Chinese Journal of Tissue Engineering Research ›› 2020, Vol. 24 ›› Issue (10): 1477-1483.doi: 10.3969/j.issn.2095-4344.2201
Relationship between thoracic and lumbar vertebral posterior wall morphology and bone cement leakage into the spinal canal during the percutaneous kyphoplasty
Zhang Shuai, Wang Gaoju, Wang Qing
- Department of Spinal Surgery, the Affiliated Hospital of Southwest Medical University, Luzhou 646000, Sichuan Province, China
-
Received:2019-06-13Revised:2019-06-14Accepted:2019-07-20Online:2020-04-08Published:2020-02-14 -
Contact:Wang Qing, Professor, Department of Spinal Surgery, the Affiliated Hospital of Southwest Medical University, Luzhou 646000, Sichuan Province, China -
About author:Zhang Shuai, Master, Attending physician, Department of Spinal Surgery, the Affiliated Hospital of Southwest Medical University, Luzhou 646000, Sichuan Province, China
CLC Number:
Cite this article
Zhang Shuai, Wang Gaoju, Wang Qing. Relationship between thoracic and lumbar vertebral posterior wall morphology and bone cement leakage into the spinal canal during the percutaneous kyphoplasty[J]. Chinese Journal of Tissue Engineering Research, 2020, 24(10): 1477-1483.
share this article
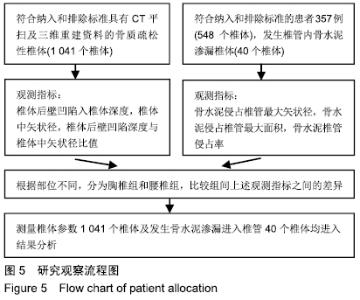
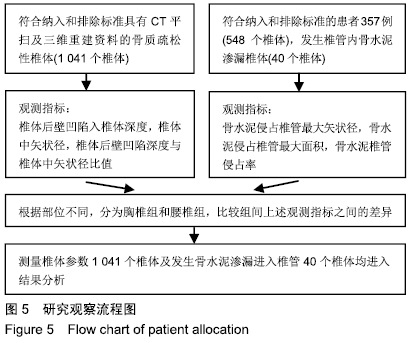
2.1 受试者数量分析 椎体后壁形态参数测量纳入病例98例共计1 176个椎体,其中陈旧性骨折T6为2个,T7为5个,T8为2个,T9为1个,T10为1个,T11为2个,T12为4个,L1为6个,L2为5个,L3为2个,L4为1个;新鲜骨折T6为2个,T7为3个,T8为6个,T9为3个,T10为7个,T11为6个,T12为14个,L1为22个,L2为21个,L3为7个,L4为7个,L5为6个;实际测量1 041个椎体。 在98例患者行PKP手术治疗,但测量时为避免骨水泥干扰,测量的椎体是该类患者的非骨折椎体,排除了行PKP治疗椎体,所以应该测量椎体总数为1 176个,但实际测量的是1 041个。 同期行PKP手术治疗OVCF患者357例(548个椎体)发生椎管内骨水泥渗漏40个,胸椎组31个,腰椎组9个,40个均进入结果分析。研究观察流程见图5。 "
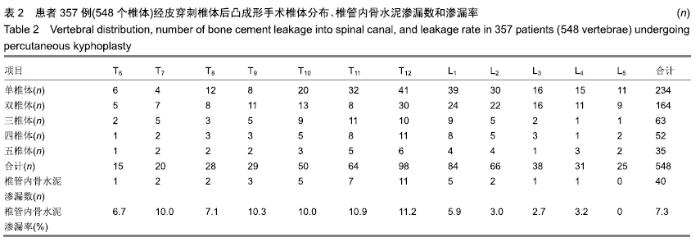
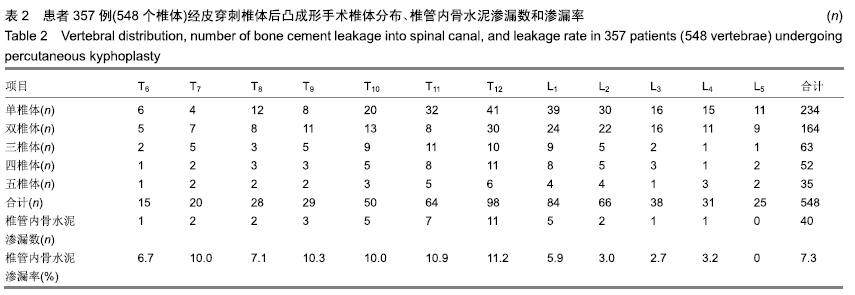
2.2 患者基线分析 进行椎体后壁形态测量的98例OVCF患者,其中男31例,女67例,年龄58-89岁(71.6±1.2岁),骨密度-1.4至-5.8 SD (-3.2±0.4) SD。 骨水泥渗漏侵占椎管程度测量纳入357例均为汉族,其中男132例,女225例,年龄55-94岁(72.6±1.4)岁,病程1 d-10个月,平均(33.8±2.1) d,357例患者行PKP手术胸椎304个,腰椎244个,具体手术部位分布见表2;术中单个椎体骨水泥注入量胸椎组2.5-6.0 (4.2±0.2) mL,腰椎组3.5-7.5(5.1±0.5) mL。 "
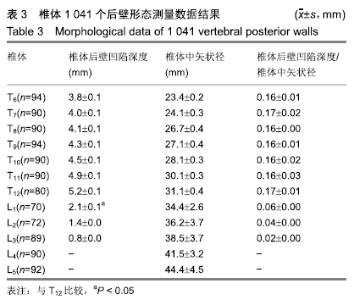
2.3 影像学参数测量结果 患者198例胸、腰椎椎体后壁形态相关参数:椎体后壁凹陷入椎体实质深度在T6-T12逐渐加深,L1-L5逐渐变浅,椎体中矢状径在T6-L5逐渐大,两者比值在T6-T12服从正态分布,在T6-T12均为0.16(1/6)左右,腰椎较胸椎明显减小,在L1-L3明显小于1/6,在L4、L5接近于0,见表3。 "

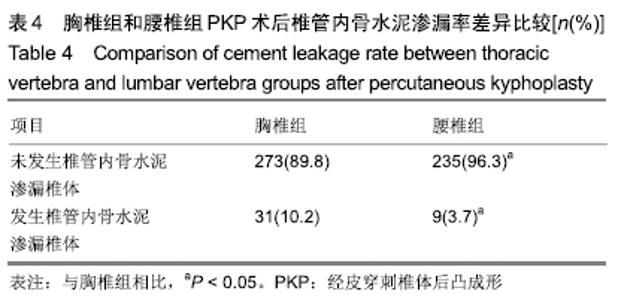
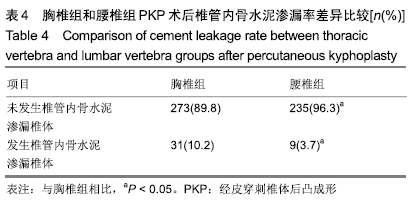
患者357例行PKP术发生椎管内骨水泥渗漏参数测量结果:手术椎体548个,其中胸椎304个,发生骨水泥椎管内渗漏31个,渗漏率为10.2%;腰椎244个,发生椎管内骨水泥渗漏9个,渗漏率为3.7%,胸椎发生椎管内骨水泥渗漏率明显大于腰椎(P < 0.05),见表2,4。胸椎组骨水泥侵占椎管最大矢状径、侵占椎管面积及椎管侵占率明显大于腰椎组(P < 0.05),见表5。 "

"

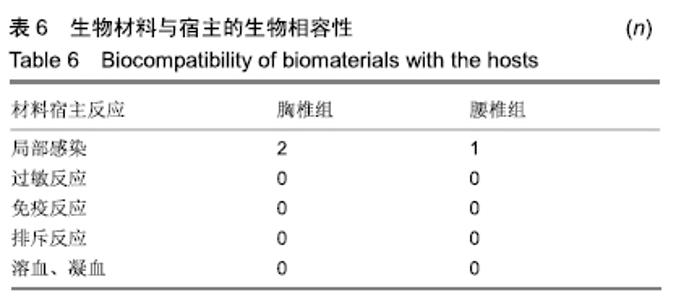
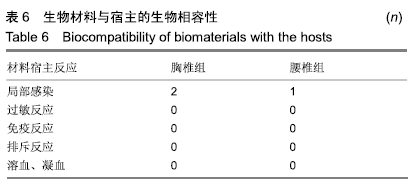
2.4 生物相容性评价 见表6。 "
