Chinese Journal of Tissue Engineering Research ›› 2021, Vol. 25 ›› Issue (35): 5723-5728.doi: 10.12307/2021.306
Previous Articles Next Articles
Effects of maxillary expansion on temporomandibular joint and airway in children
Gao Liping1, Wan Lu1, Zeng Manman2, Li Xiaobing3, Zhong Wenyi1
- 1Prevention and Children’s Dentistry in the Affiliated Stomatological Hospital of Zunyi Medical University, Zunyi 563000, Guizhou Province, China; 2Department of Stomatology, North Sichuan Medical College, Nanchong 637000, Sichuan Province, China; 3Department of Children’s Stomatology, West China School/Hospital of Stomatology, Sichuan University, Chengdu 610041, Sichuan Province, China
-
Received:2020-12-21Revised:2020-12-24Accepted:2021-01-23Online:2021-12-18Published:2021-08-05 -
Contact:Zhong Wenyi, Master, Professor, Prevention and Children’s Dentistry in The Affiliated Stomatological Hospital of Zunyi Medical University, Zunyi 563000, Guizhou Province, China -
About author:Gao Liping, Master candidate, Prevention and Children’s Dentistry in the Affiliated Stomatological Hospital of Zunyi Medical University, Zunyi 563000, Guizhou Province, China -
Supported by:the Science & Technology Department of Sichuan Province, No. 2018ZDYF980 and 2018FZ0099 (to LJQ and LXB); the Science and Technology Project of Honghuagang District, Zunyi City, No. 2017 (20) and (2020) 295 (both to ZWY)
CLC Number:
Cite this article
Gao Liping, Wan Lu, Zeng Manman, Li Xiaobing, Zhong Wenyi. Effects of maxillary expansion on temporomandibular joint and airway in children[J]. Chinese Journal of Tissue Engineering Research, 2021, 25(35): 5723-5728.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
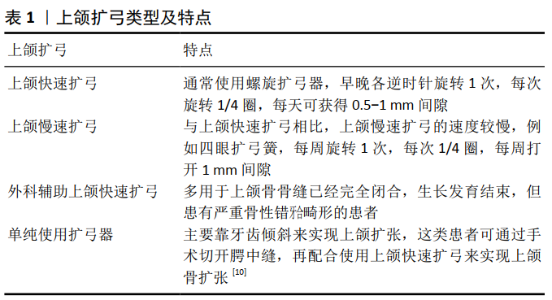
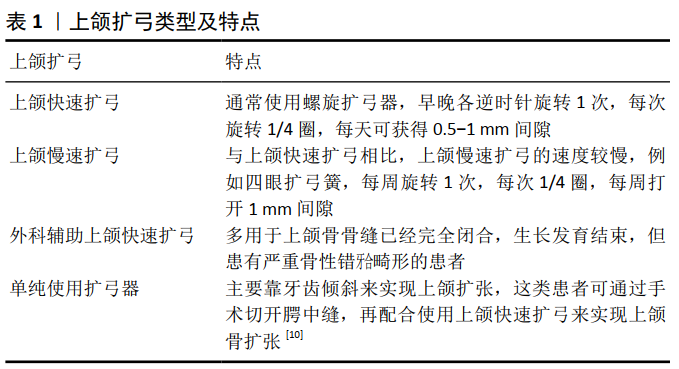
2.1 上颌扩弓的基本技术要点、生物力学机制及临床应用 2.1.1 上颌扩弓的定义、类型及方法 上颌扩弓是指通过正畸或外科辅助方式打开腭中缝,扩大上颌横向宽度,使上、下颌骨宽度及牙弓形态相协调的一种矫治方法。上颌扩弓按扩弓速度主要分为上颌快速扩弓、上颌慢速扩弓、上颌半快速扩弓、外科辅助上颌快速扩弓[9](见表1) 。 2.1.2 上颌扩弓的生物力学机制 上颌扩弓的原理是通过较大的机械力牵拉以打开腭中缝,促进腭中缝处的骨质沉积,从而实现扩大上颌横向宽度的目标。上颌快速扩弓及上颌慢速扩弓均能有效增加上颌骨的横向宽度,但二者的机制稍显不同。上颌快速扩弓主要作用于腭中缝[11] ,是以扩大上颌骨性轮廓为主,能够实现最大程度的骨性扩张和较小的牙齿倾斜移动[12] 。上颌慢速扩弓则主要作用于后牙牙颈部,通过牙齿倾斜移动,间接改变牙槽骨的骨弓轮廓,同时实现牙弓轮廓的扩大,与上颌快速扩弓相比较少作用于腭中缝[11] 。此外,也有研究指出上颌扩弓可引起上颌骨周围组织结构的变化,例如上颌扩弓能够改变鼻-上颌复合体的解剖生理结构,对改善鼻腔功能和提升鼻通气量也有一定的作用[13] 。 2.1.3 上颌扩弓的临床运用时机 不同年龄阶段的儿童,其腭中缝的骨化程度不同。随着年龄的增长,腭中缝处的骨质逐渐沉积、融合,钙化程度的增加也相应增大了扩弓的难 度[14-15]。MELSEN[16] 研究表明,腭中缝在10岁以前是未完全闭合的,大抵在14岁实现交错融合,对于未完全闭合的年轻患儿,单独使用扩弓器就能很好地完成腭中缝的扩展[17]。也有学者认为,20-25岁时腭中缝才能完全闭合[18] ,因此,对于错过青春生长迸发期的患儿,仍然可以考虑通过扩弓来改善上颌横向宽度不足的状态。 CAMERON等[19] 认为在骨生长停滞之前,上颌扩弓的应用能够最大程度地实现骨缝的扩张和生理性骨质沉积,从而达到较好的长期效果。对于骨性Ⅲ类伴有上牙弓狭窄的患儿,由于骨缝未完全闭合尚具有较大的生长潜力,但是延迟矫治时间,容易造成不可逆的骨性畸形,因此扩弓时机的选择就显得尤为重要。上颌扩弓主要适用于腭中缝未闭合、仍具有生长潜力的儿童及青少年[9]。临床上多选择尚在生长发育高峰期的患儿进行上颌快速扩弓治疗[20-21],而对于学龄前儿童通常不能使用上颌快速扩弓,其原因在于上颌快速扩弓容易导致鼻的“弓背样”畸形[22] 。