Chinese Journal of Tissue Engineering Research ›› 2013, Vol. 17 ›› Issue (40): 7163-7168.doi: 10.3969/j.issn.2095-4344.2013.40.022
Previous Articles Next Articles
Complications and risk factors after allogeneic hematopoietic stem cell transplantation
Guo Zhi, Chen Hui-ren
- Department of Hematology, General Hospital of Beijing Military Region, Beijing 100700, China
-
Online:2013-10-01Published:2013-10-31 -
About author:Guo Zhi★, Master, Associate chief physician, Department of Hematology, General Hospital of Beijing Military Region, Beijing 100700, China Guozhi02@163.com -
Supported by:the National Natural Science Foundation of China, No. 31200686*
CLC Number:
Cite this article
Guo Zhi, Chen Hui-ren. Complications and risk factors after allogeneic hematopoietic stem cell transplantation[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(40): 7163-7168.
share this article

2.1 异基因造血干细胞移植后肺部并发症 异基因造血干细胞移植后有40%-60%的患者出现肺部并发症,其中有10%-40%的患者因肺部并发症而死亡。特发性肺炎综合征和侵袭性霉菌感染是异基因造血干细胞移植后常见的肺部并发症。1998年,Palmas等[3]首先提出迟发性非感染性肺部并发症的概念,是异基因造血干细胞移植后晚期肺部并发症,发生率在3.0%-23.7%,发病中位时间为七八个月,导致患者死亡的主要原因是进行性呼吸衰竭及继发肺部感染[4]。迟发性非感染性肺部并发症的发病机制可能与预处理过程中使用的放射线、细胞毒性药物、免疫抑制剂以及慢性移植物抗宿主病的预防有关。近年来关于异基因造血干细胞移植后肺部并发症的发生率及治疗,见表1。"
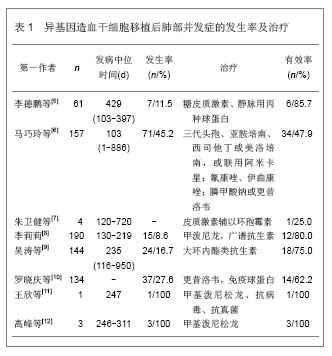
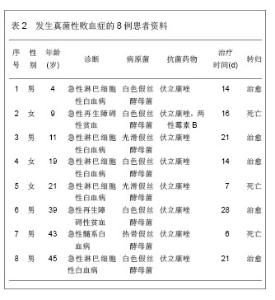
异基因造血干细胞移植后相关并发症的发生与多种因素有关[13]。马巧玲等[6]研究异基因造血干细胞移植后发生肺部并发症的危险因素。肺部并发症以细菌性肺炎和间质性肺炎居多,主要的病原体为金黄色葡萄球菌、粪肠球菌、表皮葡萄球菌、铜绿假单孢菌和肺炎克雷白杆菌等。单因素分析肺部并发症的危险,患者年龄、疾病状态、供受者关系、人类白细胞抗原配型相合程度及广泛型慢性移植物抗宿主病是影响移植后肺部并发症的危险因素。多因素分析显示疾病状态和广泛型移植物抗宿主病与肺部并发症的发生显著相关。李莉莉[8]研究异基因造血干细胞移植后发生特发性肺炎综合征的危险因素,原发症为慢性粒细胞白血病和急性移植物抗宿主病与特发性肺炎综合征的发生有关,移植后死亡率较高。异基因造血干细胞移植后发生侵袭性霉菌感染的危险因素,移植物抗宿主病的激素治疗和巨细胞病毒血症是侵袭性霉菌感染发生的危险因素。吴涛等[9]单因素分析研究显示,迟发性非感染性肺部并发症的发生与巨细胞病毒抗原血症、急性移植物抗宿主病、慢性移植物抗宿主病相关,多因素分析显示与慢性移植物抗宿主病和巨细胞病毒抗原血症相关。 2.2 异基因造血干细胞移植后真菌性败血症 异基因造血干细胞移植后发生真菌性败血症的情况越来越多,是目前严重并发症之一,可以导致患者死亡。由于移植前进行大剂量的放疗和化疗,使患者的免疫功能低下,发生真菌性败血症的危险显著提升[14]。同时,真菌感染与移植后严重的移植物抗宿主病、移植前患者有真菌感染史或处于感染状态、强烈的预处理方案、非血缘造血干细胞移植及供受者人类白细胞抗原不相合等存在明显的相关性[15]。作者回顾分析140例异基因造血干细胞移植患者,急性髓系白血病62例,急性淋巴细胞性白血病30例,急性再生障碍性贫血22例,骨髓增生异常综合征20例,淋巴瘤4例,多发性骨髓瘤2例,亲缘供者移植135例,非亲缘供者移植5例。供受者人类白细胞抗原全相合80例,1个位点不合18例,2个位点不合12例,3个位点不合30例。全相合造血干细胞移植采用改良的白消安加环磷酰胺方案:阿糖胞苷4 g/m2×2 d,静脉滴注;白消安4 mg/(kg•d)× 3 d,口服;环磷酰胺1.8 g/(m2•d),静脉滴注;甲基环已亚硝脲250 mg/m2×1 d,口服。人类白细胞抗原不相合造血干细胞移植,预处理方案为氟达拉滨替代环磷酰胺的改良的白消安加环磷酰胺方案:阿糖胞苷 4 g/m2×2 d,静脉滴注;白消安4 mg/(kg•d)×3 d,口服;氟达拉滨40 mg/(m2•d)×5 d,静脉滴注;甲基环已亚硝脲250 mg/m2×1 d,口服。