中国组织工程研究 ›› 2015, Vol. 19 ›› Issue (24): 3818-3823.doi: 10.3969/j.issn.2095-4344.2015.24.010
• 口腔组织构建 oral tissue construction • 上一篇 下一篇
成人单侧完全性唇腭裂双侧髁突的形态特点
李增才,刘新强
- 青岛大学附属医院口腔正畸科,山东省青岛市 266003
-
出版日期:2015-06-11发布日期:2015-06-11 -
通讯作者:刘新强,硕士,主任医生,硕士生导师,青岛大学附属医院口腔正畸科,山东省青岛市 266003 -
作者简介:李增才,男,1986年生,汉族,青岛大学在读硕士,主要从事口腔正畸方面的研究。
Bilateral condylar morphology in adult patients with unilateral cleft lip and palate
Li Zeng-cai, Liu Xin-qiang
- Department of Orthodontics, the Affiliated Hospital of Qingdao University, Qingdao 266003, Shandong Province, China
-
Online:2015-06-11Published:2015-06-11 -
Contact:Liu Xin-qiang, Master, Chief physician, Master’s supervisor, Department of Orthodontics, the Affiliated Hospital of Qingdao University, Qingdao 266003, Shandong Province, China -
About author:Li Zeng-cai, Studying for master’s degree, Qingdao University, Qingdao 266003, Shandong Province, China
摘要:
背景:对单侧完全性唇腭裂患者进行正畸治疗,应首先了解其髁突形态的特点。 目的:探索成人单侧完全性唇腭裂患者双侧髁突形态的特点。 方法:收集临床单侧完全性唇腭裂患者和正常志愿者各25例,分别作为实验组和对照组,通过全颌曲面断层片,测量髁突上部高度、升支高度、髁突高度、髁突颈部宽度,并计算髁突上部高度/升支高度和髁突高度/髁突颈部宽度。 结果与结论:与对照组相比,实验组患者健侧和缺损侧髁突上部高度、髁突颈部宽度、髁突高度、髁突上部高度/升支高度减小(P < 0.05),且髁突形态类型存在明显差异,但升支高度和髁突高度/髁突颈部宽度差异无显著性意义(P > 0.05),且实验组患者健侧和缺损侧髁突上部高度、升支高度、髁突颈部宽度、髁突高度、髁突上部高度/升支高度、髁突高度/髁突颈部宽度以及髁突形态差异无显著性意义(P > 0.05)。说明成人单侧完全性唇腭裂患者呈现髁突短而颈部窄,髁突相对下颌升支短小的特点,这为临床上矫治单侧完全性唇腭裂患者提供临床依据。 中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
中图分类号:
引用本文
李增才,刘新强. 成人单侧完全性唇腭裂双侧髁突的形态特点[J]. 中国组织工程研究, 2015, 19(24): 3818-3823.
Li Zeng-cai, Liu Xin-qiang. Bilateral condylar morphology in adult patients with unilateral cleft lip and palate [J]. Chinese Journal of Tissue Engineering Research, 2015, 19(24): 3818-3823.
Quantitative analysis and clinical information of experimental subjects
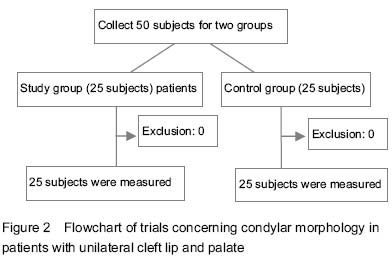
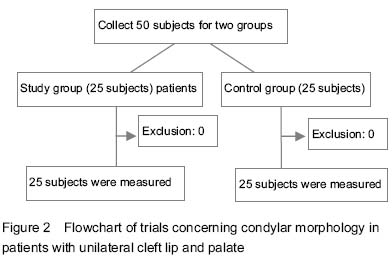
All patients were involved in the final analysis, no loss. Flowchart of trials is displayed in Figure 2.