相反地,上颌慢速扩弓更适用于矫治年龄较小的患者,其力较轻柔、对腭部及牙周组织的损伤较小、矫治后期稳定较好、复发率较低,但其扩弓速度会更慢[18] 。此外,也有不少学者观察发现,年龄越小的患者越容易扩开腭中缝[23] ,从而能够更快地完成矫治目标。 2.2 上颌扩弓对儿童颞下颌关节发育的影响 2.2.1 儿童颞下颌关节生理性发育及改建的特点 由于颞下颌关节在下颌运动中所处的关键位置,决定了下颌咀嚼、吞咽、说话和呼吸功能的协调发展[24]。儿童的颞下颌关节骨改建活跃,能够适应动态负荷下的功能性压应力的变化[25],通过将力传导至下颌骨骨化中心——髁突,引起髁突软骨膜增生形成纤维软骨,随后逐层钙化[26]。通过这种软骨内成骨的方式,最终实现下颌骨沿生物力学方向进行的三维向生长。 上颌扩弓能够间接改变髁突内应力的分布,刺激并诱导髁突软组织细胞的增生,从而实现对髁突形态的改建[27]。不少学者研究发现,儿童时期的髁突还处在生长发育阶段,仍具有重新定位、改建和重塑的能力,上颌快速扩弓可重新定位髁突在关节窝内的位置[28],并引导髁突头和髁突颈的重塑[29]。骨性Ⅲ类反牙合的患儿,往往伴有髁突位置不对称,双侧髁突所受的功能性压力不一致,进而导致髁突的发育畸形,甚至引起整个面型的偏斜,尽早治疗才能保证此类患儿的下颌骨沿着正确的方向生长。 2.2.2 上颌扩弓对儿童早期髁突所处关节窝位置的改变及生理意义 正常情况下,儿童在乳牙牙合时期,颞下颌关节所处的位置尚不稳定,在“六龄牙”萌出建牙合以后,达到牙尖交错位时髁突处于对称的、最前、最上位。错牙合畸形会改变髁突的相对位置[30],并引导髁突侧向移位,有研究通过髁突冠状角观察证实,这种髁突的移位是向前、下方进行的[31],也有研究发现后牙反牙合患者扩弓之前,两侧髁突位置在关节窝中有明显的差异性,非反牙合侧髁突的位置比牙合侧偏前[32]。对上颌横向发育异常的患儿,在进行早期干预时,能够帮助矫正后牙反牙合,改变原先的髁突位置,帮助实现髁突重塑[33]。LIPPOLD等[34] 发现,对处于生长发育期中的儿童,使用上颌快速扩弓能够在短期内改变髁突-窝的关系,改善髁突间的对称关系。从远期效果来看,上颌快速扩弓矫治1年后后牙反牙合患者的颅面部不对称性得到明显改善,而对于单侧后牙反牙合患者的下颌骨也可发生显著变化,双重髁突位置变得相对对称[35],对于功能性单侧后牙反牙合的患儿,目前的研究多表明早期使用上颌扩弓更有利于髁突及关节的生长发育。早期矫治单侧后牙反牙合可以改善咬合接触和提高咬合稳定 性[36],经过扩弓后,反牙合和非反牙合的髁突分别随下颌前移和后移[27],双侧髁突位置更加对称[33] 。VITRAL等[37] 研究发现,当使用上颌快速扩弓后,在正中关系-最大牙尖交错位时患者下颌功能性移位改善,颞下颌关节的CT图像显示髁突适应了一种新的颌位情况,髁突位置更对称更完美。同样,有学者发现在上颌扩弓前后,使用超声技术测量系统观察到髁突在正中和习惯性咬合间的异常移位减少,上颌扩弓后患者面部变得对称,下颌的功能性移位得到改善[34]。因此,改善髁突-关节窝之间的关系,对生长发育期的儿童而言,能够正确引导其下颌生长,对促进上、下牙弓协调一致发挥重要作用[38]。但也有学者认为后牙反牙合的矫正与髁突位置无关。COSKUNER等[39]认为用四眼圈簧扩张上颌可以在一定程度上纠正Ⅱ类关系,然而对颞下颌关节没有显著影响。MCLEOD等[40]使用CBCT对上颌扩张前后的髁突位置进行三维评估后发现,治疗组和对照组之间髁突的位置变化并不显著,尽管双侧髁突在关节窝内的位置改变在测量中具有统计学意义,但并没有实际的临床应用价值。 尽管目前针对后牙反牙合的患儿是否早期治疗尚有少许争议,但大多数学者支持为颞下颌关节创造一个良好的发育环境,早期矫治是必须的。它的意义在于对于那些严重影响髁突的发育及髁突-关节窝关系建立的错牙合畸形,早期使用上颌扩弓能够借助儿童髁突的生长发育潜力及重塑能力,使移位的髁突尽早回到正确位置,防止进一步恶化。 2.2.3 上颌扩弓对儿童早期关节盘-髁关系改变及生理意义 关节盘位于关节窝内、髁突头的上方,呈卵圆形、双凹状,具有缓冲应力的作用。在张闭口及咀嚼运动时,髁突与关节盘的动度协调一致,共同完成颞下颌关节的转动和滑动等生理过程。目前,关于上颌扩弓对儿童早期盘-髁关系的作用,大多数学者认为,扩弓不会影响关节正常的盘-髁关系,也不会造成关节盘形态和位置的改变[41-42]。MASI等[41]对30例功能性单侧后牙反牙合的患儿使用Haas型矫治器进行上颌扩弓后,采用MRI对治疗前后关节盘的位置、形态大小进行评估和测量,发现上颌扩弓后关节盘的位置和形态并没有任何变化;ARAT等[29]通过对7例单侧后牙反牙合和11例双侧后牙反牙合患者进行扩弓治疗,也得出了相似的结论,并推论可能是由于关节盘的软组织结构对压应力有较好的缓冲作用所致。此外,有部分学者对安氏Ⅱ类及Ⅲ类错牙合患者进行上颌扩弓治疗后,关节盘的位置出现可复性的前移[37,43],具体的作用机制尚不清楚[44] 。 2.2.4 上颌扩弓对颞下颌关节周围咀嚼肌的影响 上颌扩弓对颞下颌关节周围咀嚼肌是否存在作用,一直以来不同学者所持观点不同。对于后牙反牙合患者,研究发现反牙合的治疗有助于提高咀嚼肌的活动,使肌肉张力增加,使其接近正常咬合的水平[45]。有学者对上颌扩弓与后牙反牙合患者颞肌及咬肌肌电活动的关系发现,正畸治疗移动到正常且更有利的咬合关系时,颞肌与咬肌的肌电活动得到不同程度的增强[46]。在对咀嚼肌收缩活动之间的协调性研究中表明,对治疗前肌肉协调性良好的儿童来说,咀嚼肌群能够很好地适应上颌快速扩弓[36]。ARAT等[29] 研究发现,上颌快速扩弓术后,患者咀嚼过程中颞前肌与咬肌的肌电活动明显下降,但扩弓完成后1.5个月,其肌电活动均上升到扩弓前,术后3个月,其肌电活动对称并下降到正常值内。 上颌扩弓对单侧后牙反牙合肌肉活动影响的研究中,有学者发现,有或无单侧后牙反牙合的儿童在功能运动中均存在轻微的颞前肌和咬肌的不对称性活动,且单侧后牙反牙合儿童的肌肉不对称程度并不高于无反牙合的健康儿童[47] 。因此上颌快速扩弓对单侧后牙反牙合肌肉活动的协调性及对称性仍需进一步的研究。 2.3 上颌扩弓对儿童气道改变的影响 上颌快速扩弓不仅仅作用于腭中缝,还影响上颌骨及相关组织结构的变化,上颌牙弓狭窄患儿经上颌快速扩弓治疗后,鼻上颌复合体增宽,鼻咽及腭咽容积增加[48]。