移植物抗宿主病的预防采用经典的环孢素A加短程甲氨蝶呤,加用霉酚酸酯及抗人胸腺细胞球蛋白预防。移植前有真菌感染阳性的患者继续维持原抗真菌药物治疗,常用伏立康唑、伊曲康唑、两性霉素B和卡泊芬净,移植后给予伏立康唑注射液4 mg/( kg•次),2次/d静脉滴注。于移植方案开始时或开始后48 h内给药,直至患者的中性粒细胞恢复至> 0.5×109 L-1停药,给药时间≤28 d。给予患者支持治疗,中性粒细胞数<0.5×109 L-1时使用粒细胞集落刺激因子刺激造血,血小板<20×109 L-1时输注血小板,血红蛋白<80 g/L时输注悬浮红细胞等对症支持治疗,适当输注免疫球蛋白预防感染,若出现发热发感染征象给予亚胺培南或美罗培南等经验性抗感染,同时积极查找感染灶及微生物证据。结果8例患者血培养真菌阳性,发生率为5.7%,发生时间在7-32 d,平均(20.1±3.1) d,共培养出真菌8株,5株白色假丝酵母菌,2株光滑假丝酵母菌,1株热带假丝酵母菌,药敏试验发现对伏立康唑、伊曲康唑、两性霉素B和卡泊芬净等常用抗真菌药均敏感。8例患者发生真菌性败血症的资料,见表2。"
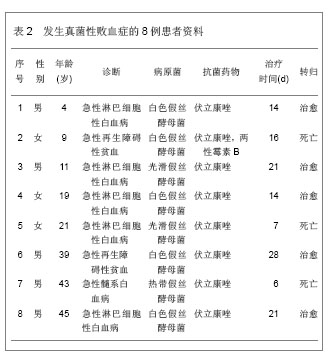

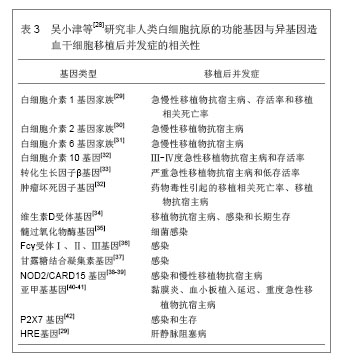
3例患者死亡,死亡率为37.5%,其中1例患者于移植后32 d出现真菌性败血症,合并肺部真菌感染,先后经伏立康唑、两性霉素B等药物治疗,病情未得到控制,于48 d死于呼吸衰竭;另2例患者分别在12,15 d血培养阳性,发生真菌性败血症后应用伏立康唑,但于19,21 d死亡原因均为感染性休克。 2.3 异基因造血干细胞移植后巨细胞病毒感染 巨细胞病毒是一种特异性的DNA病毒,是已知人类疱疹病毒中最大的一组病毒。在异基因造血干细胞移植的过程中,由于移植的预处理,应用大量化疗和免疫抑制药物,使患者的免疫功能严重受损,巨细胞病毒被激活[16]。巨细胞病毒感染与移植物抗宿主病有一定的相关性,巨细胞病毒可以引起移植物抗宿主病,同时,移植物抗宿主病也会引起巨细胞病毒感染[17]。巨细胞病毒是异基因造血干细胞移植后常见合并症,是导致患者死亡的主要原因之一[18]。作者选取2010年1月至2012年1月在解放军北京军区总医院血液科行异基因造血干细胞移植的患者140例进行巨细胞病毒感染的实验研究[19]。,包括38例急性髓系白血病患者,52例急性淋巴细胞白血病患者,18例慢性髓系白血病患者,6例淋巴瘤患者,18例再生障碍性贫血患者,8例多发性骨髓癌患者,供受者人类白细胞抗原全相合造血干细胞移植95例,人类白细胞抗原不相合造血干细胞移植45例。骨髓与外周血单个核细胞采集,供者接受粒细胞集落刺激因子动员,剂量为5-10 μg/( kg•d),连续皮下四五天。移植方法采用骨髓加外周血单个核细胞联合移植,第4天在硬膜外麻醉下从髂后上棘采集骨髓,第5天采集外周血单个核细胞,两者总和单个核细胞数在5×108/kg以上。对于人类白细胞抗原相合的造血干细胞移植主要采用改良BUCY方案,不合相的造血干细胞移植采用氟达拉滨替代环磷酰胺的改良BUCY方案。对人类白细胞抗原不相合造血干细胞移植主要采用氟达拉滨替代环磷酰胺的改良BUCY方案。联合使用多种免疫抑制剂预防移植物抗宿主病,在经典的环孢素A加短程甲氨蝶呤方案基础上,再加用霉酚酸酯及抗人胸腺细胞球蛋白预防移植物抗宿主病。移植前全部患者经查巨细胞病毒-DNA均为阴性,所有患者于移植后开始给予阿昔洛韦注射液4 mg/kg,2次/d。移植后1个月改为阿昔洛韦口服直至3个月,每周行巨细胞病毒-DNA检查,出现巨细胞病毒-DNA阳性给予更昔洛韦或者膦甲酸钠静脉滴注,直至巨细胞病毒-DNA转阴。 移植疗效:移植后中位随访时间为13.5个月,随访12个月以上者84例。140例患者中,存活93例,死亡47例,其中早期死亡12例,晚期死亡35例。发生急性移植物抗宿主病45例;死亡17例;复发死亡16例,2年生存率为66.4%。 巨细胞病毒感染情况:140例患者移植后共有48例发生巨细胞病毒感染,占34.3%,首次检出巨细胞病毒-DNA阳性中位时间是移植后大约45 d,定量范围为1.25×103-5.5×106。全部巨细胞病毒感染患者中7例进展为巨细胞病毒疾病,占14.6%,2例为巨细胞病毒相关性间质性肺炎,胸部X射线片示肺间质改变,5例为巨细胞病毒相关性出血性膀胱炎。巨细胞病毒- DNA阳性的患者给予更昔洛韦或者膦甲酸钠静滴直至巨细胞病毒-DNA转阴,全部患者经过大约45 d治疗后巨细胞病毒-DNA转阴,有效率为100%。 移植物抗宿主病与巨细胞病毒感染:发生急性移植物抗宿主病的45例患者中,合并巨细胞病毒感染20例;发生慢性移植物抗宿主病20例,合并巨细胞病毒感染12例。共有65例患者发生移植物抗宿主病,合并巨细胞病毒感染总计32例,占49.2%。未发生移植物抗宿主病患者有75例,发生巨细胞病毒感染16例,占21.3%,显著低于移植物抗宿主病患者组。 抗病毒药不良反应:更昔洛韦最常见的不良反应为骨髓抑制,其中以白细胞下降最常见,其次为血小板。作者研究中共有12例患者治疗过程中出现一过性的白细胞和血小板减少,但停药后数天便自行恢复,未观察至心、肝、肾功能的损害。服用磷甲酸钠偶见不良反应为肾损害及电解质紊乱,但发生率低,停药对症处理后可恢复正常。 异基因造血干细胞移植后发生巨细胞病毒感染的相关报道。