| [1] KARMAKAR A, ACHARYA S, BISWAS D, et al. Evaluation of percutaneous vertebroplasty for management of symptomatic osteoporotic compression fracture. J Clin Diagn Res. 2017;11(8): RC07-RC10. [2] LIEBERMAN IH, DUDENEY S, REINHARDT M K, et al. Initial outcome and efficacy of "kyphoplasty" in the treatment of painful osteoporotic vertebral compression fractures. Spine. 2001;26(14): 1631-1638. [3] KAN SL, YUAN ZF, CHEN LX, et al. Which is best for osteoporotic vertebral compression fractures: balloon kyphoplasty, percutaneous vertebroplasty or non-surgical treatment? A study protocol for a Bayesian network meta-analysis. BMJ Open. 2017; 7(1):E012937-E012941. [4] PHILLIPS FM, HO E, CAMPBELLHUPP M, et al. Early radiographic and clinical results of balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Spine; 2003,28(19):2265-2267. [5] MA XL, XING D, MA JX, et al. Balloon kyphoplasty versus percutaneous vertebroplasty in treating osteoporotic vertebral compression fracture:grading the evidence through a systematic review and meta-analysis. Eur Spine J. 2012;21(9):1844-1859. [6] 周宏斌,秦小容,屈万明,等.不同方法治疗老年骨质疏松性椎体压缩骨折的临床疗效分析[J].重庆医学,2016,26(6):802-804. [7] 李惠民,陈银河,申才良.经皮椎体后凸成形术治疗骨质疏松性椎体压缩骨折远期并发症的Meta分析[J].中国脊柱脊髓杂志,2017,29(7): 718-722. [8] 王松,杨剑,杨函,等.侧卧位单侧经横突-椎弓根入路椎体后凸成形术治疗骨质疏松性椎体压缩骨折的疗效[J].实用医学杂志,2017, 33(33):3905-3909. [9] ZHAN Y, JIANG J, LIAO H, et al. Risk factors for cement leakage after vertebroplasty or kyphoplasty: a meta-analysis of published evidence. World Neurosurg. 2017;101(6):633-642. [10] YEOM JS, KIM WJ, CHOY WS, et al. Leakage of cement in percutaneous transpedicular vertebroplasty for painful osteoporotic compression fractures. J Bone Joint Surg Br. 2003;85(1):83-89. [11] GARFIN SR, YUAN HA, REILEY MA. New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine(Phila Pa1976). 2001; 26(14):1511-1515. [12] SHAWKY A, EZZATI A, GOVINDASAMY R, et al. Kyphoplasty for osteoporotic vertebral fractures with posterior wall injury. Spine J. 2017;18(7):1143-1148. [13] SUN K, LIU Y, PENG H, et al. A comparative study of high-viscosity cement percutaneous vertebroplasty vs. low-viscosity cement percutaneous kyphoplasty for treatment of osteoporotic vertebral compression fractures. J Huazhong Univ Sci Technolog Med Sci. 2016;36(3):389-394. [14] LIU T, LI Z, SU Q, et al. Cement leakage in osteoporotic vertebral compression fractures with cortical defect using high-viscosity bone cement during unilateral percutaneous kyphoplasty surgery. Medicine. 