time dependence of the effect of ischemic preconditioning on successive sprint swimming performance. J Sci Med Sport. 2017;20(5):507-511. [88] LOPES TR, SABINO-CARVALHO JL, FERREIRA THN, et al. Effect of Ischemic Preconditioning on the Recovery of Cardiac Autonomic Control From Repeated Sprint Exercise. Front Physiol. 2018;9:1465. [89] MAROCOLO M, MAROCOLO IC, DA MOTA GR, et al. Beneficial Effects of Ischemic Preconditioning in Resistance Exercise Fade Over Time. Int J Sports Med. 2016; 37(10):819-824. [90] MAROCOLO M, WILLARDSON JM, MAROCOLO IC, et al. Ischemic Preconditioning and Placebo Intervention Improves Resistance Exercise Performance. J Strength Cond Res. 2016;30(5):1462-1469. [91] PAIXÃO RC, DA MOTA GR, MAROCOLO M. Acute effect of ischemic preconditioning is detrimental to anaerobic performance in cyclists. Int J Sports Med. 2014;35(11): 912-915. [92] PARADIS-DESCHÊNES P, JOANISSE DR, BILLAUT F. Ischemic preconditioning increases muscle perfusion, oxygen uptake, and force in strength-trained athletes. Appl Physiol Nutr Metab. 2016; 41(9):938-944. [93] PARADIS-DESCHÊNES P, JOANISSE DR, BILLAUT F. Sex-Specific Impact of Ischemic Preconditioning on Tissue Oxygenation and Maximal Concentric Force. Front Physiol. 2017;7:674. [94] PATTERSON SD, BEZODIS NE, GLAISTER M, et al. The Effect of Ischemic Preconditioning on Repeated Sprint Cycling Performance. Med Sci Sports Exerc. 2015;47(8):1652-1658. [95] RODRIGUES AL, IDE BN, SASAKI JE, et al. Ischemic Preconditioning Improves the Bench-Press Maximal Strength in Resistance-Trained Men. Int J Exerc Sci. 2023;16(4):217-229. [96] SALAGAS A, TSOUKOS A, TERZIS G, et al. Effectiveness of either short-duration ischemic pre-conditioning, single-set high-resistance exercise, or their combination in potentiating bench press exercise performance. Front Physiol. 2022;13: 1083299. [97] SLYSZ JT, BURR JF. Enhanced Metabolic Stress Augments Ischemic Preconditioning for Exercise Performance. Front Physiol. 2018;9:1621. [98] SUTTER EN, MATTLAGE AE, BLAND MD, et al. Remote Limb Ischemic Conditioning and Motor Learning: Evaluation of Factors Influencing Response in Older Adults. Transl Stroke Res. 2019;10(4):362-371. [99] TANAKA D, SUGA T, TANAKA T, et al. Ischemic Preconditioning Enhances Muscle Endurance during Sustained Isometric Exercise. Int J Sports Med. 2016;37(8): 614-618. [100] TELLES LG, BILLAUT F, DE SOUZA RIBEIRO A, et al. Ischemic Preconditioning with High and Low Pressure Enhances Maximum Strength and Modulates Heart Rate Variability. Int J Environ Res Public Health. 2022;19(13):7655. [101] THOMPSON KMA, WHINTON AK, FERTH S, et al. Ischemic Preconditioning: No Influence on Maximal Sprint Acceleration Performance. Int J Sports Physiol Perform. 2018;13(8):986-990. [102] VANGSOE MT, NIELSEN JK, PATON CD. A Comparison of Different Prerace Warm-Up Strategies on 1-km Cycling Time-Trial Performance. Int J Sports Physiol Perform. 2020;15(8):1109-1116. [103] CHRISTIANSEN D, OLSEN CBL, KEHLER F, et al. Active Relative to Passive Ischemic Preconditioning Enhances Intense Endurance Performance in Well-Trained Men. Int J Sports Physiol Perform. 2022; 17(6):979-990. [104] COCKING S, LANDMAN T, BENSON M, et al. The impact of remote ischemic preconditioning on cardiac biomarker and functional response to endurance exercise. Scand J Med Sci Sports. 2017;27(10):1061-1069. [105] FOSTER GP, WESTERDAHL DE, FOSTER LA, et al. Ischemic preconditioning of the lower extremity attenuates the normal hypoxic increase in pulmonary artery systolic pressure. Respir Physiol Neurobiol. 2011;179(2-3):248-253. [106] GRIFFIN PJ, FERGUSON RA, GISSANE C, et al. Ischemic preconditioning enhances critical power during a 3 minute all-out cycling test. J Sports Sci. 2018;36(9):1038-1043. [107] HALLEY SL, PEELING P, BROWN H, et al. Repeat Application of Ischemic Preconditioning Improves Maximal 1,000-m Kayak Ergometer Performance in a Simulated Competition Format. J Strength Cond Res. 2020. doi: 10.1519/JSC.0000000000003748. [108] HALLEY SL, MARSHALL P, SIEGLER JC. Effect of ischemic preconditioning and changing inspired O2 fractions on neuromuscular function during intense exercise. J Appl Physiol (1985). 2019;127(6):1688-1697. [109] HITTINGER EA, MAHER JL, NASH MS, et al. Ischemic preconditioning does not improve peak exercise capacity at sea level or simulated high altitude in trained male cyclists. Appl Physiol Nutr Metab. 2015;40(1):65-71. [110] JESSEN S, ZEUTHEN M, SOMMER JEPPESEN J, et al. Active ischemic pre-conditioning does not additively improve short-term high-intensity cycling performance when combined with caffeine ingestion in trained young men. Eur J Sport Sci. 2024;24(6):693-702. [111] KIDO K, SUGA T, TANAKA D, et al. Ischemic preconditioning accelerates muscle deoxygenation dynamics and enhances exercise endurance during the work-to-work test. Physiol Rep. 2015;3(5):e12395. [112] KIDO K, SUGA T, TANAKA D, et al. Remote ischemic preconditioning accelerates systemic O2 dynamics and enhances endurance during work-to-work cycling exercise. Transl Sports Med. 2018;1(5):204-211. [113] KILDING AE, SEQUEIRA GM, WOOD MR. Effects of ischemic preconditioning on economy, VO2 kinetics and cycling performance in endurance athletes. Eur J Appl Physiol. 