使用上颌快速扩弓时,腭中缝、翼上颌缝、鼻上颌缝、额上颌颌缝处应力较大,能使上颌骨产生金字塔形扩展,金字塔的顶点为鼻骨,基部位于口腔侧,鼻腔的后上部分在横向方向上移动最小,并且鼻底处的鼻腔宽度增加,上颌有向下和向前的运动及向后旋转的趋 势[49] ,气道容积的变化受扩弓速度影响。与上颌慢速扩弓相比,上颌快速扩弓使鼻腔和鼻咽的体积增加更大[50] 。Karaman 等[51] 发现鼻软组织的长度随着上颌骨的向前移位而增加,鼻软组织的宽度也明显增加[52],能够显著改变鼻腔的内部结构大小,显著增加了鼻腔和鼻咽的体积[53],鼻腔和咽部的气流压力均有下降,鼻气流增加,气道阻力降低[54],改善儿童和青少年的呼吸[55] 。 上颌发育不足的患者常伴有OSAHS,它是一种具有多种病因的睡眠障碍[56]。对于儿童,腺扁桃体肥大仍然是其主要解剖学危险因素。OSAHS特征是入睡时气道全部/部分阻塞,口-鼻气流降低,导致低氧血症和高碳酸血症[57],而此时期是大脑发育的关键时期,睡眠障碍会导致严重的不良后果,如发育迟缓、认知和行为异常、多动、注意力不集中、学习成绩差、心血管及其内皮功能障碍以及整体生活质量下降[58]。从此角度说明OSAHA的治疗非常迫切,需要及早发现和治疗。对于扁桃体肥大的患儿,腺扁桃体切除术已成为儿童OSAHS的首选治疗方法,但它们不能完全缓解疾病症状[59]。对上颌发育不足、下颌后缩伴OSAHS和打鼾的患儿,正畸治疗也起着重要作用,上颌快速扩弓能使鼻腔的外壁扩开、腭穹隆下降、鼻中隔变直[60],从而增加鼻腔体积、降低鼻腔对气流的阻力,鼻呼吸增加使腺样体倾向于恢复到生理性萎缩状态[61],扁桃体变小,从而有助于增加呼吸空间[62] ,这种作用在鼻腔的下部分更为明显[63],可以改善气道狭窄,提高呼吸的质量[64]。通过改善呼吸暂停低通气指数[65],增加平均血氧饱和度[66],从而减轻OSAHS并改善多导睡眠指标[67]。上颌快速扩弓扩宽上颌骨及牙弓的宽度的同时,也能够改善舌头的位置,使嘴唇在闭口时能够正常闭合,它也间接增加口咽间隙[68],这对于改善呼吸功能和颅面发育的治疗稳定性至关重要[69]。 使用上颌快速扩弓对声音也有一定的影响[70],并且发现用于评价语音质量的参数与鼻腔宽度的增加呈显著正相关[71],但目前关于这些内容尚处于研究阶段,有待进一步证实。 "
| [1] GUPTA ND, MAHESHWARI S, MITTAL S. Treatment of Class III by Biphasic therapy. Indian Ortho Soc. 2005;38:193-197. [2] MOMMAERTS MY, ABELOOS JVS, NEYT NMF, et al. Problems,obstacles and complications with transpalatal distraction in non-congenital deformities. Craniomaxillofac Surg. 2002;30(3):139-143. [3] 裘军,王萍,王列炜,等.安氏Ⅲ类错牙合畸形非拔牙矫正前后头影测量分析研究[J].临床军医杂志,2012,40(1):180-181. [4] 李小兵.基于牙弓形态大小发育的青少年隐形矫治[J].中国实用口腔科杂志,2019,12(8):449-454. [5] 韩科,张豪.牙合学理论与临床实践[M].北京:人民军医出版社, 2014:39-40. [6] CHIARI S, ROMSDORFER P, SWOBODA H, et al. Effects of rapid maxillary expansion on the airways and ears–a pilot study. Eur J Orthod. 2009; 31(2):135-141. [7] MACHADO-JÚNIOR AJ, ZANCANELLA E, CRESPO AN. Rapid maxillary expansion and obstructive sleep apnea: A review and meta-analysis.Med Oral Patol Oral Cir Bucal. 2016;21(4):e465-469. [8] CAMACHO M, CHANG ET, SONG SA, et al. Rapid maxillary expansion for pediatric obstructive sleep apnea: a systematic review and meta-analysis. Laryngoscope. 2017;127(7):1712-1719. [9] MCNAMARA JA JR, FRANCHI L, MCCLATCHEY LM. Orthodontic and orthopedic expansion of the transverse dimension: A four decade perspective. Semin Orthod. 2019;25(1):3-15. [10] SYGOUROS A, MOTRO M, UGURLU F, et al. Surgically assisted rapid maxillary expansion:Cone beam computed tomography evaluation of different surgical techniques and their effects on the maxillary dentoskeletal complex.Am J Orthod Dentofacial Orthop. 2014;146(6): 748-757. [11] BRUDER C, ORTOLANI CLF, LIMA TA, et al. Evaluation of palate area before and after rapid maxillary expansion, using cone-beam computed tomography. Dental Press J Orthod. 2019;24(5):40-45. [12] GECGELEN M, AKSOY A, KIRDEMIR P, et al. Evaluation of stress andpain during rapid maxillary expansion treatments. J Oral Rehabil. 