2017;96(25):E7216-E7221. [15] JIACHEN L, LIE Q, CHANGQING J, et al. Bone cement distribution is a potential predictor to the reconstructive effects of unilateral percutaneous kyphoplasty in OVCFs: a retrospective study. J Orthop Surg Res. 2018;13(1):140-146. [16] CHEN H, TANG P, ZHAO Y, et al. Unilateral versus bilateral balloon kyphoplasty in the treatment of osteoporotic vertebral compression fractures. Orthopedics. 2014;37(9):e828-e835. [17] NIEUWENHUIJSE MJ, VAN ERKEL AR, DIJKSTRA PD. Cement leakage in percutaneous vertebroplasty for osteoporotic vertebral compression fractures: identification of risk factors. Spine J. 2011; 11(9):839-848. [18] HARRINGTON KD. Major neurological complications following percutaneous vertebroplasty with polymethylmethacrylate: a case report. J Bone Joint Surg Am. 2001;83-A(7):1070-1073. [19] CHEN J, CHEN Y, ZHANG Z S, et al. Retrospective analysis of cement leakage in percutaneous kyphoplasty for osteoporotic vertebral compression fractures. Medicine. 2019,98(10): e14793-e14798. [20] DING J, ZHANG Q, ZHU J, et al. Risk factors for predicting cement leakage following percutaneous vertebroplasty for osteoporotic vertebral compression fractures. Eur Spine J. 2016;25(11):3411-3417. [21] GAO C, ZONG M, WANG WT, et al. Analysis of risk factors causing short-term cement leakages and long-term complications after percutaneous kyphoplasty for osteoporotic vertebral compression fractures. Acta Radiol. 2018;59(5):577-585. [22] ZHAN Y, JIANG J, LIAO H, et al. Risk factors for cement leakage after vertebroplasty or kyphoplasty: a meta-analysis of published evidence. World Neurosurg. 2017;101(5):633-642. [23] KAUR K, SINGH R, PRASATH V, et al. Computed tomographic-based morphometric study of thoracic spine and its relevance to anaesthetic and spinal surgical procedures. J Clin Orthop Trauma. 2016;7(2):101-108. [24] TAN SH, TEO EC, CHUA HC. Quantitative three-dimensional anatomy of cervical, thoracic and lumbar vertebrae of Chinese Singaporeans. Eur Spine J. 2004;13(2):137-146. [25] SCOLES PV, LINTON AE, LATIMER B, et al. Vertebral body and posterior element morphology: the normal spine in middle life. Spine.1988;13(10):1082-1086. [26] GOUZIEN P, CAZALBOU C, BOYER B, et al. Measurements of the normal lumbar spinal canal by computed tomography. Surg Radiol Anat. 1990;12(2):143-148. [27] RAPAŁA K, CHABEREK S, TRUSZCZYŃSKA A, et al. Assessment of lumbar spinal canal morphology with digital computed tomography. Ortop Traumatol Rehabil. 2009;11(2): 156-163. [28] 王高举,谢胜荣,杨进,等.老年骨质疏松性椎体压缩骨折和中青年胸腰椎骨折患者椎弓根宽度的CT观察[J].