2018;118(12):2541-2549. [114] KJELD T, RASMUSSEN MR, JATTU T, et al. Ischemic preconditioning of one forearm enhances static and dynamic apnea. Med Sci Sports Exerc. 2014;46(1):151-155. [115] MACDOUGALL KB, MCCLEAN ZJ, MACINTOSH BR, et al. Ischemic Preconditioning, But Not Priming Exercise, Improves Exercise Performance in Trained Rock Climbers. J Strength Cond Res. 2023; 37(11):2149-2157. [116] MONTOYE AHK, MITCHINSON CJ, TOWNSEND OR, et al. Ischemic Preconditioning Does Not Improve Time Trial Performance in Recreational Runners. Int J Exerc Sci. 2020;13(6):1402-1417. [117] MORLEY WN, MURRANT CL, BURR JF. Ergogenic effect of ischemic preconditioning is not directly conferred to isolated skeletal muscle via blood. Eur J Appl Physiol. 2023; 123(8):1851-1861. [118] MOTA GR, RIGHTMIRE ZB, MARTIN JS, et al. Ischemic preconditioning has no effect on maximal arm cycling exercise in women. Eur J Appl Physiol. 2020;120(2):369-380. [119] MUÑOZ-GÓMEZ E, MOLLÀ-CASANOVA S, SEMPERE-RUBIO N, et al. Potential Benefits of a Single Session of Remote Ischemic Preconditioning and Walking in Sedentary Older Adults: A Pilot Study. Int J Environ Res Public Health. 2023;20(4):3515. [120] PANDORF Z, ERICKSON S, SCHOLTEN SD. Ischemic Preconditioning On Swimming Performance: An Exploration Into Practical Application. Med Sci Sports Exerc. 2023; 55(9):377. [121] SABINO-CARVALHO JL, LOPES TR, OBEID-FREITAS T, et al. Effect of Ischemic Preconditioning on Endurance Performance Does Not Surpass Placebo. Med Sci Sports Exerc. 2017;49(1):124-132. [122] TANAKA D, SUGA T, KIDO K, et al. Acute remote ischemic preconditioning has no effect on quadriceps muscle endurance. Transl Sports Med. 2020;3(4):314-320. [123] TER BEEK F, JOKUMSEN PS, SLOTH BN, et al. Ischemic Preconditioning Attenuates Rating of Perceived Exertion But Does Not Improve Maximal Oxygen Consumption or Maximal Power Output. J Strength Cond Res. 2022;36(9):2479-2485. [124] TOCCO F, MARONGIU E, GHIANI G, et al. Muscle ischemic preconditioning does not improve performance during self-paced exercise. Int J Sports Med. 2015;36(1):9-15. [125] TOMSCHI F, NIEMANN D, BLOCH W, et al. Ischemic Preconditioning Enhances Performance and Erythrocyte Deformability of Responders. Int J Sports Med. 2018; 39(8):596-603. [126] URBANSKI R, ASCHENBRENNER P, ZMIJEWSKI P, et al. Effect of Simultaneous Lower- and Upper-Body Ischemic Preconditioning on Lactate, Heart Rate, and Rowing Performance in Healthy Males and Females. Applied Sciences. 2024;14(9):3539. [127] WIGGINS CC, CONSTANTINI K, PARIS HL, et al. Ischemic Preconditioning, O2 Kinetics, and Performance in Normoxia and Hypoxia. Med Sci Sports Exerc. 2019;51(5):900-911. [128] ZHONG Z, DONG H, WU Y, et al. Remote ischemic preconditioning enhances aerobic performance by accelerating regional oxygenation and improving cardiac function during acute hypobaric hypoxia exposure. Front Physiol. 2022;13:950086. [129] 范紫菡,吴迎.缺血处理在运动训练中的应用:效果、机制及问题[J].中国运动医学杂志,2024,43(9):753-766. [130] CHEN Z, WU W, QIANG L, et al. The effect of ischemic preconditioning on physical fitness and performance: a meta-analysis in healthy adults. Eur J Appl Physiol. 2025;125(3):805-821. [131] 徐恺,殷明越,王然.中文体育类核心期刊元分析的选题和方法学问题[J].体育科学,2024,44(1):88-97. [132] PANG CY, YANG RZ, ZHONG A, et al. Acute ischaemic preconditioning protects against skeletal muscle infarction in the pig. Cardiovasc Res. 1995;29(6):782-788. [133] SCHULZ R, POST H, VAHLHAUS C, et al. Ischemic preconditioning in pigs: a graded phenomenon: its relation to adenosine and bradykinin. Circulation. 1998;98(10):1022-1029. [134] MAROCOLO M, HOHL R, ARRIEL RA, et al. Ischemic preconditioning and exercise performance: are the psychophysiological responses underestimated? Eur J Appl Physiol. 2023;123(4):683-693. [135] SANTOS CERQUEIRA M, KOVACS D, MARTINS DE FRANÇA I, et al. Effects of Individualized Ischemic Preconditioning on Protection Against Eccentric Exercise-Induced Muscle Damage: A Randomized Controlled Trial. Sports Health. 2021; 13(6):554-564. [136] MARCORA SM, STAIANO W, MANNING V. Mental fatigue impairs physical performance in humans. J Appl Physiol (1985). 2009;106(3):857-864. [137] OKANO AH, FONTES EB, MONTENEGRO RA, et al. Brain stimulation modulates the autonomic nervous system, rating of perceived exertion and performance during maximal exercise. Br J Sports Med. 2015;49(18):1213-1218. [138] MEIRELES A, SOUZA HLR, ARRIEL RA, et al. Attenuation of Neuromuscular Fatigue by Ischemic Preconditioning with Moderate Cuff Pressure is Not Related to Muscle Oxygen Saturation in Men. Int J Exerc Sci. 2023;16(2):1025-1037. [139] HERROD PJJ, LUND JN, PHILLIPS BE. Time-efficient physical activity interventions to reduce blood pressure in older adults: a randomised controlled trial. Age Ageing. 2021;50(3):980-984. [140] ZHANG Y, KONG H, XU K, et al. Comment on “Does ischemic preconditioning enhance sports performance more than placebo or no intervention? A systematic review with meta-analysis”. J Sport Health Sci. 2025;14:101056. |
| [1] | 冯 强, 皮亦华, 黄华生, 黄德伦, 张 艳. 骨髓间充质干细胞移植治疗大鼠心肌梗死:急性和慢性运动的影响[J]. 中国组织工程研究, 2025, 29(23): 4868-4877. |
| [2] | 付常喜, 何瑞波, 马 刚, 朱 政, 马文超 .
