Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (4): 621-627.doi: 10.3969/j.issn.2095-4344.1044
Previous Articles Next Articles
Lumbar spondylolisthesis: status and prospects of implant treatment
Li Xianzhou, Wang Qian, Zhang Cunxin
- Department of Spine Surgery, Eastern Branch of Jining No. 1 People’s Hospital, Jining 272111, Shandong Province, China
-
Online:2019-02-08Published:2019-02-08 -
Contact:Zhang Cunxin, Department of Spine Surgery, Eastern Branch of Jining No. 1 People’s Hospital, Jining 272111, Shandong Province, China -
About author:Li Xianzhou, Chief physician, Department of Spine Surgery, Eastern Branch of Jining No. 1 People’s Hospital, Jining 272111, Shandong Province, China
CLC Number:
Cite this article
Li Xianzhou, Wang Qian, Zhang Cunxin . Lumbar spondylolisthesis: status and prospects of implant treatment[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(4): 621-627.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
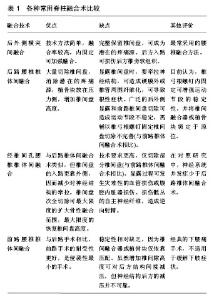
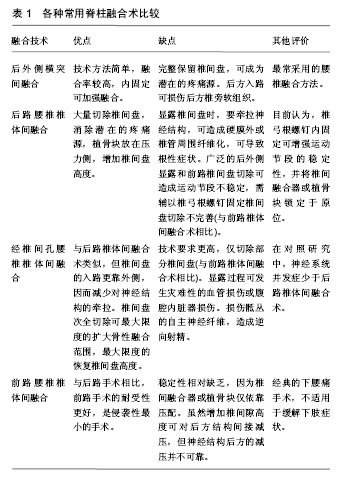
2.1 神经减压术 神经减压术顾名思义其目的在对受压迫的神经进行减压,以缓解神经受压引起的临床症状。对于减压范围众多学者各持己见,无外乎分为两派,一派坚持扩大减压,以充分松解受压神经;一派坚持达到有效减压即可,过度减压易导致脊柱不稳。但不可否认,多数轻度滑脱、神经受压患者,经单纯神经减压治疗后获得了满意的效果[5]。阮狄克等[6]对28例Ⅰ度腰椎滑脱椎管狭窄患者行单纯椎板开窗减压手术,术后随访发现其近中远期疗效均较理想。同时其研究发现,对于大于Ⅱ度的椎体滑脱患者,行单纯减压增加了脊柱不稳的概率,建议减压同时应辅助脊柱内固定对滑脱阶段加以融合。这一观点与国内西永明等[4]团队的研究结果一致。国外Johnsson等[7]随访了单纯椎板切除而没有进行椎体融合的腰椎滑脱患者,发现术后超过一半的患者出现了脊柱不稳、原发椎体滑脱及神经受压症状加重的情况。而采取微创手术有限减压,尽可能保留脊柱中柱稳定性的患者,其术后滑脱症状再次加重率降至30%以下。这与Sairyo等[8]研究结果基本一致,其原因主要归功于微创术式保留了脊柱中柱的稳定性[5]。综上所述,如单纯减压必须切除椎板时,需辅以脊柱融合;如椎体滑脱无椎管狭窄时,只需融合不稳的脊柱即可。 2.2 脊柱融合术 随着科学技术的进步和医学的发展,脊柱融合技术目前也是多种多样,但其最终目的一致,都是应用各式脊柱内固定器械来固定失稳脊柱。虽然脊柱融合固定后缓解了椎管狭窄、神经受压等临床症状,但其弊端随着术后患者随访时间的延长,也越来越多的暴露在人们面前。脊柱活动度丢失,相邻节段退变加速,腰背部肌肉僵直,慢性腰背疼痛等屡见报道。脊柱融合方式多种多样,常见的方式有前路椎体间融合、后路椎体间融合、经椎间孔椎体间融合、极外侧椎间融合、腰椎后外侧融合、环状融合(又称前后路联合融合或360°融合)、峡部关节处直接修复术、L5椎体切除术以及各种微创手术治疗等。各种手术的优缺点见表1。"

2.2.1 前路椎体间融合术 顾名思义该术式于椎体前方操作,借助椎间融合器融合滑脱椎体[9]。该手术方式主要用于无法行后路手术或轻度腰椎滑脱者。国内外关于前路椎体间融合术式疗效均有报道,Inoue等[10]、陈守来等[11]、王慧敏等[12]均随访报道了前路椎体间融合术后患者长期随访满意率较高。前路椎体间融合术式可通过恢复椎间高度及复位滑脱椎体间接实现椎管减压,而不必破坏椎间关节、椎板、脊突及椎旁肌等结构,保留了脊柱中柱及后柱的稳定性。但其弊端也越来越多的被报道,因其无法对椎管直接减压,如椎管存在骨性狭窄,其术后效果较差,因此楚戈等[13]建议在行前路椎体间融合术时应辅以后路减压。另外,逆向射精、内脏损伤、肾静脉血栓形成、血管损伤、术后肠麻痹等并发症也屡见报道。对于重度腰椎滑脱患者,不建议行前路椎体间融合术手术。 2.2.2 后路椎间融合术 该术式对于轻中重度腰椎滑脱均可适用,对于重度滑脱,可先行滑脱椎体提拉复位,再行椎间融合固定[14]。该术式借助坚强的内固定器械在实现对受压神经确切减压的同时,可维持脊柱三维矫形、恢复脊柱正常生理曲度及脊柱稳定,防止植骨块的塌陷及脱出,增加植骨愈合率及椎间融合率[15]。椎体间的融合常需借助人工椎间融合器如Cage、BAK等,也可取髂骨块或减压骨块行自体骨移植。因术中需置入椎弓根螺钉,在置钉过程中存在损伤两侧神经根的风险。为此,一些专家及学者建议减少椎弓根螺钉的使用数量,以降低发生神经根损伤的概率。因此单钉棒固定系常被用来治疗短节段的轻度滑脱。楚戈等[16]通过对比研究,发现单、双侧钉棒内固定系统治疗短节段腰椎滑脱,术后疗效差异无显著性意义,但单钉棒内固定系统手术更安全、医疗费用更低。 2.2.3 经椎间孔椎间融合术 该术式通过显露单侧或双侧椎间孔来对受压神经减压,再辅以脊柱内固定系统稳定脊柱。