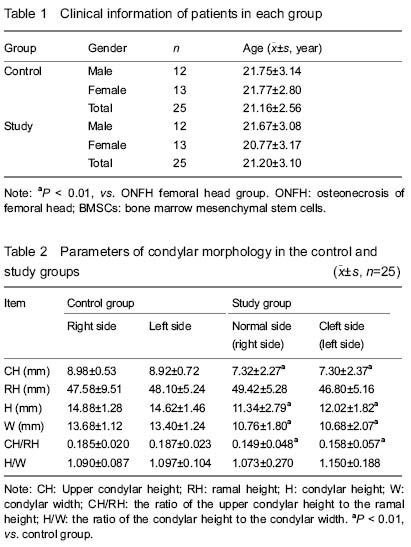
The age distributions in the two groups are shown in
Table 1. There was statistically insignificant difference between the male and female in condylar morphology[32-35]. Therefore, data for both genders were pooled for analyses.
Condylar morphology
Descriptive statistics and comparison of upper condylar height, ramal height, condylar height, condylar width, the ratio of the upper condylar height to the ramal height and the ratio of the condylar height to the condylar width for the right and left sides in the control group are shown in Table 2. There was no statistically significant difference in the control group (P > 0.05). Therefore, data for both sides in the control group were pooled for further analyses. Statistical comparison of measurements for the normal and cleft sides in the study group is shown in Table 2. There was statistically insignificant difference in the study group (P > 0.05).
Statistical results of tests comparing the measurements of the control group and the normal side in the study group are shown in Table 2. There was statistically significant difference in the upper condylar height, condylar height, condylar width, and the ratio of the upper condylar height to the ramal height (P=0.000, P=0.000, P=0.000 and P=0.000, respectively). However, there was not statistically significant difference in ramal height and the ratio of the condylar height to the condylar width (P > 0.05). Statistical results of tests comparing the measurements of the control group and the cleft side in the study group are shown in Table 2. There was statistically significant difference in the upper condylar height, condylar height, condylar width, and the ratio of the upper condylar height to the ramal height (P=0.000, P=0.000, P=0.000 and P=0.003, respectively), but ramal height and the ratio of the condylar height to the condylar width did not exhibit any statistically significant difference (P > 0.05).
| [1] Toro-Ibacache V, Cortés Araya J, Díaz Muñoz A, et al. Morphologic variability of nonsyndromic operated patients affected by cleft lip and palate: a geometric morphometric study. Am J Orthod Dentofacial Orthop. 2014;146(3):346-354. [2] Dixon MJ, Marazita ML, Beaty TH, et al. Cleft lip and palate: understanding genetic and environmental influences. Nat Rev Genet. 2011;12(3):167-178. [3] Wang KH, Heike CL, Clarkson MD, et al. Evaluation and integration of disparate classification systems for clefts of the lip. Front Physiol. 2014;5:163. [4] Sasaki Y, Taya Y, Saito K, et al. Molecular contribution to cleft palate production in cleft lip mice. Congenit Anom (Kyoto). 2014;54(2):94-99. [5] Kim NY, Kim YH, Park JW, et al. Association between MSX1 SNPs and nonsyndromic cleft lip with or without cleft palate in the Korean population. J Korean Med Sci. 2013; 28(4):522-526. [6] Younkin SG, Scharpf RB, Schwender H, et al. A genome-wide study of de novo deletions identifies a candidate locus for non-syndromic isolated cleft lip/palate risk. BMC Genet. 2014;15:24. [7] Beaty TH, Taub MA, Scott AF, et al. Confirming genes influencing risk to cleft lip with/without cleft palate in a case-parent trio study. Hum Genet. 2013;132(7):771-781. [8] Mossey PA, Modell B. Epidemiology of oral clefts 2012: an international perspective. Front Oral Biol. 2012;16:1-18. [9] Prescott NJ, Winter RM, Malcolm S. Nonsyndromic cleft lip and palate: complex genetics and environmental effects. Ann Hum Genet. 