不同运动模式影响心肌梗死致心力衰竭大鼠骨骼肌重塑的机制
[J]. 中国组织工程研究, 2025, 29(2): 221-230. |
| [3] | 孙玉马, 马文超, 付常喜. 粒细胞集落刺激因子联合高强度间歇运动预处理改善急性心肌梗死大鼠心脏重塑[J]. 中国组织工程研究, 2024, 28(31): 4987-4994. |
| [4] | 徐文杰, 谢旭东, 何瑞波, 马 刚, 彭 朋. 补充血管紧张素(1-7)联合运动疗法对肾性高血压大鼠心脏重塑的作用与机制[J]. 中国组织工程研究, 2024, 28(26): 4137-4144. |
| [5] | 张 敏, 娄 国, 付常喜. 有氧运动预适应改善骨髓间充质干细胞治疗急性心肌梗死的效果[J]. 中国组织工程研究, 2024, 28(25): 3988-3993. |
| [6] | 杨梦晓, 付常喜. 力量训练改善去卵巢模型大鼠骨损伤的作用机制[J]. 中国组织工程研究, 2024, 28(20): 3150-3156. |
| [7] | 刘 芃, 马 刚, 何瑞波, 彭 朋. 有氧运动干预慢性肾功能衰竭模型大鼠的肾脏纤维化[J]. 中国组织工程研究, 2023, 27(20): 3209-3215. |
| [8] | 陈子扬, 蒲 锐, 邓 爽, 袁凌燕. 外泌体对运动介导胰岛素抵抗类疾病的调控作用[J]. 中国组织工程研究, 2021, 25(25): 4089-4094. |
| [9] | 申晋波, 张 林. 急性力竭运动导致大鼠跟腱微损伤的超微结构变化及机制[J]. 中国组织工程研究, 2021, 25(8): 1190-1195. |
| [10] | 袁国强, 秦永生, 彭 朋. 高强度间歇运动对自发性高血压模型大鼠病理性心脏肥大的影响及机制[J]. 中国组织工程研究, 2020, 24(23): 3708-3715. |
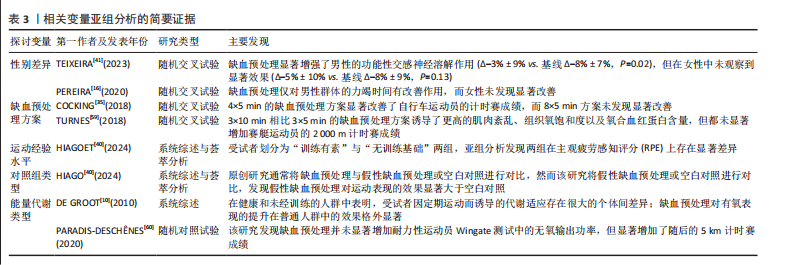
研究发现在增量自行车运动测试之前进行缺血预处理可将最大摄氧量提高3%,输出功率提高1.6%[10]。缺血预处理能有效提高无氧表现,例如短距离游泳成绩[11-12]、高负荷阻力运动的重复次数[13-14]、力竭测试表现等[15-16]。在有氧表现方面,缺血预处理可提升5 km跑步和自行车计时赛成绩[17-19],延长增量测试和高强度力竭测试的时间[5,19-21]、提高摄氧量[20-21],其增益效果的生理机制尚不明确,但通过苏玉莹等[22]最新的研究可发现,缺血预处理的内源性保护机制可能引发心血管系统、呼吸系统、神经系统、感知系统、代谢反应和恢复系统产生一系列生理变化,如增强心脏泵血能力、改善血液循环、提升氧气输送效率、降低主观疲劳感、促进代谢产物清除和加强神经肌肉募集等,从而有助于运动表现的提升。
然而,当前研究结果的分歧仍是该领域面临的持续挑战,现存大量文献证明缺血预处理并不能有效提高运动表现,例如在无氧表现方面,有研究发现缺血预处理后的冲刺和计时赛成绩[23-26]、跳跃能力[27]、最大自主收缩能力[28-29]、一次最大重复没有明显提升[30];在有氧表现方面,计时赛成绩[31-35]、力竭测试表现[36-37]、最大摄氧量也没有显著提升[31,38-39]。因此,缺血预处理对运动表现是否有效仍是一个亟待解决的问题。而出现这一争议的原因之一是原创研究在方法学上的显著异质性,例如是否设置安慰剂对照组、是否包含热身环节、缺血与再灌注的具体参数(如持续时间)等,这些因素可能对缺血预处理的效果产生显著影响。有研究发现安慰剂效应的存在可能高估缺血预处理的真实效果[40];假性缺血预处理(例如气囊施加20 mmHg)的压力可能会产生安慰剂反应,尽管这种处理方式应该没有任何效应,但研究发现其效果与真实缺血预处理所产生的表现提升效果类似,这表明心理因素可能对结果有所贡献[40]。因此,进一步探索潜在的安慰剂效应变得至关重要。不仅如此,人口统计学因素(如性别、年龄等)也可能对缺血预处理的效果产生重要影响[16,41]。然而,目前针对这些因素的研究仍较为有限,亟需通过荟萃分析加以系统评估。
缺血预处理作为一种潜在的运动表现提升策略,可能为普通人群和运动员提供一个更加高效省时的急性表现提升方法。该研究旨在荟萃分析缺血预处理对运动表现的提升效果,并探讨受试者特征和缺血预处理方案等变量对主效应合并的调节效应。
中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
1.1 协议注册 此系统综述和荟萃分析遵循《系统综述与元分析优先报告条目》(PRISMA)2020指南[42]。研究已在PROSPERO平台注册(注册号:CRD42024614265)。
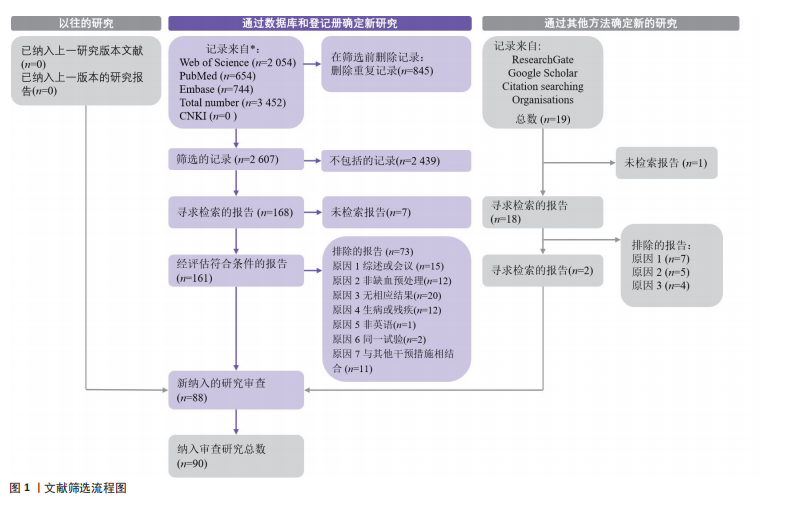
1.2 检索策略 在正式检索之前,其中1位作者(张益林)进行了简略检索。由2位独立评审员(徐恺和殷明越)在PubMed(MEDLINE)、Web of Science和EMBASE数据库中进行了系统文献检索,检索截止日期为2024-09-04。检索词是数据库特定的MeSH术语和关键词的组合:“remote ischemic preconditioning” OR “remote ischaemic preconditioning” OR “remote preconditioning” OR “remote conditioning” OR “remote ischemic conditioning” OR “remote ischaemic conditioning” OR “transient limb ischemia” OR “muscle ischemia” OR “ischemic preconditioning” AND “performance” OR “sport*” OR “exercise” OR “strength training” OR “running” OR “swimming” OR “cycling” OR “athletes” OR “sports performance”。在不同数据库中,尽可能添加了人类过滤器(各数据库的详细检索词见表1)。此外,所有已识别研究的参考文献列表均经过手动扫描以寻找其他研究。