因其无需切除关节突关节,可有效避免损伤神经根及硬膜囊,所以经椎间孔椎间融合多用于高位椎体滑脱及二次手术避免硬膜瘢痕形成[13]。Lowe等[17]追踪分析了40例因退行性腰椎滑脱行单侧经椎间孔椎间融合双侧融合的患者,术后90%的患者可获得牢固的融合。术后3年随访发现,目测类比评分显著提高,85%的患者均可获得满意疗效。因该术式不切除或仅切除一侧关节突关节,所以对脊柱稳定性破坏不大。 2.2.4 极外侧椎间融合术 由Ozgur等[18]于2006年首次报道,该术式经腰大肌进入椎间盘[19],无需打开腹膜,其优点是避免了前路椎体间融合术式逆向射精、内脏损伤、肾静脉血栓形成、血管损伤、术后肠麻痹等并发症,但却无法实现对椎管内的减压,所以该术式适用于轻度滑脱患者。对于椎体滑脱合并椎管骨性狭窄者并不适合。Rodgers等[20]对600例实施极外侧椎间融合的患者进行随访研究发现,与传统开放手术比较,极外侧椎间融合在降低手术并发症方面确实更胜一筹,但其远期效果有待进一步观察。 2.2.5 椎体环周360°融合术 椎体环周融合植骨面广、植骨量大,增加了椎体间融合后的机械强度[21],可有效提升椎间植骨融合率。Helenius等[22]对腰椎重度滑脱的儿童或青少年患者分别行前路椎体间融合术、后路椎体间融合术和椎体环周融合,经过长期随访发现椎体环周植骨融合术其疗效要明显优于前两者。Kwon等[23]对于成人轻度腰椎滑脱伴峡部裂的患者实椎体环周融合术后,随访结果与Helenius等[22]基本一致,认为椎体环周融合可有效提高椎间植骨融合率,改善术后疗效。该术式通常联合椎体滑脱提拉复位同时进行,单纯融合并不能有效改善神经症状。 2.3 峡部关节处直接修复术 腰椎峡部指上、下关节突之间的狭窄部分,此处骨质结构相对薄弱,容易发生骨折。正常腰凸向前,骶凸向后,L5/S1处为生理弯曲的转折点。上方腰椎向前倾斜,下方骶椎向后倾斜,因此,腰椎的负重力自然形成向前的分力,使L5有向前滑移的倾向。生理状态下,L5下关节突和周围关节囊、韧带、肌肉等的力量可维持腰椎的稳定,从而使L5峡部成为应力点,因此峡部容最易发生骨折、崩裂,这也是L5峡部崩裂最多的原因。峡部崩裂直接修复术,适用于青壮年有神经症状但不伴有盘源性腰痛的患者[24]。Ivanic等[25]对113例腰椎滑脱并峡部裂的患者行峡部关节处直接植骨修复,术后长期随访发现小于14岁的患者其植骨融合率明显高于20岁以上的患者,认为该术式比较适用于年轻患者。 2.4 L5椎体切除术 L5椎体切除术并不常用,其适应证相对较窄,主要包括重度腰椎滑脱合并严重腰骶部畸形或脊椎失稳的患者,以及对于重度腰椎滑脱术后失败的补救手术。Gaines等[26]首先报道了应用该术式行L4与S1椎体直接融合的病例,认为该术式可以重建脊柱矢状位的平衡及减少神经损伤的风险。在后期的临床工作中,对30例重度腰椎滑脱行L5椎体切除术的患者长达15年的随访发现,L5椎体切除术后并未发生马尾神经症状,认为其中远期疗效可靠。Wild等[27]对婴幼儿重度腰椎滑脱合并腰骶部畸形患者行L5椎体切除术,术后随访10年,亦未见明显不良并发症。邹德威等[28]采用前路行L5椎体切除联合后路RF复位固定治疗V度腰椎滑脱,也取得了良好效果。因此,L5椎体切除术其手术疗效比较可靠,但其在临床工作中并不常用,可能与患者重度腰椎滑脱发病率相对较低有关。 2.5 微创手术治疗 微创手术与传统开放手术相比,可有效避免损伤椎旁软组织,减少术中、术后出血,减轻术后疼痛轻、缩短住院周期,更易于被临床医生及患者接受。目前常用的微创术式有经皮前路腰骶椎间轴向融合术、微创后路腰椎滑脱复位融合手术及腹腔镜前路腰椎滑脱复位融合术等,其共同特点是需要特殊的微创操作器械。Kim等[29]发现经微创手术可有效避免椎旁肌萎缩、肌力下降及腰背部软组织慢性疼痛等缺点,并且在减少术中、术后出血量及减少镇痛药物使用量及降低患者住院日方面具有明显优势。Wu等[30]对比微创经椎间孔椎间融合与传统开放手术发现,2种术式在植骨融合率方面相当,但微创术后的并发症发生率相对稍低,这一发现与Tsutsumimoto等[31]的研究结果基本一致。目前各种研究均报道微创手术后疗效较好,但其远期疗效有待进一步研究。"

| [1] 任杭岭,耿伟,马金柱,等.腰椎滑脱症患者手术前后脊柱-骨盆矢状位参数变化与临床疗效的相关性分析[J].中国修复重建外科杂志, 2015,29(10):1269-1274.[2] Pankowski R, Smoczynski A, Roclawski M, et al. Operative treatment of isthmic spondylolisthesis with posterior stabilization and ALIF. Cages versus autogenous bone grafts. Stud Health Technol Inform. 2012;176:311-314. [3] 潘良春,黄彰,江华.腰椎滑脱症的治疗进展[J].创伤外科杂志, 2009, 11(3):278-280.[4] 西永明,贾连顺.退行性腰椎滑脱外科治疗中的相关问题[J].中国脊柱脊髓杂志,2006,16(1):65-67.[5] Sengupta DK, Herkowitz HN. Degenerative spondylolisthesis: review of current trends and controversies. Spine (Phila Pa 1976). 2005;30(6 Suppl):S71-S81. [6] 阮狄克,何勍,丁宇,等.单纯减压治疗伴Ⅰ度退变滑脱的腰椎管狭窄症的中远期疗效分析[J].中国脊柱脊髓杂志, 2006,16(1):11-14.[7] Johnsson R, Stromqvist B, Axelsson P, et al. Influence of spinal immobilization on consolidation of posterolateral lumbosacral fusion. A roentgen stereophotogrammetric and radiographic analysis. Spine (Phila Pa 1976). 