2009年,Kekik等[20]人类白细胞抗原等位基因可以有1个巨细胞病毒激活保护或诱发作用,为急性移植物抗宿主病的风险评估和设计个性化治疗提供依据。2011年,Ruiz-Camps等[21]在异基因造血干细胞移植的第1年,有超过50%的患者会有巨细胞病毒感染或再激活。2011年,Ichihara等[22]巨细胞病毒感染可以造成造血功能重建延迟,抑制造血细胞增殖和分化,造成移植物不能存活。2012年,Jang等[23]最初的白细胞减少是进展为巨细胞病毒感染的最显著危险因素。 2.4 异基因造血干细胞移植后中枢神经系统并发症 关于异基因造血干细胞移植后发生中枢神经系统并发症的报道相对较少。吴穗晶等[24]回顾性分析95例异基因造血干细胞移植患者,有7例出现中枢神经系统并发症。预处理方案为白消安/环磷酰胺或全身照射/环磷酰胺。全相合的同胞移植、脐血移植采用环孢素、甲氨蝶呤、霉酚酸酯。不相合的同胞移植、无关移植、单倍型相合骨髓移植加抗胸腺细胞球蛋白。7例患者年龄在12-46岁,女5例,男2例,诊断为慢性髓性白血病慢性期3例,骨髓增生异常综合征2例,急性淋巴细胞白血病首次完全缓解1例,白血病M5b-CR3期1例。同胞全相合2例,同胞5/6相合1例,脐血5/6相合1例,单倍型5/6相合2例,无关8/10相合1例。中枢神经系统并发症发生时间45-100 d,症状为肌力下降昏迷1例,肌力视力下降1例,抽搐语言不清1例,抽搐神志模糊2例,抽搐迅速昏迷2例。CT、MRI、MRA检查阳性3例。分析可能的病因,感染2例,脑病2例,脑梗死2例,脑出血1例。预防中枢神经系统并发症的方法包括在移植前行腰穿检查并鞘内注射甲氨蝶呤或阿糖胞苷;应用白消安预处理后给予预防癫痫治疗;定期检测环孢素、他克莫司的浓度;定期检测巨细胞病素抗原,应用更昔洛韦预防病毒感染,氟康唑或伊曲康唑预防真菌感染。经预防和治疗后存活4例,死亡3例。韩利杰等[25]观察68例异基因造血干细胞移植患者中枢神经系统并发症的发生情况及特点,并分析其原因和高危因素。69例患者异基因造血干细胞移植后6个月内8例发生中枢神经系统并发症,发生率11.6%。其中在人类白细胞抗原全相合及不全相合组分别为4.9%(2/41)和21.4%(6/28),移植物抗宿主病≤2度和>2度组分别为6.7%(4/9)、44.4%(4/60)。异基因造血干细胞移植最常见的中枢神经系统并发症是癫痫和颅内感染,其次为颅内出血。异基因造血干细胞移植中人类白细胞抗原配型不全相合和发生移植物抗宿主病>2度均是发生中枢神经系统并发症的高危因素。 2.5 非因素多态性与异基因造血干细胞移植后并发症 放疗和化疗过程中释放的白细胞介素1细胞、白细胞介素6细胞、白细胞介素8细胞和肿瘤坏死因子α等细胞因子能够激活抗原呈递细胞,诱导供者T细胞的激活,上调受者人类白细胞抗原和黏附分子的表达等,会造成移植物抗宿主病的发生[26-27]。非人类白细胞抗原的功能基因单核苷酸多态性与异基因造血干细胞移植后并发症的相关性研究,见表3。"
| [1]Medline.Pubmed[DB/OL].2013-08-21.http://www.ncbi.nlm.nih. gov/pubmed/ [2]中国知网.中国学术期刊总库[DB/OL].2013-08-21. https://www.cnki.net [3]Palmas A, Tefferi A, Myers JL, et al.Late-onset noninfectious pulmonary complications after allogeneic bone marrow transplantation.Br J Haematol. 1998;100(4):680-687. [4]Sakaida E, Nakaseko C, Harima A, et al.Late-onset noninfectious pulmonary complications after allogeneic stem cell transplantation are significantly associated with chronic graft-versus-host disease and with the graft-versus-leukemia effect.Blood.2003;102(12):4236-4242. [5]李德鹏,程海,李振宇,等.异基因造血干细胞移植后迟发性非感染性肺部并发症7例并文献复习[J].徐州医学院学报,2012,32(11): 749-751. [6]马巧玲,冯四洲,王枚,等.异基因造血干细胞移植后肺部并发症的发生和危险因素分析[J].生物医学工程与临床,2007,11(2): 129-133. [7]朱卫健,王玫玫,杜均祥,等.异基因造血干细胞移植后迟发性非感染肺部并发症4例分析[J].广东医学,2011,32(5):600-601. [8]李莉莉.异基因造血干细胞移植术后肺部并发症研究[D].上海:第二军医大学,2011:1-3. [9]吴涛,刘启发,张钰,等.异基因造血干细胞移植后迟发性非感染性肺部并发症的发生和危险因素分析[J].中华血液学杂志,2010, 31(4):249-252. [10]罗晓庆,张曦,陈幸华,等.异基因造血干细胞移植后肺部并发症的临床观察[J].重庆医学,2010,39(14):1846-1847. [11]王欣,刘林,陈建斌,等.异基因造血干细胞移植后迟发性非感染性肺部并发症1例报道及文献复习[J].重庆医学,2009,38(14): 1755-1757. [12]高峰,李小宇,朱梦波,等.