1.3 研究选择与合格标准 1位作者(张益林)负责文献的识别和筛选,在合格性评估阶段,2位作者(徐恺和殷明越)根据排除和纳入标准对全文进行审查。若个别情况下无法确定某研究是否应被排除,将与第3位作者(孔昊)协商后作出决定。所有流程均使用Zotero文献管理软件完成。纳入文章的合格标准根据“PICOS”(参与者:Participants,P;干预措施: Intervention,I;对照组:Comparison,C;结果:Outcome,O;研究类型:Study,S)原则在表2中列出。
1.4 偏倚风险评估 采用Cochrane偏倚风险评估工具2(RoB 2)对符合纳入标准的研究进行偏倚风险评估[43]。该工具评估5个领域:①随机化过程;②偏离预期干预(分配效应和依从性);③缺失结果数据;④结果测量;⑤报告结果的选择。每个领域的评估结果分为“是”“可能是”“可能否”或“否”。根据Cochrane指南,偏倚风险被分类为“高”(至少1个领域存在高偏倚风险)、“存在一些担忧”(至少1个领域存在一些担忧但无高偏倚风险)或“低”(所有领域均为低偏倚风险)[44]。每项研究的总体风险被分类为“高”“存在一些担忧”和“低”的领域数量决定[44]。2位评审员独立评估每项研究的各个领域及总体偏倚风险,如有分歧则由第3位评审员进行裁决。
1.5 数据提取与整理 从纳入的研究中细致提取了多种特征,包括参与者的性别、年龄、运动经验水平、缺血预处理循环次数及其持续时间、肢体部位以及与缺血预处理、假性缺血预处理或无缺血相关的结果指标数据。
根据运动持续时间(75 s)[45-46],


将纳入的研究分为无氧运动和有氧运动。在运动经验水平方面,最初尝试将参与者按照中国运动员等级标准划分,然而发现国际上绝大部分有关缺血预处理的原创研究并未提及参与者的运动成绩,而是描述他们的运动经验年限或者参加什么级别的比赛。因此将参与者的运动经验水平根据MCKAY等[47]的标准分为6个等级(0-5):久坐不动者、休闲活动者、发展或训练中者、高度训练或国家级运动员、精英或国际级运动员,以及世界级运动员。
参与者的年龄基于原始纳入研究提供的平均值进行分析。如果原始研究提供了年龄范围(例如18-35岁),则使用中位数;如果原始研究分别为缺血预处理组、假性缺血预处理组或空白对照组提供了单独的年龄,则通过将各组所有年龄相加并除以样本量来计算平均年龄。在数据提取过程中,如果遇到不完整的数据,通过电子邮件联系作者以获取完整数据集,例如当仅提供事后比较而未提供具体的测试前后数据时。此外,对于以图形形式呈现数据的研究,使用数据提取工具(WebPlotDigitizer-Copyright 2010-2024 Ankit Rohatgi)提取数据。在比较缺血预处理干预次数时(例如,测试前48 h干预1次、测试前24 h干预1次、测试前15 min干预1次,结果为3次缺血预处理干预 vs. 2次干预 vs. 1次干预 vs. 假性缺血预处理组或空白对照组),仅提取测试前15 min的干预(1次干预)数据,并与空白对照组或假性缺血预处理组数据进行比较[48]。
在提取计时试验数据时,部分研究提供了计时试验的总距离和速度。因此,使用公式“时间=距离/速度”计算时间。此外,数据以缺血预处理响应者和非响应者形式呈现,或以每位参与者个体数据而非整体组数据形式提供时,提取每位参与者的数据并重新计算平均值和标准差[44]。
1.6 数据分析
1.6.1 数据综合与效应量计算 在纳入的研究中,存在2种比较形式:
(1)组间后测比较:指缺血预处理组、空白对照组和假性缺血预处理组缺乏前测数据,仅直接比较后测结果(缺血预处理组 vs. 空白对照组,缺血预处理组 vs. 假性缺血预处理组);
(2)前后测变化值比较:指缺血预处理组、空白对照组和假性缺血预处理组同时具备前测和后测数据,计算各组的变化值后再比较组间变化幅度的差异。
为了建立统一的分析框架,对于第一种缺乏前测数据时,将其前测值设定为基线状态(均值=0,标准差=0),随后通过变化值进行组间差异比较。此外,作为敏感性分析,建立了仅使用后测数据的比较模型,以验证研究结论的稳健性。以下公式用于计算变化值和效应量(effect size,ES):


其中,Mpost 和 Mpre 分别表示 缺血预处理组、空白对照组和假性缺血预处理组的前测和后测表现的均值;SDpre和 SDpost 分别表示缺血预处理组、空白对照组和假性缺血预处理组的前测和后测表现的标准差,n1 和n2 分别表示缺血预处理组、空白对照组和假性缺血预处理组的前测和后测样本量;SDpooled是测量值的合并标准
差[49]。前后测相关系数 r设定为0.6,随后在0.5-0.9范围内进行敏感性分析。效应量使用经过小样本调整后的estimate。
当报告标准误(SE)时,使用公式计算标准差。效应量值分类为小(< 0.2)、中(0.2-0.49)和大(0.5-0.8)。异质性通过 I2、τ2 和 Q 检验进行评估,其中 I2 为 25%、50% 和 75%分别表示低、中和高异质性。Q检验在 P < 0.1时被认为显著。这些指标代表了剩余异质性的相对和绝对值,表明未解释的变异性中归因于剩余异质性的部分。计算预测区间以更好地考虑未来类似研究的潜在变异性。