2012; 39(10):767-755. [13] LIU JL, LI HF, YAN H. Comparing the effects of fast and slow expansion on nasal cavity and maxilla structure. Hua Xi Kou Qiang Yi Xue Za Zhi. 2019;37(5):533-536. [14] MORALIS A, ZITZMANN K, GOSAU M, et al. The effects of surgical expansion of the maxillary arch and its consequences for the incisor axis. Cranio-Maxillofac Surg. 2016;44(5): 569-573. [15] ANGELIERI F, FRANCHI L, CEVIDANES LH, et al. Diagnostic performance of skeletal maturity for the assessment of midpalatal suture maturation.Am J Orthod Dentofac Orthop. 2015;148(6):1010-1016. [16] MELSEN B. Palatal growth studied on human autopsy material. A histologic microradiographic study. Am J Orthod. 1975;68(1):42-54. [17] 徐舒豪,黄诗言,饶南荃,等.上颌横向发育不足的临床治疗进展[J]. 临床口腔医学杂志,2016,32(4):251-253. [18] 张晓芸.颅面部生长发育与错畸形的矫正时机(一)[J].中华口腔正畸学杂志,2012,19(1):41-45. [19] CAMERON CG, FRANCHI L, BACCETTI T, et al. Long-term effects of rapid maxillary expansion: A posteroanterior cephalometric evaluation. Am J Orthod Dentofacial Orthop. 2002;121(2):129-135. [20] MCNAMARA JA JR, LIONE R, FRANCHI L, et al. The role of rapid maxillary expansion in the promotion of oral and general health. Prog Orthod. 2015;16(1):33. [21] MOAWAD SG, BOUSERHAL J, AL-MUNAJED MK. Assessment of the efficiency of Erbium-YAG laser as an assistant method to rapid maxillary expansion: An in vivo study. Int Orthod. 2016;14(4):462-475. [22] 陈扬熙.口腔正畸学:基础、技术与临床[M].北京:人民卫生出版社, 2012:560-561. [23] 张月兰, 韦大鹏, BLESSING S, 等. 上颌四眼圈簧扩弓后对上颌牙齿及上颌骨变化影响的 CBCT 研究[J]. 实用口腔医学杂志,2016,32(2):216-219. [24] FANGHÄNEL J, GEDRANGE T. On the development, morphology and function of the temporomandibular joint in the light of the orofacial system. Ann Anat. 2007;189(4):314-319. [25] RAVOSA MJ, KANE RJ. Dietary variation and mechanical properties of articular cartilage in the temporomandibular joint: Implications for the role of plasticity in mechanobiology and pathobiology. Zoology (Jena). 2017;(10)124:42-50. [26] UTREJA A, DYMENT NA, YADAV S, et al. Cell and matrix response of temporomandibular cartilage to mechanical loading. Osteoarthritis Cartilage. 2016;24(2):335-344. [27] PAPACHRISTOU D, PIRTTINIEMI P, KANTOMAA T, et al. Fos- and Jun- related transcription factors are involved in the signal transduction pathway of mechanical loading in condylar chondrocytes. Eur J Orthod. 2006;28(1):20-26. [28] LIMA FILHO RM, DE OLIVEIRA RUELLAS AC. Mandibular behavior with slow and rapid maxillary expansion in skeletal Class II patients: A long-term study. Angle Orthod. 2007;77(4):625-631. [29] ARAT FE, ARAT ZM, TOMPSON B, et al. Muscular and condylar response to rapid maxillary expansion. Part 3: Magnetic resonance assessment of condyle-disc relationship. Am J Orthod Dentofacial Orthop. 