1992;17(1):16-21. [8] Sairyo K, Katoh S, Sakamaki T, et al. Vertebral forward slippage in immature lumbar spine occurs following epiphyseal separation and its occurrence is unrelated to disc degeneration: is the pediatric spondylolisthesis a physis stress fracture of vertebral body? Spine (Phila Pa 1976). 2004;29(5):524-527. [9] Kanamori M, Yasuda T, Hori T, et al. Minimum 10-year follow-up study of anterior lumbar interbody fusion for degenerative spondylolisthesis: progressive pattern of the adjacent disc degeneration. Asian Spine J. 2012;6(2):105-114. [10] Inoue S, Watanabe T, Goto S, et al. Degenerative spondylolisthesis. Pathophysiology and results of anterior interbody fusion. Clin Orthop Relat Res. 1988;227:90-98. [11] 陈守来,陈浩,陈明江,等. 经前路椎体间植骨融合治疗腰椎滑脱[J].中国矫形外科杂志,2000,7(7):79-80.[12] 王慧敏,谭明生,李子荣,等. 椎体间融合器治疗腰椎滑脱症[J].中国矫形外科杂志,2003,11(Z1):47-49.[13] 楚戈,白靖平,锡林•宝勒日,等.退变性腰椎滑脱的治疗进展[J].中国矫形外科杂志,2007,15(19):1486-1488.[14] Klockner C, Weber U. Correction of lumbosacral kyphosis in high grade spondylolisthesis and spondyloptosis. Orthopade. 2001; 30(12):983-987. [15] 王建顺,王新虎,刘继军,等.椎弓根螺钉内固定结合椎体间植骨术治疗腰椎滑脱症的疗效观察[J].中国骨与关节损伤杂志, 2008,23(8): 669-670.[16] 楚戈,卡哈尔•艾肯木,何祖胜.单、双侧后外侧椎弓根钉置入并植骨融合治疗退变性腰椎滑脱的随机对照[J].中国组织工程研究与临床康复,2011,15(35):6540-6545.[17] Lowe TG, Tahernia AD, O'Brien MF, et al. Unilateral transforaminal posterior lumbar interbody fusion (TLIF): indications, technique, and 2-year results. J Spinal Disord Tech. 2002;15(1):31-38. [18] Ozgur BM, Aryan HE, Pimenta L, et al. Extreme Lateral Interbody Fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006;6(4):435-443. [19] Lehmer SM, Steffee AD, Gaines RJ. Treatment of L5-S1 spondyloptosis by staged L5 resection with reduction and fusion of L4 onto S1 (Gaines procedure). Spine (Phila Pa 1976). 1994; 19(17):1916-1925. [20] Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011;36(1):26-32. [21] La Rosa G, Conti A, Cacciola F, et al. Pedicle screw fixation for isthmic spondylolisthesis: does posterior lumbar interbody fusion improve outcome over posterolateral fusion? J Neurosurg. 2003; 99(2 Suppl):143-150. [22] Helenius I, Lamberg T, Osterman K, et al. Posterolateral, anterior, or circumferential fusion in situ for high-grade spondylolisthesis in young patients: a long-term evaluation using the Scoliosis Research Society questionnaire. Spine (Phila Pa 1976). 