[1] WILMOT AS, RUUTIAINEN AT, BAKHRU PT, et al. Subchondral insufficiency fracture of the knee: A recognizable associated soft tissue edema pattern and a similar distribution among men and women. Eur J Radiol. 2016;85(11):2096-2103.
[2] AKAMATSU Y, MITSUGI N, HAYASHI T, et al. Low bone mineral density is associated with the onset of spontaneous osteonecrosis of the knee. Acta Orthop. 2012;83(3):249-255.
[3] NORMAN A, BAKER ND. Spontaneous osteonecrosis of the knee and medial meniscal tears. Radiology. 1978;129(3):653-656.
[4] TSUKAMOTO H, SAITO H, SAITO K, et al. Radiographic deformities of the lower extremity in patients with spontaneous osteonecrosis of the knee. Knee. 2020;27(3):838-845.
[5] ROBERTSON DD, ARMFIELD DR, TOWERS JD, et al. Meniscal root injury and spontaneous osteonecrosis of the knee: an observation. J Bone Joint Surg Br. 2009;91(2):190-195.
[6] HUSSAIN ZB, CHAHLA J, MANDELBAUM BR, et al. The Role of Meniscal Tears in Spontaneous Osteonecrosis of the Knee: A Systematic Review of Suspected Etiology and a Call to Revisit Nomenclature. Am J of Sports Med. 2019;47(2):501-507.
[7] 沈茂荣,王平,沈欣欣,等. 膝关节自发性骨坏死相关机制的研究进展[J]. 中医临床研究,2021,13(18):113-116.
[8] OCHI J, NOZAKI T, NIMURA A, et al. Subchondral insufficiency fracture of the knee: review of current concepts and radiological differential diagnoses. Jpn J Radiol. 2022;40(5):443-457.
[9] MAROM N, KOCH JE, BEER Y, et al. Thrombophilia-Associated Factors in Patients with Spontaneous Osteonecrosis of the Knee. Cartilage. 2019;10(1):53-60.
[10] BJÖRKMAN A, BURTSCHER IM, SVENSSON PJ, et al. Factor V Leiden and the prothrombin 20210A gene mutation and osteonecrosis of the knee. Arch Orthop Trauma Surg. 2005;125(1):51-55.
[11] GLUECK CJ, FREIBERG RA, WANG P. Medical Treatment of Osteonecrosis of the Knee Associated With Thrombophilia-Hypofibrinolysis. Orthopedics. 2014;37(10):e911-e916.
[12] 刘新光,王卫国,张念非,等. 膝关节自发性骨坏死与内侧半月板突出相关性的MRI观察[J]. 中国矫形外科杂志,2016,24(5):421-426.
[13] FUJISAWA T, CHOE H, KUSABA Y, et al. Medial meniscus extrusion and stage are related to the size of spontaneous osteonecrosis of the knee in patients who underwent high tibial osteotomy. Knee. 2022;36:72-79.
[14] SUNG JH, HA JK, LEE DW, et al. Meniscal Extrusion and Spontaneous Osteonecrosis With Root Tear of Medial Meniscus: Comparison With Horizontal Tear. Arthroscopy. 2013;29(4):726-732.
[15] ODA S, FUJITA A, MORIUCHI H, et al. Medial meniscal extrusion and spontaneous osteonecrosis of the knee. J Orthop Sci. 2019;24(5):867-872.
[16] 黄竞敏,李昱鸿,李冬超,等. 内侧半月板外突与半月板损伤及膝内翻的相关性研究[J]. 中华骨科杂志,2016,36(3):156-161.
[17] HASHIMOTO S, TERAUCHI M, HATAYAMA K, et al. Medial meniscus extrusion as a predictor for a poor prognosis in patients with spontaneous osteonecrosis of the knee. Knee. 2021;31:164-171.
[18] AKAMATSU Y, KOBAYASHI H, KUSAYAMA Y, et al. Predictive factors for the progression of spontaneous osteonecrosis of the knee. Knee Surg Sports Traumatol Arthrosc. 2017;25(2):477-484.
[19] GOSHIMA K, SAWAGUCHI T, SHIGEMOTO K, et al. Open-wedge high tibial osteotomy for spontaneous osteonecrosis of the medial tibial plateau shows excellent clinical outcomes. J Exp Orthop. 2020;7(1):14.
[20] NAKAYAMA H, ISEKI T, KANTO R, et al. Analysis of risk factors for poor prognosis in conservatively managed early-stage spontaneous osteonecrosis of the knee. Knee. 2016;23(1):25-28.
[21] KOSHINO T, OKAMOTO R, TAKAMURA K, et al. Arthroscopy in spontaneous osteonecrosis of the knee. Orthop Clin North Am. 1979; 10(3):609-618.
[22] KOSHINO T. The treatment of spontaneous osteonecrosis of the knee by high tibial osteotomy with and without bone-grafting or drilling of the lesion. J Bone Joint Surg Am.1982;64(1):47-58.
[23] AGLIETTI P, BUZZI R. Idiopathic osteonecrosis of the knee. Ital J Orthop Traumatol. 1984;10(2):217-226.