2008; 133(6):830-836. [30] LEONARDI R, CALTABIANO M, CAVALLINI C, et al. Condyle Fossa relationship associated with functional posterior crossbite, before and after rapid maxillary expansion. Angle Orthod. 2012;82(6):1040-1046. [31] MELGAÇO CA, COLUMBANO NETO J, JURACH EM, et al. Immediate changes in condylar position after rapid maxillary expansion.Am J Orthod Dentofacial Orthop. 2014;145(6):771-779. [32] 苏盈盈,王春玲,李红,等.儿童功能性单侧后牙反牙合患者的髁突对称性及矫治后髁突位置变化的研究[J]. 口腔医学,2009,29(6): 305-308. [33] KECIK D, KOCADERELI I, SAATCI I. Evaluation of the treatment changes of functional posterior crossbite in the mixed dentition. Am J Orthod Dentofacial Orthop. 2007;131(2):202-215. [34] LIPPOLD C, HOPPE G, MOISEENKO T, et al. Analysis of condylar differences in functional unilateral posterior crossbite during early treatment-a randomized clinical study. J OrofacOrthop. 2008;69(4):283-296. [35] EVANGELISTA K, FERRARI-PILONI C, BARROS LAN, et al. Three-dimensional assessment of craniofacial asymmetry in children with transverse maxillary deficiency after rapid maxillary expansion: A prospective study. Orthod Craniofac Res. 2020;23(3):300-312. [36] DI EP, TEPEDINO M, CHIMENTI C, et al. Longitudinal effects of rapid maxillary expansion on masticatory muscles activity. J Clin Exp Dent. 2017;9(5):e635-e640. [37] VITRAL RW, FRAGA MR, DE OLIVEIRA RS, et al. Temporomandibular joint alterations after correction of a unilateral posterior crossbite in a mixed-dentition patient: A computed tomography study. Am J Orthod Dentofacial Orthop. 2007;132(3):395-399. [38] TORRES D, LOPES J, MAGNO MB, et al. Effects of rapid maxillary expansion on temporomandibular joints: A systematic review. Angle Orthod. 2020;90(3):442-456. [39] COSKUNER HG, CIGER S. Three-dimensional assessment of the temporomandibular joint and mandibular dimensions after early correction of the maxillary arch form in patients with Class II Division 1 or Division 2 malocclusion. Korean J Orthod. 2015;45(3):121-129. [40] MCLEOD L, HERNÁNDEZ IA, HEO G, et al. Condylar positional changes in rapid maxillary expansion assessed with cone-beam computer tomography. Int Orthod. 2016;14(3):342-356. [41] MASI M, LEDERMAN HM, YAMASHITA HK, et al. Temporomandibular joint evaluation with magnetic resonance imaging in children with functional unilateral posterior crossbite, treated with rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2009;136(2):207-217. [42] STOCUM DL, ROBERTS WE. Part I: Development and Physiology of the Temporomandibular Joint. Current Osteoporosis Reports. 2018;16(4) 360-368. [43] PINTO AS, BUSCHANG PH, THROCKMORTON GS, et al. Morphological and positional asymmetries of young children with functional unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 2001;120(5):513-520. [44] RUF S, WÜSTEN B, PANCHERZ H. Temporomandibular joint effects of activator treatment: A prospective longitudinal magnetic resonance imaging and clinical study. Angle Orthod. 