2006; 31(2):190-196. [23] Kwon BK, Hilibrand AS, Malloy K, et al. A critical analysis of the literature regarding surgical approach and outcome for adult low-grade isthmic spondylolisthesis. J Spinal Disord Tech. 2005; 18 Suppl: S30-S40. [24] Lundin DA, Wiseman D, Ellenbogen RG, et al. Direct repair of the pars interarticularis for spondylolysis and spondylolisthesis. Pediatr Neurosurg. 2003;39(4):195-200. [25] Ivanic GM, Pink TP, Achatz W, et al. Direct stabilization of lumbar spondylolysis with a hook screw: mean 11-year follow-up period for 113 patients. Spine (Phila Pa 1976). 2003;28(3):255-259. [26] Gaines RW. L5 vertebrectomy for the surgical treatment of spondyloptosis: thirty cases in 25 years. Spine (Phila Pa 1976). 2005;30(6 Suppl):S66-S70. [27] Wild A, Jager M, Werner A, et al. Treatment of congenital spondyloptosis in an 18-month-old patient with a 10-year follow-up. Spine (Phila Pa 1976). 2001;26(21):E502-E505. [28] 邹德威,海涌,马华松,等.重度腰椎滑脱的治疗[J].中华骨科杂志, 1998,18(5):4-7.[29] Kim DY, Lee SH, Chung SK, et al. Comparison of multifidus muscle atrophy and trunk extension muscle strength: percutaneous versus open pedicle screw fixation. Spine (Phila Pa 1976). 2005;30(1):123-129. [30] Wu RH, Fraser JF, Hartl R. Minimal access versus open transforaminal lumbar interbody fusion: meta-analysis of fusion rates. Spine (Phila Pa 1976). 2010;35(26):2273-2281. [31] Tsutsumimoto T, Shimogata M, Ohta H, et al. Mini-open versus conventional open posterior lumbar interbody fusion for the treatment of lumbar degenerative spondylolisthesis: comparison of paraspinal muscle damage and slip reduction. Spine (Phila Pa 1976). 2009;34(18):1923-1928. [32] Mihara H, Onari K, Cheng BC, et al. The biomechanical effects of spondylolysis and its treatment. Spine (Phila Pa 1976). 2003; 28(3):235-238. [33] 郑应,谭明生.腰椎后路非融合固定系统的临床应用[J].中国骨伤, 2007,20(4):283-285.[34] Agabegi SS, Fischgrund JS. Contemporary management of isthmic spondylolisthesis: pediatric and adult. Spine J. 2010; 10(6):530-543. [35] Jacobs WC, Vreeling A, De Kleuver M. Fusion for low-grade adult isthmic spondylolisthesis: a systematic review of the literature. Eur Spine J. 2006;15(4):391-402. [36] Ohtori S, Koshi T, Yamashita M, et al. Single-level instrumented posterolateral fusion versus non-instrumented anterior interbody fusion for lumbar spondylolisthesis: a prospective study with a 2-year follow-up. J Orthop Sci. 2011;16(4):352-358. [37] Musluman AM, Yilmaz A, Cansever T, et al. Posterior lumbar interbody fusion versus posterolateral fusion with instrumentation in the treatment of low-grade isthmic spondylolisthesis: midterm clinical outcomes. J Neurosurg Spine. 2011;14(4):488-496. [38] Zhou ZJ, Zhao FD, Fang XQ, et al. Meta-analysis of instrumented posterior interbody fusion versus instrumented posterolateral fusion in the lumbar spine. J Neurosurg Spine. 