异基因造血干细胞移植术后迟发性非感染性肺部并发症三例[J].白血病•淋巴瘤,2008,17(3):210-212. [13]Tabbara IA, Zimmerman K, Morgan C, et al.Allogeneic hematopoietic stem cell transplantation: complications and results.Arch Intern Med. 2002;162(14):1558-1566. [14]陈惠仁,何学鹏,杨凯,等.CD25抗体在单倍型干细胞移植后肠道急性GVHD治疗中的应用[J].中华医学杂志,2010,90(38): 2693-2696. [15]Petersdorf EW.HLA matching in allogeneic stem cell transplantation.Curr Opin Hematol. 2004;11(6):386-391. [16]Ruiz-Camps I, Len O, de la Cámara R, et al.Valganciclovir as pre-emptive therapy for cytomegalovirus infection in allogeneic haematopoietic stem cell transplant recipients.Antivir Ther. 2011;16(7):951-957. [17]Cantoni N, Hirsch HH, Khanna N, et al.Evidence for a bidirectional relationship between cytomegalovirus replication and acute graft-versus-host disease.Biol Blood Marrow Transplant. 2010;16(9):1309-1314. [18]刘开彦.造血干细胞移植患者巨细胞病毒感染的诊治进展[J].中国实用内科杂志,2007,10(27):1597-1598. [19]郭智,陈惠仁,刘晓东,等.异基因造血干细胞移植后巨细胞病毒感染的临床分析[J].中国实验血液学杂志,2012,20(4):971-974. [20]Kekik C, Besisik SK, Seyhun Y, et al.Relationship between HLA tissue type, CMV infection, and acute graft-vs-host disease after allogeneic hematopoietic stem cell transplantation: single-center experience.Transplant Proc. 2009;41(9):3859-3862. [21]Ruiz-Camps I, Len O, de la Cámara R, et al.Valganciclovir as pre-emptive therapy for cytomegalovirus infection in allogeneic haematopoietic stem cell transplant recipients.Antivir Ther. 2011;16(7):951-957. [22]Ichihara H, Nakamae H, Hirose A, et al.Immunoglobulin prophylaxis against cytomegalovirus infection in patients at high risk of infection following allogeneic hematopoietic cell transplantation.Transplant Proc. 2011;43(10):3927-3932. [23]Jang JE, Hyun SY, Kim YD, et al.Risk factors for progression from cytomegalovirus viremia to cytomegalovirus disease after allogeneic hematopoietic stem cell transplantation.Biol Blood Marrow Transplant. 2012;18(6):881-886. [24]吴穗晶,杜欣,翁建宇,等.异基因造血干细胞移植后中枢神经系统并发症[J].中华血液学杂志,2008,27(8):572-573. [25]韩利杰,马红霞,董秀娟,等.异基因造血干细胞移植的中枢神经系统并发症危险因素分析[J].白血病•淋巴瘤,2012,21(11):671-674. [26]Hochberg EP, Miklos DB, Neuberg D, et al.A novel rapid single nucleotide polymorphism (SNP)-based method for assessment of hematopoietic chimerism after allogeneic stem cell transplantation.Blood. 2003;101(1):363-369. [27]Goussetis E, Varela I, Peristeri I, et al.Cytokine gene polymorphisms and graft-versus-host disease in children after matched sibling hematopoietic stem cell transplantation: a single-center experience.Cell Mol Immunol. 