中国脊柱脊髓杂志,2016, 26(12):1076-1081. [29] RYU KS, PARK CK, KIM MK, et al. Single balloon kyphoplasty using far-lateral extrapedicular approach: technical note and preliminary results. J Spinal Disord Tech. 2007;20(5):392-398. [30] WANG S, WANG Q, KANG J, et al. An imaging anatomical study on percutaneous kyphoplasty for lumbar via a unilateral transverse process-pedicle approach. Spine (Phila Pa 1976). 2014;39(9):701-706. [31] 杨惠林,刘强,唐海,等.经皮椎体后凸成形术的规范化操作及相关问题的专家共识[J].中华医学杂志,2018,98(11):808-812. [32] HEINI P, ORLER R. Kyphoplasty for treatment of osteoporotic vertebral fractures. Eur Spine J. 2004;13(3):184-192. [33] BELKOFF SM, MARONEY M, FENTON DC, et al. An in vitro biomechanical evaluation of bone cements used in percutaneous vertebroplast. Bone. 1999;25(2 Suppl):23S-26S. [34] REBOLLEDO BJ, GLADNICK BP, UNNANUNTANA A, et al. Comparison of unipedicular and bipedicular balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures a prospective randomised study. Bone Joint J. 2013;11(3): 401-406. [35] SONG BK, EUN JP, OH YM. Clinical and radiological comparison of unipedicular versus bipedicular balloon kyphoplasty for the treatment of vertebral compression fractures. Osteoporosis Int. 2009;20(10):1717-1723. |
| [1] | Liu Yulin, Li Guotai. Combined effects of hyperbaric oxygen, vibration training and astaxanthin on bone mineral density, glucose metabolism and oxidative stress in diabetic osteoporosis rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(20): 3117-3124. |
| [2] | Lin Haishan, Mieralimu Muertizha, Li Peng, Ma Chao, Wang Li. Correlation between skeletal muscle fiber characteristics and bone mineral density in postmenopausal women with hip fractures [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(20): 3144-3149. |
| [3] | Chen Jiayun, Li Anan, Lü Zhaohui, Wu Zixuan, Cai Minjie, Huang Xuyan . Effect of long-term use of proton pump inhibitors on bone mineral density and bone metabolism: a Meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(17): 2775-2780. |
| [4] | Liu Zhijun, Liu Shaojin, Wei Hewei, Wan Lei, Huang Hongxing, Qiao Rongqin. Effect of Bushen Jianpi Huoxue Recipe on transforming growth factor beta/bone morphogenetic protein 2 signaling pathway in the muscle and skeleton of ovariectomized rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(14): 2219-2223. |
| [5] | Chen Zegang, Ding Haili, Li Long, Wang Chun. Changes of bone metabolism after different intensity endurance exercises in growing rats [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(35): 5582-5588. |
| [6] | He Li, Liu Zhai, Gao Zhimei, Liu Chunying, Zhao Junlu, Ren Qingyun. Radiomics for diagnostic value of osteoporosis in female patients based on lumbar magnetic resonance imaging [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(30): 4841-4846. |