2001;65(Pt 6):505-515. [10] Kesande T, Muwazi LM, Bataringaya A, et al. Prevalence, pattern and perceptions of cleft lip and cleft palate among children born in two hospitals in Kisoro District, Uganda. BMC Oral Health. 2014;14:104. [11] Leslie EJ, Marazita ML. Genetics of cleft lip and cleft palate. Am J Med Genet C Semin Med Genet. 2013;163C(4):246-258. [12] Diah E, Lo LJ, Huang CS, et al. Maxillary growth of adult patients with unoperated cleft: answers to the debates. J Plast Reconstr Aesthet Surg. 2007;60(4):407-413. [13] Bartzela T, Katsaros C, Rønning E, et al. A longitudinal three-center study of craniofacial morphology at 6 and 12 years of age in patients with complete bilateral cleft lip and palate. Clin Oral Investig. 2012;16(4):1313-1324. [14] Chiu YT, Liao YF. Is cleft severity related to maxillary growth in patients with unilateral cleft lip and palate? Cleft Palate Craniofac J. 2012;49(5):535-540. [15] Garib DG, Santos PB, Janson G, et al. Association Between Dental Arch Widths and Interarch Relationships in Children With Operated Unilateral Complete Cleft Lip and Palate. Cleft Palate Craniofac J. 2013. in press. [16] Freitas JA, das Neves LT, de Almeida AL, et al. Rehabilitative treatment of cleft lip and palate: experience of the Hospital for Rehabilitation of Craniofacial Anomalies/USP (HRAC/USP)--Part 1: overall aspects. J Appl Oral Sci. 2012;20(1):9-15. [17] da Silva Filho OG, Normando AD, Capelozza Filho L. Mandibular growth in patients with cleft lip and/or cleft palate--the influence of cleft type. Am J Orthod Dentofacial Orthop. 1993;104(3):269-275. [18] Silva Filho OG, Calvano F, Assunção AG, et al. Craniofacial morphology in children with complete unilateral cleft lip and palate: a comparison of two surgical protocols. Angle Orthod. 2001;71(4):274-284. [19] Susami T, Okayasu M, Inokuchi T, et al. Maxillary protraction in patients with cleft lip and palate in mixed dentition: cephalometric evaluation after completion of growth. Cleft Palate Craniofac J. 2014;51(5):514-524. [20] Latief BS, Lekkas KC, Schols JG, et al. Width and elevation of the palatal shelves in unoperated unilateral and bilateral cleft lip and palate patients in the permanent dentition. J Anat. 2012;220(3):263-270. [21] Wu TT, Ko EW, Chen PK, et al. Craniofacial characteristics in unilateral complete cleft lip and palate patients with congenitally missing teeth. Am J Orthod Dentofacial Orthop. 2013;144(3):381-390. [22] Habets LL, Bezuur JN, Naeiji M, et al. The Orthopantomogram, an aid in diagnosis of temporomandibular joint problems. II. The vertical symmetry. J Oral Rehabil. 1988;15(5):465-471. [23] Kilic N, Kiki A, Oktay H. Condylar asymmetry in unilateral posterior crossbite patients. Am J Orthod Dentofacial Orthop. 2008;133(3):382-387. [24] Kiki A, Kiliç N, Oktay H. Condylar asymmetry in bilateral posterior crossbite patients. Angle Orthod. 2007;77(1):77-81. [25] Uysal T, Sisman Y, Kurt G, et al. Condylar and ramal vertical asymmetry in unilateral and bilateral posterior crossbite patients and a normal occlusion sample. Am J Orthod Dentofacial Orthop. 2009;136(1):37-43. [26] Jena AK, Singh SP, Utreja AK. Effects of sagittal maxillary growth hypoplasia severity on mandibular asymmetry in unilateral cleft lip and palate subjects. Angle Orthod. 2011; 81(5):872-877. [27] Abad-Santamaría L, López-de-Andrés A, Jiménez-Trujillo I, et al. Effect of unilateral posterior crossbite and unilateral cleft lip and palate on vertical mandibular asymmetry. Ir J Med Sci. 2014;183(3):357-362. [28] Veli I, Uysal T, Ozer T, et al. Mandibular asymmetry in unilateral and bilateral posterior crossbite patients using cone-beam computed tomography. Angle Orthod. 