2011;15(3): 295-310. [39] Humphreys SC, Hodges SD, Patwardhan AG, et al. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine (Phila Pa 1976). 2001;26(5):567-571. [40] Kim KT, Lee SH, Lee YH, et al. Clinical outcomes of 3 fusion methods through the posterior approach in the lumbar spine. Spine (Phila Pa 1976). 2006;31(12):1351-1357, 1358. [41] Min JH, Jang JS, Lee SH. Comparison of anterior- and posterior-approach instrumented lumbar interbody fusion for spondylolisthesis. J Neurosurg Spine. 2007;7(1):21-26. [42] Hsieh PC, Koski TR, O'Shaughnessy BA, et al. Anterior lumbar interbody fusion in comparison with transforaminal lumbar interbody fusion: implications for the restoration of foraminal height, local disc angle, lumbar lordosis, and sagittal balance. J Neurosurg Spine. 2007;7(4):379-386. [43] Kim JS, Kang BU, Lee SH, et al. Mini-transforaminal lumbar interbody fusion versus anterior lumbar interbody fusion augmented by percutaneous pedicle screw fixation: a comparison of surgical outcomes in adult low-grade isthmic spondylolisthesis. J Spinal Disord Tech. 2009;22(2):114-121. [44] Kim JS, Lee KY, Lee SH, et al. Which lumbar interbody fusion technique is better in terms of level for the treatment of unstable isthmic spondylolisthesis? J Neurosurg Spine. 2010;12(2): 171-177. [45] Yan DL, Pei FX, Li J, et al. Comparative study of PILF and TLIF treatment in adult degenerative spondylolisthesis. Eur Spine J. 2008;17(10):1311-1316. [46] Goz V, Weinreb JH, Schwab F, et al. Comparison of complications, costs, and length of stay of three different lumbar interbody fusion techniques: an analysis of the Nationwide Inpatient Sample database. Spine J. 2014;14(9):2019-2027. [47] Kwon BK, Albert TJ. Adult low-grade acquired spondylolytic spondylolisthesis: evaluation and management. Spine (Phila Pa 1976). 2005;30(6 Suppl):S35-S41. [48] Hakalo J, Wronski J. The role of reduction in operative treatment of spondylolytic spondylolisthesis. Neurol Neurochir Pol. 2008; 42(4):345-352. [49] Soegaard R, Bunger CE, Christiansen T, et al. Circumferential fusion is dominant over posterolateral fusion in a long-term perspective: cost-utility evaluation of a randomized controlled trial in severe, chronic low back pain. Spine (Phila Pa 1976). 2007; 32(22):2405-2414. [50] Videbaek TS, Christensen FB, Soegaard R, et al. Circumferential fusion improves outcome in comparison with instrumented posterolateral fusion: long-term results of a randomized clinical trial. Spine (Phila Pa 1976). 