[24] MONT MA, BAUMGARTEN KM, RIFAI A, et al. Atraumatic osteonecrosis of the knee. J Bone Joint Surg Am. 2000;82(9):1279-1290.
[25] DUANY NG, ZYWIEL MG, MCGRATH MS, et al. Joint-preserving surgical treatment of spontaneous osteonecrosis of the knee. Arch Orthop Trauma Surg. 2010;130(1):11-16.
[26] MUHEIM G, BOHNE WH. Prognosis in spontaneous osteonecrosis of the knee. Investigation by radionuclide scintimetry and radiography. J Bone Joint Surg Br. 1970;52(4):605-612.
[27] LOTKE PA, ECKER ML. Osteonecrosis of the knee. J Bone Joint Surg Am. 1988;70(3):470-473.
[28] AGLIETTI P, INSALL JN, BUZZI R, et al. Idiopathic osteonecrosis of the knee. Aetiology, prognosis and treatment. J Bone Joint Surg Br. 1983;65(5):588-597.
[29] LOTKE PA, ABEND JA, ECKER ML. The treatment of osteonecrosis of the medial femoral condyle. Clin Orthop Relat Res. 1982;(171):109-116.
[30] JURÉUS J, LINDSTRAND A, GEIJER M, et al. The natural course of spontaneous osteonecrosis of the knee (SPONK): a 1- to 27-year follow-up of 40 patients. Acta Orthop. 2013;84(4):410-414.
[31] SOUCACOS PN, JOHNSON EO, SOULTANIS K, et al. Diagnosis and management of the osteonecrotic triad of the knee. Orthop Clin North Am. 2004;35(3):371-381.
[32] KERBOUL M, THOMINE J, POSTEL M, et al. The conservative surgical treatment of idiopathic aseptic necrosis of the femoral head. J Bone Joint Surg Br. 1974;56(2):291-296.
[33] PAPE D, SEIL R, FRITSCH E, et al. Prevalence of spontaneous osteonecrosis of the medial femoral condyle in elderly patients. Knee Surg Sports Traumatol Arthrosc. 2002;10(4):233-240.
[34] 王浩浩,张民,席刚,等.膝关节自发性骨坏死的保膝治疗研究进展[J]. 实用骨科杂志,2020,26(12):1127-1131.
[35] FORST J, FORST R, HELLER KD, et al. Spontaneous osteonecrosis of the femoral condyle: causal treatment by early core decompression. Arch Orthop Trauma Surg. 1998;117(1-2):18-22.
[36] TÍRICO L, EARLY SA, MCCAULEY JC, et al. Fresh Osteochondral Allograft Transplantation for Spontaneous Osteonecrosis of the Knee: A Case Series. Orthop J Sports Med. 2017;5(10):1808777964.
[37] 侯威宇,段圆慧,孙云波,等.自体骨软骨移植联合开放楔形胫骨高位截骨术治疗膝关节自发性骨坏死的临床疗效[J]. 实用骨科杂志,2021,27(8):753-757.
[38] TAKEUCHI R, ARATAKE M, BITO H, et al. Clinical results and radiographical evaluation of opening wedge high tibial osteotomy for spontaneous osteonecrosis of the knee. Knee Surg Sports Traumatol Arthrosc. 2009;17(4):361-368.
[39] 叶培,董志兴,王立晖,等. 全膝关节置换术治疗晚期膝关节自发性骨坏死[J]. 中国骨与关节损伤杂志,2021,36(8):837-839.
[40] CHOY WS, KIM KJ, LEE SK, et al. Medial unicompartmental knee arthroplasty in patients with spontaneous osteonecrosis of the knee. Clin Orthop Surg. 2011;3(4):279-284.
|
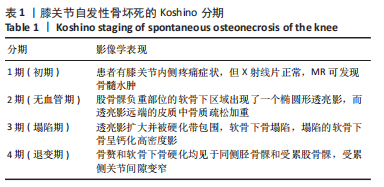
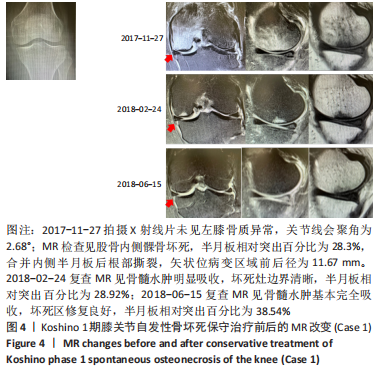



 Koshino 1期的SONK(如Case 1),建议保守治疗,具体方案包括选择消炎止痛药物、抗骨质疏松药物(钙剂、骨化三醇、唑来膦酸钠注射液/地舒单抗注射液)、避免负重及支架保护等方法[34]。
Koshino 1期的SONK(如Case 1),建议保守治疗,具体方案包括选择消炎止痛药物、抗骨质疏松药物(钙剂、骨化三醇、唑来膦酸钠注射液/地舒单抗注射液)、避免负重及支架保护等方法[34]。