2011; 81(6):966-974. [29] Sanders DA, Rigali PH, Neace WP, et al. Skeletal and dental asymmetries in Class II subdivision malocclusions using cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2010;138(5):542.e1-20; discussion 542-543. [30] Ramirez-Yañez GO, Stewart A, Franken E, et al. Prevalence of mandibular asymmetries in growing patients. Eur J Orthod. 2011;33(3):236-242. [31] Kurt G, Bayram M, Uysal T, et al. Mandibular asymmetry in cleft lip and palate patients. Eur J Orthod. 2010;32(1): 19-23. [32] Celikoglu M, Halicioglu K, Buyuk SK, et al. Condylar and ramal vertical asymmetry in adolescent patients with cleft lip and palate evaluated with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2013;144(5): 691-697. [33] Bakri S, Rizell S, Lilja J, et al. Vertical maxillary growth after two different surgical protocols in unilateral cleft lip and palate patients. Cleft Palate Craniofac J. 2014;51(6): 645-650. [34] Hoppenreijs TJ, Freihofer HP, Stoelinga PJ, et al. Condylar remodelling and resorption after Le Fort I and bimaxillary osteotomies in patients with anterior open bite. A clinical and radiological study. Int J Oral Maxillofac Surg. 1998; 27(2): 81-91. [35] Borstlap WA, Stoelinga PJ, Hoppenreijs TJ, et al. Stabilisation of sagittal split advancement osteotomies with miniplates: a prospective, multicentre study with two-year follow-up. Part III--condylar remodelling and resorption. Int J Oral Maxillofac Surg. 2004;33(7):649-655. [36] Kambylafkas P, Murdock E, Gilda E, et al. Validity of panoramic radiographs for measuring mandibular asymmetry. Angle Orthod. 2006;76(3):388-393. [37] Silva MA, Wolf U, Heinicke F, et al. Cone-beam computed tomography for routine orthodontic treatment planning: a radiation dose evaluation. Am J Orthod Dentofacial Orthop. 2008;133(5):640.e1-5. [38] Roberts JA, Drage NA, Davies J, et al. Effective dose from cone beam CT examinations in dentistry. Br J Radiol. 2009; 82(973):35-40. [39] Lenza MG, Lenza MM, Dalstra M, et al. An analysis of different approaches to the assessment of upper airway morphology: a CBCT study. Orthod Craniofac Res. 2010; 13(2):96-105. [40] Graber TM. Panoramic radiography in orthodontic diagnosis. Am J Orthod. 1967;53(11):799-821. [41] Tronje G, Welander U, McDavid WD, et al. Image distortion in rotational panoramic radiography. IV. Object morphology; outer contours. Acta Radiol Diagn (Stockh). 1981;22(6): 689-696. [42] Larheim TA, Svanaes DB. Reproducibility of rotational panoramic radiography: mandibular linear dimensions and angles. Am J Orthod Dentofacial Orthop. 1986;90(1):45-51. [43] Türp JC, Vach W, Harbich K, et al. Determining mandibular condyle and ramus height with the help of an Orthopantomogram--a valid method? J Oral Rehabil. 1996; 23(6):395-400. [44] Azevedo AR, Janson G, Henriques JF, et al. Evaluation of asymmetries between subjects with Class II subdivision and apparent facial asymmetry and those with normal occlusion. Am J Orthod Dentofacial Orthop. 2006;129(3): 376-383. [45] Kitai N, Mukai Y, Murabayashi M, et al. Measurement accuracy with a new dental panoramic radiographic technique based on tomosynthesis. Angle Orthod. 2013; 83(1):117-126. [46] Habets LL, Bezuur JN, van Ooij CP, et al. The orthopantomogram, an aid in diagnosis of temporomandibular joint problems. I. The factor of vertical magnification. J Oral Rehabil. 