2006;31(25):2875-2880. [51] Remes V, Lamberg T, Tervahartiala P, et al. Long-term outcome after posterolateral, anterior, and circumferential fusion for high-grade isthmic spondylolisthesis in children and adolescents: magnetic resonance imaging findings after average of 17-year follow-up. Spine (Phila Pa 1976). 2006;31(21):2491-2499. [52] Swan J, Hurwitz E, Malek F, et al. Surgical treatment for unstable low-grade isthmic spondylolisthesis in adults: a prospective controlled study of posterior instrumented fusion compared with combined anterior-posterior fusion. Spine J. 2006;6(6):606-614. [53] Kim JS, Kim DH, Lee SH, et al. Comparison study of the instrumented circumferential fusion with instrumented anterior lumbar interbody fusion as a surgical procedure for adult low-grade isthmic spondylolisthesis. World Neurosurg. 2010; 73(5):565-571. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Wang Haiying, Lü Bing, Li Hui, Wang Shunyi. Posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis: prediction of functional prognosis of patients based on spinopelvic parameters [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1393-1397. |
| [3] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [4] | Song Chengjie, Chang Hengrui, Shi Mingxin, Meng Xianzhong. Research progress in biomechanical stability of lateral lumbar interbody fusion [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 923-928. |
| [5] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [6] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [7] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [8] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [9] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [10] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [11] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [12] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [13] | Qian Xuankun, Huang Hefei, Wu Chengcong, Liu Keting, Ou Hua, Zhang Jinpeng, Ren Jing, Wan Jianshan. Computer-assisted navigation combined with minimally invasive transforaminal lumbar interbody fusion for lumbar spondylolisthesis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3790-3795. |
| [14] | Tang Xiaokai, Li Weiming. Role and mechanism of Nel-like molecule-1 in promoting bone fusion after spinal fusion [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3914-3920. |
| [15] | Yang Qin, Zhou Honghai, Chen Longhao, Zhong Zhong, Xu Yigao, Huang Zhaozhi. Research status and development trend of pelvic reconstruction techniques: a bibliometric and visual analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(23): 3718-3724. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||