2011;8(3): 276-280. [28]吴小津,吴德沛.非HLA基因多态性与异基因造血干细胞移植后并发症发生[J].中华移植杂志:电子版,2010,4(1):60-64. [29]Kallianpur AR.Genomic screening and complications of hematopoietic stem cell transplantation: has the time come?Bone Marrow Transplant. 2005;35(1):1-16. [30]MacMillan ML, Radloff GA, Kiffmeyer WR, et al.High-producer interleukin-2 genotype increases risk for acute graft-versus-host disease after unrelated donor bone marrow transplantation.Transplantation. 2003;76(12):1758-1762. [31]Unfried G, Böcskör S, Endler G, et al.A polymorphism of the interleukin-6 gene promoter and idiopathic recurrent miscarriage.Hum Reprod. 2003;18(2):267-270. [32]Rocha V, Franco RF, Porcher R, et al.Host defense and inflammatory gene polymorphisms are associated with outcomes after HLA-identical sibling bone marrow transplantation.Blood.2002;100(12):3908-3918. [33]Berro M, Mayor NP, Maldonado-Torres H, et al.Association of functional polymorphisms of the transforming growth factor B1 gene with survival and graft-versus-host disease after unrelated donor hematopoietic stem cell transplantation.Haematologica. 2010;95(2):276-283. [34]Hattori H, Matsuzaki A, Suminoe A, et al.Polymorphisms of transforming growth factor-beta1 and transforming growth factor-beta1 type II receptor genes are associated with acute graft-versus-host disease in children with HLA-matched sibling bone marrow transplantation.Bone Marrow Transplant. 2002;30(10):665-671. [35]Bogunia-Kubik K, Middleton P, Norden J, et al.Association of vitamin D receptor polymorphisms with the outcome of allogeneic haematopoietic stem cell transplantation.Int J Immunogenet. 2008;35(3):207-213. [36]Zhong C, Quanzhong Y, Genshan M, et al.Myeloperoxidase gene-463G > A polymorphism and premature coronary artery disease.Genet Mol Biol. 2009;32(2):260-263. [37]Solomon S, Kassahn D, Illges H.The role of the complement and the Fc gamma R system in the pathogenesis of arthritis.Arthritis Res Ther. 2005;7(4):129-135. [38]Mullighan CG, Heatley SL, Danner S, et al.Mannose-binding lectin status is associated with risk of major infection following myeloablative sibling allogeneic hematopoietic stem cell transplantation.Blood. 