1987;14(5):475-480. [47] White SC, Pharoah MJ. Oral radiology. 5th ed. St. Louis: Mosby, 2004. [48] Laspos CP, Kyrkanides S, Tallents RH, et al. Mandibular asymmetry in noncleft and unilateral cleft lip and palate individuals. Cleft Palate Craniofac J. 1997;34(5):410-416. [49] Shetye PR, Evans CA. Midfacial morphology in adult unoperated complete unilateral cleft lip and palate patients. Angle Orthod. 2006;76(5):810-816. [50] Ingervall B, Thilander B. Activity of temporal and masseter muscles in children with a lateral forced bite. Angle Orthod. 1975;45(4):249-258. [51] Pirttiniemi P, Kantomaa T, Salo L, et al. Effect of reduced articular function on deposition of type I and type II collagens in the mandibular condylar cartilage of the rat. Arch Oral Biol. 1996;41(1):127-131. [52] Copray JC, Jansen HW, Duterloo HS. Effects of compressive forces on proliferation and matrix synthesis in mandibular condylar cartilage of the rat in vitro. Arch Oral Biol. 1985;30(4):299-304. [53] Copray JC, Jansen HW, Duterloo HS. An in-vitro system for studying the effect of variable compressive forces on the mandibular condylar cartilage of the rat. Arch Oral Biol. 1985;30(4):305-311. [54] Inui M, Fushima K, Sato S. Facial asymmetry in temporomandibular joint disorders. J Oral Rehabil. 1999; 26(5):402-406. [55] Pirttiniemi P, Kantomaa T, Salo L, et al. Effect of reduced articular function on deposition of type I and type II collagens in the mandibular condylar cartilage of the rat. Arch Oral Biol. 1996;41(1):127-131. [56] Pinto AS, Buschang PH, Throckmorton GS, et al. Morphological and positional asymmetries of young children with functional unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 2001;120(5):513-520. [57] Horswell BB, Levant BA. Craniofacial growth in unilateral cleft lip and palate: skeletal growth from eight to eighteen years. Cleft Palate J. 1988;25(2):114-121. [58] Honda A, Baba Y, Ogawa T, et al. Long-term maxillomandibular changes after maxillary distraction osteogenesis in growing children with cleft lip with or without palate. Cleft Palate Craniofac J. 2013;50(2): 168-173. [59] Kyrkanides S, Richter L. Mandibular asymmetry and antigonial notching in individuals with unilateral cleft lip and palate. Cleft Palate Craniofac J. 2002;39(1):30-35. [60] de Moraes ME, Hollender LG, Chen CS, et al. Evaluating craniofacial asymmetry with digital cephalometric images and cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2011;139(6):e523-531. [61] Damstra J, Oosterkamp BC, Jansma J, et al. Combined 3-dimensional and mirror-image analysis for the diagnosis of asymmetry. Am J Orthod Dentofacial Orthop. 2011; 140(6):886-894. [62] Van Elslande DC, Russett SJ, Major PW, et al. Mandibular asymmetry diagnosis with panoramic imaging. Am J Orthod Dentofacial Orthop. 2008;134(2):183-192. |
| [1] | 张同同, 王中华, 文 杰, 宋玉鑫, 刘 林. 3D打印模型在颈椎肿瘤手术切除与重建中的应用[J]. 中国组织工程研究, 2021, 25(9): 1335-1339. |
| [2] | 刘亚非, 王雅淋, 左艳萍, 孙 琦, 尉 静, 赵利霞. X射线测量青少年骨性Ⅲ类患者前牵引治疗后颞下颌关节结构的改变[J]. 中国组织工程研究, 2021, 25(8): 1154-1159. |
| [3] | 吴 训, 孟娟红, 张建运, 王 亮. 浓缩生长因子修复兔髁突全层软骨损伤[J]. 中国组织工程研究, 2021, 25(8): 1166-1171. |
| [4] | 樊佳兵, 张军梅. 成年女性不同垂直骨面型下颌骨形态的测量分析[J]. 中国组织工程研究, 2021, 25(8): 1177-1183. |
| [5] | 曾燕华, 郝延磊. 许旺细胞体外培养及纯化的系统性综述[J]. 中国组织工程研究, 2021, 25(7): 1135-1141. |
| [6] | 徐东紫, 张 婷, 欧阳昭连. 心脏组织工程领域全球专利竞争态势分析[J]. 中国组织工程研究, 2021, 25(5): 807-812. |