2002;72(6):527-540. [45] MASPERO C, GIANNINI L, GALBIATI G, et al. Neuromuscular evaluation in young patients with unilateral posterior crossbite before and after rapid maxillary expansion. Stomatologija. 2015;17(3):84-88. [46] FARRONATO G, GIANNINI L, FOLEGATTI C, et al. Impacted maxillary canine on the position of the central incisor: Surgical-orthodontic repositioning. Minerva Stomatol. 2013;62(4):117-125. [47] MICHELOTTI A, RONGO R, VALENTINO R, et al. Evaluation of masticatory muscle activity in patients with unilateral posterior crossbite before and after rapid maxillary expansion. Eur J Orthod. 2019;41(1):46-53. [48] 常大桐, 周彦恒, 刘伟涛. 上颌反复快速扩缩对上气道影响的锥束CT研究[J].北京大学学报(医学版),2017,49(4):685-690. [49] PRIYADARSHINI J, MAHESH CM, CHANDRASHEKAR BS, et al. Stress and displacement patterns in the craniofacial skeleton with rapid maxillary expansion-a finite element method study. Prog Orthod. 2017;18(1):1-8. [50] LOTFI V, GHONEIMA A, LAGRAVERE M, et al. Three-dimensional evaluation of airway volume changes in two expansion activation protocols. Int Orthod. 2018;16(1):144-157. [51] KARAMAN AI, BASCIFTC¸IFA, GELGÖR IE, et al. Examination of soft tissue changes after rapid maxillary expansion. World J Orthod. 2002;3(3): 217-222. [52] PANGRAZIO-KULBERSH V, WINE P, HAUGHEY M, et al.Cone beam computed tomography evaluation of changes in the naso-maxillary complex associated with two types of maxillary expanders. Angle Orthod. 2012;82(3):448-457. [53] KAVAND G, LAGRAVERE M, KULA K, et al. Retrospective CBCT analysis of airway volume changes after bone-borne vs tooth-borne rapid maxillary expansion. Angle Orthod. 2019;89(4):566-574. [54] BAZARGANI F, MAGNUSON A, LUDWIG B. Effects on nasal airflow and resistance using two different RME appliances: a randomized controlled trial. Eur J Orthod. 2018;40(3):281-284. [55] ALYESSARY AS, OTHMAN SA, YAP AUJ, et al. Effects of non-surgical rapid maxillary expansion on nasal structures and breathing: A systematic review. Int Orthod. 2019;17(1): 12-19. [56] HOPPS E, CAIMI G.Obstructive Sleep Apnea Syndrome: Links Betwen Pathophysiology and Cardiovascular Complications. Clin Invest Med. 2015;38(6):E362-370. [57] KATZ ES, WHITE DP.Genioglossus activity in children with obstructive sleep apnea during wakefulness and sleep onset.Am J Respir Crit Care Med.2003;168(6):664-670. [58] MARCUS CL, MOORE RH, ROSEN CL, et al.A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med. 2013; 368(25):2366-2376. [59] WEISSBACH A, LEIBERMAN A, TARASIUK A, et al. Adenotonsilectomy improves enuresis in children with obstructive sleep apnea syndrome.Int J Pediatr Otorhinolaryngol. 