| [7] | Zhao Zhonghai, Yan Tong, Li Hongqiu, Pan Hai. Systematic review and meta-analysis on the effect of resistance training on bone mineral density in postmenopausal women with osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(30): 4914-4920. |
| [8] |
Ye Yunjin, Li Jianyang, Ge Jirong, Xu Huijuan, Chen Sainan, Xie Lihua, Li Li.
Combination of hip geometry mechanics and fracture risk assessment tool to predict fracture risk in middle-aged and elderly women [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(26): 4101-4105. |
| [9] | Li Kaiming, Zhu Liguo, Zhang Qing, Li Linghui, Xie Rui, Chen Ming, Liang Long, Lin Chengyu, Hou Xiaozhou. Zolidronic acid combined with percutaneous kyphoplasty in the treatment of osteoporotic compression fractures: a meta-analysis of bone density improvement, recurrent vertebral fractures prevention, and long-term efficacy evaluation [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(24): 3911-3917. |
| [10] | Zhao Jing, Yin Lian, Lei Xuemei, Li Miaomiao, Wang Kun, Zhang Tingran, Luo Jiong. KAASTU training for muscle fitness in the middle-aged and elderly adults: effects and strengths [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(23): 3737-3743. |
| [11] | Qian Guang, Yu Yueming, Dong Youhai, Hong Yang, Wang Minghai. Pulsed electromagnetic fields stimulation combined with sclerostin antibody improves bone metabolism and bone microstructure in postmenopausal osteoporosis rabbits [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(20): 3130-3134. |
| [12] | Qi Yusen, Han Mengguang, Luo Jinwei, Guan Chenwei, Hu Jiayang, Xu Cong, Lü Yongming. Arthroscopic repair for osteoporosis in the greater tuberosity of patients with rotator cuff tear due to chronic moderate to severe tendon retraction [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(20): 3140-3145. |
| [13] | Zhao Jing. Effects of Tai Chi Chuan on the changes of bone mineral density of perimenopausal women [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(2): 176-180. |
| [14] | Yang Xiaoye, Li Wenjin, Zhu Li, Wang Yu, Zhang Shuangyuan. Changes of bone mineral density and related factors during maxillary teeth occlusion after tooth extraction in diabetic mice [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(2): 242-247. |
| [15] | Cen Zhuohao, Chen Jiena, Huang Jiahua, Shi Chushuo, Zhou Chi, Wen Junmao, Ling Min. Acupuncture combined with other therapies for osteoporosis: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(2): 320-328. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||