1.6.2 多层次meta分析 鉴于纳入的缺血预处理研究中存在多组别和多效应量的特点,此研究采用多层次混合效应模型进行荟萃分析[50-53]。具体而言,模型将组间、组内以及对照组(缺血预处理 vs. 空白对照组,缺血预处理 vs. 假性缺血预处理组)效应量作为显式嵌套的随机截距(即组内效应量嵌套于比较中,比较嵌套于研究中)。随后,将该模型的拟合优度与传统的两层级和三层级模型进行比较,并根据赤池信息准则(AIC)和贝叶斯信息准则(BIC)确定最终模型[54]。效应量通过逆采样方差加权,以考虑层级内、对照组-研究组和研究组间的
方差[55]。
此研究采用聚类稳健方差估计方法[51],并进行小样本调整[56],以考虑研究内效应量之间的相关性。最初将研究内的相关性设置为0.6,对相关性0.4和0.8进行敏感性分析,元分析结果无差异。模型参数使用受限最大似然法进行估计。单个系数及其对应的置信区间(confidence interval,CI)通过t分布进行检验[54]。所有多层次元分析均使用R语言(版本4.3.0;R核心团队,维也纳,奥地利)中的metafor包进行[57],而聚类稳健方差估计和小样本调整方法则通过clubSandwich
包实现[58]。
1.6.3 亚组分析与元回归分析 亚组与回归分析用来探索异质性来源与影响因素。此研究对多个二分类调节变量进行了亚组分析,包括能量代谢特点、性别、对照组类型、参与者的训练经验以及缺血预处理组数,以探讨这些因素对缺血预处理效果的潜在影响。有关上述5个变量进行亚组分析的简要依据在表3中查阅[10,16,35,40-41,59-60]。
为了确定连续型变量是否对缺血预处理有潜在影响,此研究对年龄进行回归分析。回归分析基于混合效应模型,使用受限最大似然估计进行计算,与传统最大似然估计相比,其在估计随机效应时考虑了固定效应的存在,因此通常被认为更加稳健[61]。在评估回归预测关系时,分别拟合、比较了线性与非线性三次函数,并选择模型拟合优度最佳的模型[61]。
1.6.4 发表偏倚与证据质量评估 发表偏倚风险通过漏斗图结合Egger检验进行评估[62-63],其中P > 0.05表示不存在发表偏倚风险。
科学证据的质量根据GRADE手册的建议进行评估[64]。使用GRADEpro
GDT软件将证据质量评级为高、中、低或极低。缺血预处理干预对运动表现改善的证据质量根据偏倚风险、结果不一致性、证据间接性、结果不精确性和发表偏倚进行评估[65-66]。最初,证据被视为高质量,但根据以下标准进行降级[65-66]:①研究中的偏倚风险:存在一些担忧时降1级,高风险时降2级;②间接性:如果存在间接性(例如,人群、干预措施、对照和结果不一致)降1级,如果间接性源于多种来源则降2级;③发表偏倚:如果怀疑存在发表偏倚(Egger检验和原始描述)降1级;④不一致性:当研究间异质性(I2)较高(> 50%)或置信区间重叠较差时降1级;⑤不精确性:当比较的样本量< 800名参与者或效应无明确方向(P > 0.05)时降1级。如果同时满足不精确性的2个标准,则证据质量降2级。评估过程由第一作者与第二作者独立完成。
3.2 缺血预处理对运动表现的影响 相比于不添加缺血预处理的运动,无论是无氧运动还是有氧运动前添加缺血预处理可有效提高运动表现[ES=0.13,95%CI (0.06,0.21),P < 0.01]。这一发现通过严格的统计学方法量化了范紫菡等[129]的综述观点,即他们认为缺血预处理对提升有氧能力、力量耐力、无氧耐力存在积极效应。不仅如此,在苏玉莹等[22]的研究中,他们发现缺血预处理对运动表现的急性影响一直以来饱受争议,即部分原创研究支持缺血预处理能够提高运动表现,而部分文献反之。然而,此研究通过综合90项原创研究的效应发现缺血预处理的确能够显著提高运动表现,尽管该效果较小。未来如果能够进一步优化下文所探讨的一些相关变量,缺血预处理有望成为体育科学领域的一个急性“兴奋剂”以优化人们的运动表现。
此外,研究结果也进一步支持了先前CHEN等[130]的荟萃分析,他们发现缺血预处理可以作为一种增强运动表现的方法,特别是对于主要由有氧系统和糖酵解提供动力的运动。然而CHEN等[130]的研究样本较少(27篇文章),且该荟萃分析仅仅是做了实验后测的差异对比(非前后差异),并且各项效应之间出现较大的权重差异[131]。而此研究克服了CHEN等[130]的一些研究局限,即从90项研究中提取干预前后的差异值以精准计算缺血预处理对运动表现提升的效应。不仅如此,CARU等[2]的研究表明,缺血预处理方案参数由于其异质性较大无法进行荟萃分析(I2=73.47%),因此他们仅仅做了系统综述评价,而此研究通过多层次荟萃分析方法克服了研究内和研究间的异质性。与此研究相似的研究结果在INCOGNITO等[46]的系统综述(非荟萃分析)中也发现,即缺血预处理的确会提高运动表现,但是仅仅涉及到67%的参与者,并且他们发现小样本和研究间的异质性会影响到数据的结果。相比之下,此研究纳入90篇文献,涉及1 439名受试者,通过三、四层次荟萃方法排除异质性(I2-Level 3=9.13%,I2-Level I2-Level 4=5.74%),发现缺血预处理提升运动表现的效应量很低,其异质性来源主要是因为对照组差异。具体而言,异质性主要是因为安慰剂效应会显著影响缺血预处理的效果(下文将详细讨论)。因此,应该谨慎看待缺血预处理对运动表现的真实效应,尤其是考虑到荟萃分析研究间的异质性以及原创实验的对照组差异。
3.3 能量代谢特点 关于缺血预处理的能量代谢特点,该研究主要围绕两个核心问题展开,并成功解决了当前研究领域的两点争议:
(1)缺血预处理能否提升无氧表现和有氧表现?此研究发现,缺血预处理既能提升无氧表现,也能提升有氧表现。在无氧表现方面,多项原创实验研究表明,缺血预处理能够显著提高短时间游泳成绩[11-12]、高负荷阻力运动的重复次数[13-14]、力竭测试表现等[15-16]。在有氧表现方面,缺血预处理也被证实能够提升5 km跑步和自行车计时赛成绩[15,17-18],延长增量测试的力竭时间[5,19-20],并提高高强度力竭测试的持续时间以及最大摄氧量[20-21]。然而,也有大量研究发现缺血预处理对运动表现的提升效果并不显著。例如,在无氧表现方面,部分研究显示缺血预处理未能显著改善冲刺能力[23-24]、计时赛成绩[25-26]、跳跃能力[27]、最大自主收缩能力以及1次最大重复(1RM)[28-30]。在有氧表现方面,也有研究指出缺血预处理对计时赛成绩[31-35]、力竭时间[36-37]、摄氧量等指标无显著影响[31,38-39]。尽管如此,通过严格的荟萃分析,此研究证实了缺血预处理对无氧表现和有氧表现的提升效果均具有统计学意义(P < 0.01),表明缺血预处理在整体上对两类运动表现均具有积极作用。
(2)缺血预处理对有氧表现和无氧表现的效果是否存在差异?此研究发现,缺血预处理对无氧表现和有氧表现的提升效果相当,这一结果与CARU等[2]的研究存在一定矛盾。他们认为,缺血预处理不考虑运动经验水平的情况下对有氧表现的提升效果似乎优于无氧表现[2],但有研究发现这可能是因为运动员的最大摄氧量已接近遗传潜能值,难以通过缺血预处理进一步显著提升[130]。然而,此研究通过综合分析发现,缺血预处理对无氧和有氧表现的效果并无显著差异。正如下文所讨论的,即缺血预处理仅仅在运动水平较低的受试者中才发现显著的提升效果,尽管组间无显著差异,但是这也表明,在这样的运动经验水平分组下可能存在普通人群效果更好的趋势。
缺血预处理的现有机制研究可能解释了为何它对无氧和有氧表现的效果相当。研究表明,缺血预处理能够显著减缓三磷酸腺苷的消耗,并在再灌注阶段通过增加血流清除缺血期间积累的有害代谢产物(如乳酸、氢离子、氨等)[6-7],这可能是缺血预处理提升无氧表现的关键机制。同时,缺血预处理还能减少葡萄糖-1-磷酸、葡萄糖-6-磷酸和乳酸的积累,从而降低运动的代谢压力,提高缺血耐受性,进而增强有氧能力[7-8]。总体而言,缺血预处理的核心作用在于减缓能量代谢速率,有效阻止进一步的能量损失,从而提高能量利用效率并维持代谢稳态[7-8]。缺血预处理独特的代谢调节机制似乎并没有说明其生理效应更加偏向于无氧代谢或者有氧代谢。而在运动科学领域中,通常需要研究不同运动项目的无氧或有氧代谢的临界点,很显然,当前的缺血预处理能量代谢机制并没有完全解释这一观点。因此,以上证据可能部分解释了为什么缺血预处理能够同时提升无氧和有氧表现,且效果相当。
3.4 缺血与再灌注时间方案 组间分析表明,缺血预处理方案可能是影响其提升运动表现效果的一个重要因素。具体而言,此研究发现3×5 min与4×5 min的缺血预处理方案能够有效提高运动表现。此外,1×5 min方案的效果显著优于其他所有方案,但这一结果需要谨慎解读,因为支持1×5 min方案的研究仅有1篇且样本量有限,可能存在偶然性。尽管有研究表明,较长的缺血再灌注周期(如3×10 min)在动物实验中能够产生显著的心脏保护作用并引起更高的肌肉紊乱[132-133],但在人体研究中并未观察到类似优势。例如,在2 000 m计时赛划船实验中,3×10 min方案在提升运动成绩方面并未显著优于3×5 min方案[59]。此外,COCKING等[35]的研究发现,8×5 min方案相较于4×5 min方案在改善自行车计时赛成绩方面也未表现出额外优势。
值得注意的是,目前尚缺乏较短时间缺血预处理方案(如1×5 min)与3×5 min或4×5 min方案的直接对比研究。然而,有研究表明,较短的缺血预处理方案(如1×5 min)可能不足以诱导显著的生理适应[126]。这一观点在此研究的亚组分析中得到了进一步支持(图4),其中3×2 min和5×2 min方案均未显著提高运动表现(P > 0.05)。综合现有证据,此研究认为3×5 min与4×5 min的缺血预处理方案可能是提升运动表现的有效选择,这些方案在提供足够刺激以诱导生理适应的同时,避免了过长时间可能带来的负面影响。
3.5 缺血预处理与安慰剂 此研究的一个关键发现是缺血预处理对运动表现的效果会受到安慰剂的显著影响。这一发现表明缺血预处理提升运动表现的机制可能并不来源于缺血预处理本身,而更多来源于受试者的心理作用。更令人意外的是,从心理指标变化到运动表现提升这样的缺血预处理机制已经被一些科学文献所证明。例如,MAROCOLO等[134]发现,无论是真实的缺血预处理还是安慰剂(无论施加20 mmHg还是220 mmHg),缺血的压力都会引起触觉感知,随后通过刺激皮下低阈值机械感受器(如帕西尼小体、迈斯纳小体、默克尔盘和鲁菲尼末梢)来调节神经处理,从而可能激发受试者的积极预期,进而提升整体表现。不仅如此,最新的荟萃分析仅仅对比了假性缺血预处理组与空白对照组的效应量,发现假性缺血预处理的运动表提升效果显著高于空白对照[40]。这与此研究结果完全吻合,即缺血预处理 vs. 空白对照的效果显著大于缺血预处理 vs. 假性缺血预处理(图4)。除此之外,DE SOUZA等[29]在一项缺血预处理对阻力运动影响的研究中发现,缺血预处理未能带来额外的效果增益,其主要原因也似乎是安慰剂效应。同样,SANTOS CERQUEIRA等[135]在针对个体化缺血预处理对防止偏心运动引起肌肉损伤的影响研究中,发现缺血预处理的效果也可能受到安慰剂的影响。