2006;70(8):1351-1356. [60] BUCK L, DALCI O, DARENDELILER M, et al. V olumetric upper airway changes after rapid maxillary expansion: a systematic review and meta-analysis. Eur J Orthod. 2016;39(5):463-473. [61] TAPIA IE, MARCUS CL, MCDONOUGH JM, et al. Airway Resistance in Children with Obstructive Sleep Apnea Syndrome. Sleep. 2016;39(4): 793-799. [62] BIANCHI A, BETTI E, TARSITANO A, et al. Volumetric three-dimensional computed tomographic evaluation of the upper airway in patients with obstructive sleep apnoea syndrome treated by maxillomandibular advancement. Br J Oral Maxillofac Surg. 2014;52(9):831-837. [63] VINHA PP, ECKELI AL, FARIA AC, et al. Effects of surgically assisted rapid maxillary expansion on obstructive sleep apnea and daytime sleepiness.Sleep Breath. 2016;20(2):501-508. [64] EICHENBERGER M, BAUMGARTNER S. The impact of rapid palatal expansion on children’s general health: a literature review.Eur J Paediatr Dent. 2014;15(1):67-71. [65] VALE F,ALBERGARIA M,CARRILHO E, et al . Efficacy of Rapid Maxillary Expansion in the Treatment of Obstructive Sleep Apnea Syndrome: A Systematic Review With Meta-analysis. J Evid Based Dent Pract. 2017;17(3):159-168. [66] VILLA MP, CASTALDO R, MIANO S, et al. Adenotonsillectomy and orthodontic therapy in pediatric obstructive sleep apnea. Sleep Breath. 2014;18(3):533-539. [67] MCNAMARA JA, LIONE R, FRANCHI L, et al. The role of rapid maxillary expansion in the promotion of oral and general health. Prog Orthod. 2015;16:33. [68] GUILLEMINAULT C, QUO S, HUYNH NT. Orthodontic Expansion Treatment and Adenotonsillectomy in the Treatment of Obstructive Sleep Apnea in Prepubertal Children. Sleep. 2008;31(7):953-957. [69] CAPPELLETTE M JR, NAGAI LHY, GONÇALVES RM, et al. Impact of rapid maxillary expansion on nasomaxillary complex volume in mouth-breathers. Dental Press J Orthod. 2017;22(3):79-88. [70] MACARI AT, ZIADE G, KHANDAKJI M, et al. Effect of rapid maxillary expansion on voice. J Voice. 2016,30(6):760.e1-760.e6. [71] BILGIÇ F, DAMLAR İ, SÜRMELIOĞLU Ö, et al. Relationship between voice function and skeletal effects of rapid maxillary expansion. Angle Orthod. 2018;88(2):202-207. |
| [1] | Pu Rui, Chen Ziyang, Yuan Lingyan. Characteristics and effects of exosomes from different cell sources in cardioprotection [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(在线): 1-. |
| [2] | Zhang Chao, Lü Xin. Heterotopic ossification after acetabular fracture fixation: risk factors, prevention and treatment progress [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1434-1439. |
| [3] | Zhou Jihui, Li Xinzhi, Zhou You, Huang Wei, Chen Wenyao. Multiple problems in the selection of implants for patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1440-1445. |