2008;112(5):2120-2128. [39]Mayor NP, Shaw BE, Hughes DA, et al.Single nucleotide polymorphisms in the NOD2/CARD15 gene are associated with an increased risk of relapse and death for patients with acute leukemia after hematopoietic stem-cell transplantation with unrelated donors.J Clin Oncol. 2007;25(27):4262-4269. [40]Fishbein T, Novitskiy G, Mishra L, et al.NOD2-expressing bone marrow-derived cells appear to regulate epithelial innate immunity of the transplanted human small intestine.Gut. 2008;57(3):323-330. [41]Sugimoto K, Murata M, Onizuka M, et al.Decreased risk of acute graft-versus-host disease following allogeneic hematopoietic stem cell transplantation in patients with the 5,10-methylenetetrahydrofolate reductase 677TT genotype.Int J Hematol. 2008;87(5):451-458. [42]Rocha V, Porcher R, Fernandes JF, et al.Association of drug metabolism gene polymorphisms with toxicities, graft-versus-host disease and survival after HLA-identical sibling hematopoietic stem cell transplantation for patients with leukemia.Leukemia. 2009;23(3):545-556. |
| [1] | Wang Jing, Xiong Shan, Cao Jin, Feng Linwei, Wang Xin. Role and mechanism of interleukin-3 in bone metabolism [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1260-1265. |
| [2] | Xiao Hao, Liu Jing, Zhou Jun. Research progress of pulsed electromagnetic field in the treatment of postmenopausal osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1266-1271. |
| [3] | Hui Xiaoshan, Bai Jing, Zhou Siyuan, Wang Jie, Zhang Jinsheng, He Qingyong, Meng Peipei. Theoretical mechanism of traditional Chinese medicine theory on stem cell induced differentiation [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1125-1129. |
| [4] | An Weizheng, He Xiao, Ren Shuai, Liu Jianyu. Potential of muscle-derived stem cells in peripheral nerve regeneration [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1130-1136. |
| [5] | Fan Yiming, Liu Fangyu, Zhang Hongyu, Li Shuai, Wang Yansong. Serial questions about endogenous neural stem cell response in the ependymal zone after spinal cord injury [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1137-1142. |
| [6] | Tian Chuan, Zhu Xiangqing, Yang Zailing, Yan Donghai, Li Ye, Wang Yanying, Yang Yukun, He Jie, Lü Guanke, Cai Xuemin, Shu Liping, He Zhixu, Pan Xinghua. Bone marrow mesenchymal stem cells regulate ovarian aging in macaques [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 985-991. |