在此荟萃分析中,缺血预处理相对于空白对照和假性缺血预处理的合并效应量为0.13,虽然具有统计学意义,但考虑到假性缺血预处理相较于空白对照本身也呈现出显著的正向效应(图4所示),该效应量可能在很大程度上受到了安慰剂的放大作用。因此,这一结果提示:缺血预处理干预本身的“真实效应”可能小于当前观测到的总效应值,但在排除心理因素的前提下,其缺血预处理本身的生理效应仍难以确定。
尽管上述证据表明缺血预处理的确存在安慰剂效应,但此研究认为缺血预处理对运动表现的提升可能并不完全来自于安慰剂效应,其他一些因素也可能在一定程度上影响到该效应量。在排除本身的生理机制外,此研究发现在所纳入的90篇文献中,有70篇文献在缺血预处理后添加了热身,然而有20篇文献并没有添加热身,并且热身的强度不一。除此之外,缺血预处理到测试的间隔时间也有较大差异,分布在缺血预处理后即刻到12 h的广泛水平。因此,不管是最新的荟萃分析还是此研究的结果[40],虽然都发现安慰剂效应,但都没有考虑到缺血预处理的间隔时间以及热身程序这两大因素,然而热身能够有效提高运动表现在体育科学领域已经达成共识。因此,尽管缺血预处理存在安慰剂效应,但仍不能忽略本身的生理机制以及与其他混杂因素的影响。未来的研究应该更多的在控制安慰剂的情况下探讨缺血预处理本身的生理机制以及有无热身对缺血预处理的影响,尤其在严格控制热身的情况下探讨不同间隔时间对缺血预处理的效果差异及生理机制。
3.6 运动经验水平 在此研究的亚组分析中,缺血预处理对运动水平较低(0-2级)的个体展现出显著效应,而对训练水平较高(3-5级)者则无显著影响。然而,进一步的组间比较并未显示出统计意义上的差异。此种“组内显著而组间不显著”的现象,可能源于多重因素。从统计学角度而言,亚组内部的效应量虽具显著性,但两组之间效应量之差可能不足以超出显著性检验的置信门槛(例如ΔES较小,置信区间较宽),尤其在研究数量有限和异质性较高的前提下,组间比较的统计功效可能进一步受限。此外,该研究显示缺血预处理对运动表现的效应量仅为0.13,属于较低效应。因此,缺血预处理的总体干预效果有限,压缩了组间差异的上限,进而不利于识别统计学上的显著变化。
尽管组间无显著差异,但组内分析表明,运动水平较低(0-2级)的受试者在缺血预处理干预后显著提高了运动表现。这一发现与CARU等[2]的研究结果一致,他们发现缺血预处理在提升有氧表现方面对健康受试者的效果优于专业运动员[2]。在此研究中,考虑到缺血预处理对运动表现的总体提升效果较小(ES=0.13),可能是高水平运动员由于长期训练已具备较高的生理适应能力,从而对缺血预处理的响应较弱;而业余运动员或运动水平较低的受试者可能从中获益更多,这可能与他们尚未达到生理适应上限有关。
不仅如此,该研究发现缺血预处理会显著受到心理作用的影响,即安慰剂效应,这一现象在高水平运动员中尤为明显,因为他们经过长期训练可能具备更强的意志力或神经控制能力。例如,在SABINO-CARVALHO等[121]的研究中,他们发现缺血预处理后高水平运动员耐力表现的提升效果并不来源于缺血预处理本身,可能主要来源于心理作用,因为缺血预处理的改善并未显著超过安慰剂。此外,神经因素(如意志力或神经控制能力)本身就可以显著影响耐力表现,且这种影响与代谢反应的变化无关[136-137]。已有研究表明,缺血预处理能够有效优化神经肌肉性能的恢复,而这种效果同样不依赖于代谢相关参数[138];进一步的研究还发现,缺血预处理的强效作用可能与突触前抑制减少、运动神经元兴奋性增加以及功能性交感神经活动调节有关[41,76]。
基于以上证据,此研究认为在评估缺血预处理的效果时,不应仅关注受试者的运动水平差异,还需综合考虑神经控制能力和心理因素。未来的研究应进一步探讨运动经验水平与神经心理因素之间的交互作用,以更全面地理解缺血预处理的作用机制,并为不同运动水平的个体制定更具针对性的干预策略。此外,建议在缺血预处理干预中纳入心理调节训练,以最大化其潜在效益,特别是对高水平运动员群体。
3.7 人口统计学因素 此研究发现,尽管性别在组间分析中未表现为显著的调节因素,但组内分析显示,缺血预处理仅对男性运动表现有显著提升效果,表明在特定亚组中性别可能存在一定的影响趋势。这一观点得到了一些研究的支持,例如一项针对性别差异的力竭测试发现,缺血预处理对任务失败时间的促进作用仅在男性中观察到[16]。还有研究发现,缺血预处理可能影响到功能性交感神经,进而促进握力运动的表现,然而这样的效果仅在男性中观察到[41]。此研究认为,尽管男性似乎在提升运动表现方面更有优势,但仍不能忽视缺血预处理的安慰剂效应,因为在PEREIRA等[16]的研究中,虽然发现了男性的运动表现提升效果优于女性,但他们也同样认为主要原因可能是个体的主观感知所导致的。鉴于组间差异未达统计学显著,因此该结论应谨慎解读,未来研究仍需在更大样本下进一步验证性别变量的真实调节作用。
关于年龄因素的影响,虽然此研究回归分析发现年龄不是缺血预处理提升运动的调节因素,但这一结果可能受到样本年龄分布不均的限制。具体而言,该研究样本主要集中在20-30岁年龄段,而60-70岁年龄段的受试者较少,40-60岁的研究样本更是完全缺失,这种不均衡的年龄分布可能导致结果的偏差。值得提出的是,单独的缺血预处理(不结合运动)对老年人的健康促进来说似乎并不是一个有效的策略。例如有研究对比了高强度间歇训练、等长握力训练以及缺血预处理对收缩压的影响,发现缺血预处理相对其他两种方法并不能显著降低收缩压[139]。然而,这并不意味着缺血预处理对老年人不会产生任何积极影响。研究发现,缺血预处理可以促进活跃的老年妇女手握力量和功能能力的急性改善[68],此外缺血预处理还可显著提高平衡能力[98]、降低老年人的收缩压并且不会产生额外的疲劳[119]。这些研究结果凸显了缺血预处理对老年人来说可能是一种省时有效的健康促进策略,特别是在改善特定功能指标方面具有潜在价值。未来的研究应当进一步扩大样本年龄范围,特别是加强中年和老年人群的研究,以更全面地评估缺血预处理在不同年龄段的效果。