| [4] | Wang Debin, Bi Zhenggang. Related problems in anatomy mechanics, injury characteristics, fixed repair and three-dimensional technology application for olecranon fracture-dislocations [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1446-1451. |
| [5] | Liu Yafei, Wang Yalin, Zuo Yanping, Sun Qi, Wei Jing, Zhao Lixia. Structural changes of the temporomandibular joint in adolescents with skeletal Class III malocclusions after maxillary protraction: an X-ray measurement analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1154-1159. |
| [6] | Wu Xun, Meng Juanhong, Zhang Jianyun, Wang Liang. Concentrated growth factors in the repair of a full-thickness condylar cartilage defect in a rabbit [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1166-1171. |
| [7] | Ji Zhixiang, Lan Changgong. Polymorphism of urate transporter in gout and its correlation with gout treatment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1290-1298. |
| [8] | Yuan Mei, Zhang Xinxin, Guo Yisha, Bi Xia. Diagnostic potential of circulating microRNA in vascular cognitive impairment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1299-1304. |
| [9] | Wang Xianyao, Guan Yalin, Liu Zhongshan. Strategies for improving the therapeutic efficacy of mesenchymal stem cells in the treatment of nonhealing wounds [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1081-1087. |
| [10] | Wan Ran, Shi Xu, Liu Jingsong, Wang Yansong. Research progress in the treatment of spinal cord injury with mesenchymal stem cell secretome [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1088-1095. |
| [11] | Liao Chengcheng, An Jiaxing, Tan Zhangxue, Wang Qian, Liu Jianguo. Therapeutic target and application prospects of oral squamous cell carcinoma stem cells [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1096-1103. |
| [12] | Zhao Min, Feng Liuxiang, Chen Yao, Gu Xia, Wang Pingyi, Li Yimei, Li Wenhua. Exosomes as a disease marker under hypoxic conditions [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1104-1108. |
| [13] | Xie Wenjia, Xia Tianjiao, Zhou Qingyun, Liu Yujia, Gu Xiaoping. Role of microglia-mediated neuronal injury in neurodegenerative diseases [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1109-1115. |
| [14] | Li Shanshan, Guo Xiaoxiao, You Ran, Yang Xiufen, Zhao Lu, Chen Xi, Wang Yanling. Photoreceptor cell replacement therapy for retinal degeneration diseases [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1116-1121. |
| [15] | Jiao Hui, Zhang Yining, Song Yuqing, Lin Yu, Wang Xiuli. Advances in research and application of breast cancer organoids [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1122-1128. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||