| [7] | Hou Jingying, Guo Tianzhu, Yu Menglei, Long Huibao, Wu Hao. Hypoxia preconditioning targets and downregulates miR-195 and promotes bone marrow mesenchymal stem cell survival and pro-angiogenic potential by activating MALAT1 [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1005-1011. |
| [8] | Zhou Ying, Zhang Huan, Liao Song, Hu Fanqi, Yi Jing, Liu Yubin, Jin Jide. Immunomodulatory effects of deferoxamine and interferon gamma on human dental pulp stem cells [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1012-1019. |
| [9] | Liang Xuezhen, Yang Xi, Li Jiacheng, Luo Di, Xu Bo, Li Gang. Bushen Huoxue capsule regulates osteogenic and adipogenic differentiation of rat bone marrow mesenchymal stem cells via Hedgehog signaling pathway [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1020-1026. |
| [10] | Wang Jifang, Bao Zhen, Qiao Yahong. miR-206 regulates EVI1 gene expression and cell biological behavior in stem cells of small cell lung cancer [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1027-1031. |
| [11] | Liu Feng, Peng Yuhuan, Luo Liangping, Wu Benqing. Plant-derived basic fibroblast growth factor maintains the growth and differentiation of human embryonic stem cells [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1032-1037. |
| [12] | Wen Dandan, Li Qiang, Shen Caiqi, Ji Zhe, Jin Peisheng. Nocardia rubra cell wall skeleton for extemal use improves the viability of adipogenic mesenchymal stem cells and promotes diabetes wound repair [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1038-1044. |
| [13] | Zhu Bingbing, Deng Jianghua, Chen Jingjing, Mu Xiaoling. Interleukin-8 receptor enhances the migration and adhesion of umbilical cord mesenchymal stem cells to injured endothelium [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1045-1050. |
| [14] | Luo Xiaoling, Zhang Li, Yang Maohua, Xu Jie, Xu Xiaomei. Effect of naringenin on osteogenic differentiation of human periodontal ligament stem cells [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1051-1056. |
| [15] | Wang Xinmin, Liu Fei, Xu Jie, Bai Yuxi, Lü Jian. Core decompression combined with dental pulp stem cells in the treatment of steroid-associated femoral head necrosis in rabbits [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1074-1079. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||