3.8 研究局限 ①由于此研究所纳入文献中的缺血肢体部位来自上肢、下肢、同侧或单侧、近端或远端且压力标准差异较大,包括动脉闭塞压力标准、收缩压标准以及压力范围标准等,因此,研究未对缺血标准和肢体部位进行亚组分析,因为这些不同变量会极大程度增加研究的异质性,即便是进行分析也会得到极不稳健的结果。②此研究计算了所纳入文献的所有受试者,共1 439名受试者,男性1 033名,女性210名,有196名在文献中未详细报告性别,此外,有29项研究的受试者为男女混合性别。尽管总体样本量较大,但男女性别比例差异较大,这样的比例分布不均可能会间接影响到结果的确定性。③此研究比较模型包括前-后测数据和仅后测数据分析。尽管Cochrane手册不建议在计算标准差时混合使用这些方法[44],但大量研究发现,混合使用不同的比较模型不会影响结果。此研究比较了不同的比较模型(仅事后评分与变化评分),发现结果稳定。④此研究未对缺血预处理干预与运动测试之间的间隔时间进行系统性分析,主要限制源于当前实证研究在该变量设定上的高度异质性。具体而言,已纳入的90篇文献中,间隔时间从缺血预处理干预结束后立即进行测试,至延迟12 h不等,缺乏统一标准。在这一广泛分布区间内,热身环节在各研究中被纳入的时点亦不一致。部分研究在间隔期结束与正式测试之间未设置热身,而另一些研究则将热身嵌套于二者之间,甚至成为“间隔时间”的组成部分。这种设计上的不确定性使得“缺血预处理→间隔→测试”这一干预流程中的关键环节被混合处理,并且热身能够有效提高运动表现已成为体育科学领域的一个共识,其干扰作用不应忽视。因此,该研究认为目前尚不具备对“间隔时间”变量进行量化回归分析的基础,并且研究团队就这一研究局限(也是当前领域的研究不足)的观点发表在了该领域的TOP期刊(中科院一区)[140]。因此,未来研究若能在干预流程设计中严格区分缺血预处理干预后“纯间隔时间”与“复合干预间隔”(如嵌入热身、测量等因素),或将有助于厘清时间因素对缺血预处理生理机制与表现效应的具体调节路径。
3.9 结论 该研究通过对90项随机交叉和随机对照试验的系统综述与荟萃分析,证实了缺血预处理对无氧和有氧运动表现的急性提升效果,效应量较小(ES=0.13),证据等级为低。缺血预处理的效果受到安慰剂效应、缺血与再灌注时间方案两类因素的调节。运动经验水平较低的男性受试者在部分结果中展现出更强的反应趋势,但性别和运动经验水平作为调节变量的效应尚未得到明确的数据支持,仍需进一步研究确认。具体而言,安慰剂效应在缺血预处理提升运动表现的效果中尤为显著,3×5 min与4×5 min的缺血预处理方案在提升运动表现方面较为有效。尽管缺血预处理对老年人的健康促进效果有限,但在改善特定功能指标方面仍具潜力。未来研究需进一步控制安慰剂效应,探讨缺血预处理的生理机制及其在不同年龄阶段、性别、压力标准等变量下的的真实效应。
3.10 未来研究方向 ①未来研究应致力于制定标准化的缺血预处理方案,包括统一的缺血压力标准(如动脉闭塞压力、收缩压或压力范围)以及明确的肢体部位选择(如上肢或下肢、单侧或双侧、近端或远端)。通过标准化试验设计,可以减少异质性,提高研究结果的可比性和稳健性。通过原创研究以对比不同肢体、同侧或单侧、不同压力标准对缺血预处理的效果差异。②未来的研究应该更多的关注缺血预处理对女性的生理机制与真实效应,此外,可在严格的变量控制下对比男女之间的性别差异。③尽管该研究发现混合使用前-后测数据和仅后测数据对结果影响较小,但未来研究仍应优化比较模型,采用更一致的数据分析方法。例如,可以设计前瞻性研究,统一采用前-后测数据或仅后测数据,以减少方法学差异对结果的潜在影响。此外,可以开发新的统计模型或机器学习方法,以更准确地评估缺血预处理的效果及其影响因素。④未来的研究应重点探讨缺血预处理与运动测试之间的间隔时间对效果的影响,并建立标准化的间隔时间框架。具体包括优化间隔时间(如即刻,30 min,1 h,6 h,12 h等)以确定最佳时间窗口,制定统一的热身方案以减少因热身不一致导致的混杂因素,尤其是考虑到缺血预处理后是否添加热身及其添加与不添加的生理机制,探讨间隔时间与热身环节的交互作用及其对缺血预处理效果的影响,并结合生理学指标(如血流动力学、代谢变化等)深入研究间隔时间影响缺血预处理效果的潜在机制。
中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
近年来,缺血预处理在运动表现提升领域逐渐成为研究热点,其潜在机制被认为涉及神经和体液调节、局部血流重分配与代谢适应等多重路径。然而,已有研究在干预方法、受试者特征和测量指标等方面存在显著异质性,导致效果不确定性较高。未来的发展趋势可能聚焦于安慰剂效应控制、标准化干预方案制定,以及结合运动模式与个体差异的精准干预策略构建。本研究通过系统评价与多层次荟萃分析,首次从缺血方案、运动经验、性别等多维度检验了缺血预处理效果的异质来源,厘清了其微弱但存在的运动表现提升效应及潜在影响因素,并确定在现有研究领域中其效应会显著的受到安慰剂效应(心理作用)的影响。相较于以往定性综述或单层次分析的研究,本研究在方法学深度与结果解释上具有一定的创新性和前沿性,为缺血预处理干预的临床应用及未来研究方向提供了较为系统的参考框架。
中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||