| [7] | 吴子健, 胡昭端, 谢有琼, 王 峰, 李 佳, 李柏村, 蔡国伟, 彭 锐. 3D打印技术与骨组织工程研究文献计量及研究热点可视化分析[J]. 中国组织工程研究, 2021, 25(4): 564-569. |
| [8] | 常文辽, 赵 杰, 孙晓亮, 王 锟, 吴国锋, 周 剑, 李树祥, 孙 晗. 人工骨膜的材料选择、理论设计及生物仿生功能[J]. 中国组织工程研究, 2021, 25(4): 600-606. |
| [9] | 刘 旒, 周箐竹, 龚 桌, 刘博言, 杨 斌, 赵 娴. 胶原/无机材料构建组织工程骨的特点及制造技术[J]. 中国组织工程研究, 2021, 25(4): 607-613. |
| [10] | 刘 飞, 崔宇韬, 刘 贺. 局部抗生素递送系统治疗骨髓炎的优势与问题[J]. 中国组织工程研究, 2021, 25(4): 614-620. |
| [11] | 李晓壮, 段 浩, 王伟舟, 唐志宏, 王旸昊, 何 飞. 骨组织工程材料治疗骨缺损疾病在体内实验中的应用[J]. 中国组织工程研究, 2021, 25(4): 626-631. |
| [12] | 张振坤, 李 喆, 李 亚, 王莹莹, 王亚苹, 周馨魁, 马珊珊, 关方霞. 海藻酸盐基水凝胶/敷料在创面愈合中的应用:持续、动态与顺序释放[J]. 中国组织工程研究, 2021, 25(4): 638-643. |
| [13] | 陈佳娜, 邱燕玲, 聂敏海, 刘旭倩. 组织工程支架材料修复口腔颌面部软组织缺损[J]. 中国组织工程研究, 2021, 25(4): 644-650. |
| [14] | 邢 浩, 张永红, 王 栋. 长骨大段骨缺损修复方法的优势与不足[J]. 中国组织工程研究, 2021, 25(3): 426-430. |
| [15] | 陈思奇, 先德彬, 徐荣胜, 覃中杰, 张 磊, 夏德林. 羟基磷灰石-磷酸三钙支架复合骨髓间充质干细胞和人脐静脉内皮细胞对大鼠颅骨缺损修复早期成血管的影响[J]. 中国组织工程研究, 2021, 25(22): 3458-3465. |
lip and palate evaluated with cone-beam computed tomography. In a review of the orthodontic literature, no published study was found that condylar morphology in patients with UCLP. This study was designed to mainly investigate the condylar morphology in the group of unilateral cleft lip and palate patients with comparison with subjects with non-UCLP patients, introducing to make treatment planning for UCLP patients.
中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
This is a synchronous non-randomized comparative study.
Experiments were performed at the Department of Orthodontics, the Affiliated Hospital of Qingdao University in China from December 2013 to November 2014.
Study group: The patients were selected from the Department of Orthodontics, The Affiliated Hospital of Qingdao University in China.
Measurement of condylar morphology
All panoramic radiographs were taken in a standard manner by the same operator, and were traced and measured manually by the same author. The outlines of the condyle and the ramal of both sides were traced on acetate paper. On the tracing paper[22,32-34], a line (O2O3-line) was drawn between the most lateral points of the condylar (O2) and of the ramal (O3) image (Figure 1A), this distance from O2 to O3 was termed ramal height. To the O2O3-line (the ramal tangent) from the most superior point of the condylar (C0) image, a perpendicular C0O1-line was drawn. The vertical distance from this line on the ramal tangent to O2 projected on the ramal tangent was measured; this distance was termed upper condylar height. A line (x-line) was drawn from the most lateral points of the neck of condylar (Figure 1B). To the x-line from the narrowest neck of condyle, a perpendicular y-line was drawn. The distance from C0 to y-line was measured and termed condylar height. The ratio of the upper condylar height to the ramal height and the ratio of the condylar height to the condylar width were calculated.
There was statistically insignificant difference between the normal and cleft sides in the measurements in the UCLP group.
实验通过全颌曲面断层片证实唇腭裂患者主要是髁突高度和宽度出现变化,而下颌升支没有变化,且而唇腭裂患者健侧和缺损侧髁突形态差异无显著性意义,因此应在正畸治疗中应考虑此一点。 中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
唇腭裂根据硬腭和软腭部的骨质、黏膜、肌层的裂开程度及部位,可分为:①软腭裂:仅软腭裂开,有时只限于腭垂。不分左右,一般不伴唇裂,临床上以女性比较多见。②不完全性腭裂:亦称部分腭裂。软腭完全裂开伴有部分硬腭裂;有时伴发单侧不完全唇裂,但牙槽突常完整。本型也无左右之分。③单侧完全性腭裂:裂隙自腭垂至切牙孔完全裂开,并斜向外侧直抵牙槽突,与牙槽裂相连;健侧裂隙缘与鼻中隔相连;牙槽突裂有时裂隙消失仅存裂缝,有时裂隙很宽;常伴发同侧唇裂。④双侧完全性腭裂:常与双侧唇裂同时发生,裂隙在前颌骨部分,各向两侧斜裂,直达牙槽突;鼻中隔、前颌突及前唇部分孤立于中央。⑤其他:除上述各类型外,还可以见到少数非典型的情况:如一侧完全、一侧不完全;腭垂缺失;黏膜下裂(隐裂);硬腭部分裂孔等。 中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||