Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (7): 1140-1148.doi: 10.3969/j.issn.2095-4344.0130
Unilateral versus bilateral percutaneous kyphoplasty for osteoporotic vertebral fractures: a meta-analysis
Gao Zhi-xiang, Li Chun, Li Lei, Huang Wei-min
- Department of Spinal Surgery, the Sixth Affiliated Hospital of Xinjiang Medical University, Urumqi 830002, Xinjiang Uygur Autonomous Region, China
-
Online:2018-03-08Published:2018-03-08 -
Contact:Huang Wei-min, Associate professor, Chief physician, Master’s supervisor, Department of Spinal Surgery, the Sixth Affiliated Hospital of Xinjiang Medical University, Urumqi 830002, Xinjiang Uygur Autonomous Region, China -
About author:Gao Zhi-xiang, Studying for master’s degree, Department of Spinal Surgery, the Sixth Affiliated Hospital of Xinjiang Medical University, Urumqi 830002, Xinjiang Uygur Autonomous Region, China
CLC Number:
Cite this article
Gao Zhi-xiang, Li Chun, Li Lei, Huang Wei-min. Unilateral versus bilateral percutaneous kyphoplasty for osteoporotic vertebral fractures: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2018, 22(7): 1140-1148.
share this article
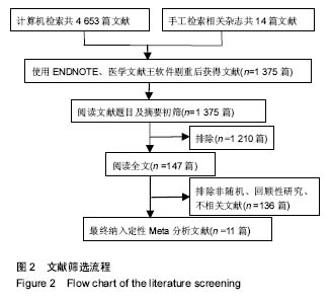
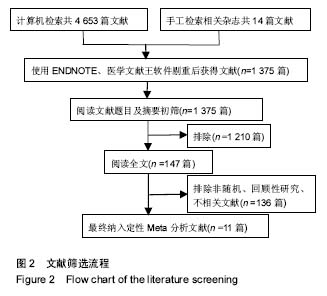
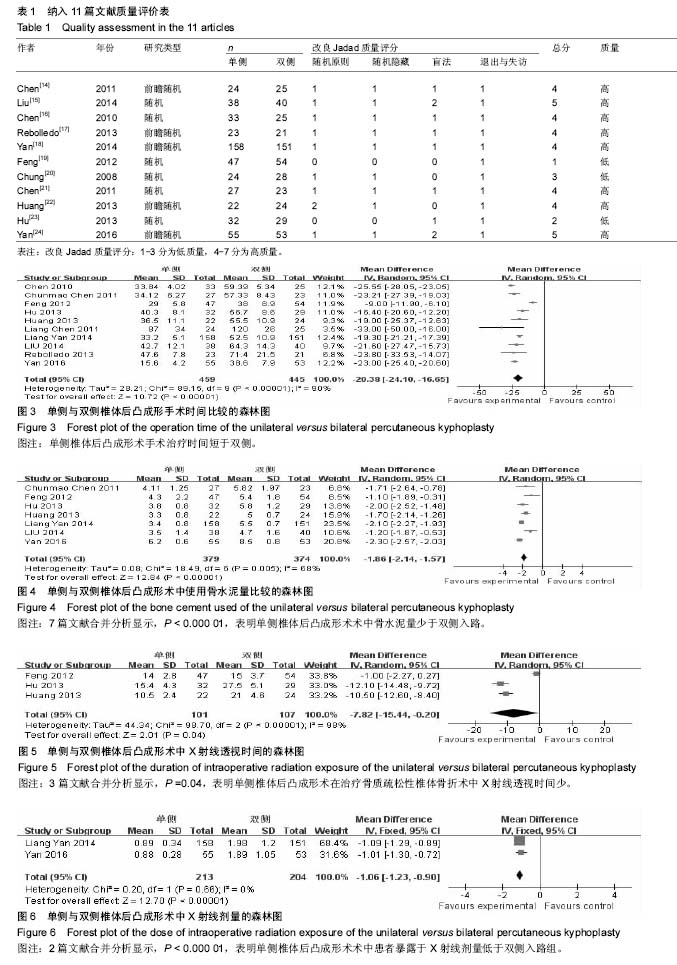
2.1 文献筛选结果及质量 初步检索共得到4 635篇文献,通过阅读文献标题及摘要排除重复文献,按照上述纳入及排除标准阅读全文最终得到11篇文献进行Meta分 析[14-24],其中6篇随机对照试验,5篇前瞻性随机对照试验,共956例患者,其中单侧组483例,双侧组473例;文献筛选流程见图2。 2位作者根据改良的Jadad评分量表分别对纳入的11篇文献进行质量评价。从文献的随机原则、随机隐藏、盲法、退出与失访4个方面进行评价,纳入的11篇文献中低质量文献3篇,高质量文献8篇,见表1。"

2.2 Meta分析结果 2.2.1 手术时间 纳入的11篇文献中有10篇文献详细比较了手术时间[14-19,21-24]。各研究结果之间存在异质性 (P < 0.000 01,I²= 90%),采用随机效应模式。Meta分析结果显示单侧与双侧经皮椎体后凸成形术相比,2组差异有显著性意义[MD=-20.38,95%CI(-24.10,-16.65),P < 0.000 01,图3],单侧经皮椎体后凸成形术治疗骨质疏松性椎体骨折的手术时间比双侧短。 2.2.2 术中骨水泥使用量 7篇文献报道研究术中骨水泥的使用量[15,18-19,21-24],各组间存在异质性(P=0.005,I²=68%),采用随机效应模式进行Meta分析示,单侧与双侧手术方式在骨水泥的使用量方面差异有显著性意义[MD=-1.86,95%CI(-2.14,-1.57),P < 0.000 01,图4],单侧入路手术方式骨水泥使用量明显少于双侧。 2.2.3 术中放射时间及剂量 3篇文献报道了术中X射线的暴露时间[19,22-23],合并分析显示各组间存在异质性 (P < 0.000 01,I²= 98%),采用随机效应模式进行Meta分析示,单侧与双侧手术方式术中X射线透视时间差异有显著性意义[MD=-7.82,95%CI(-15.44,-0.20),P=0.04,见图5]。2篇文献测量了术中X线辐射剂量[18,24],合并分析显示各组间无异质性(P=0.66,I²= 0%),采用固定效应模式进行Meta分析示,单侧与双侧手术方式术患者暴露于X射线剂量差异有显著性意义[MD=-1.06,95%CI(-1.23, -0.90),P < 0.000 01,见图6]。综上Meta分析线单侧入路手术方式在术中患者暴露于X射线的时间、剂量方面均低于双侧入路组。"

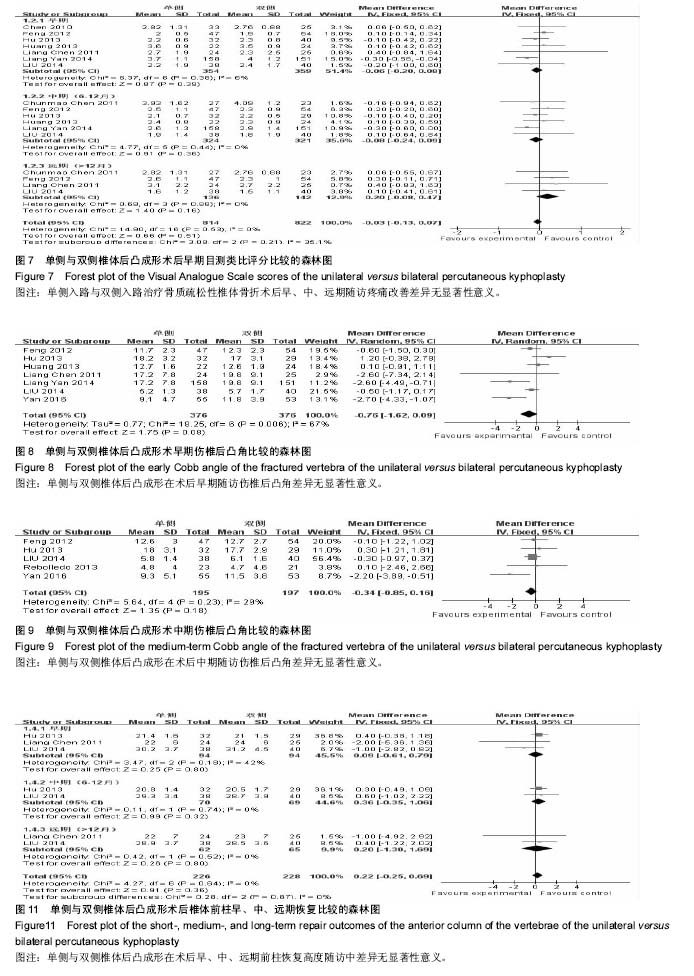
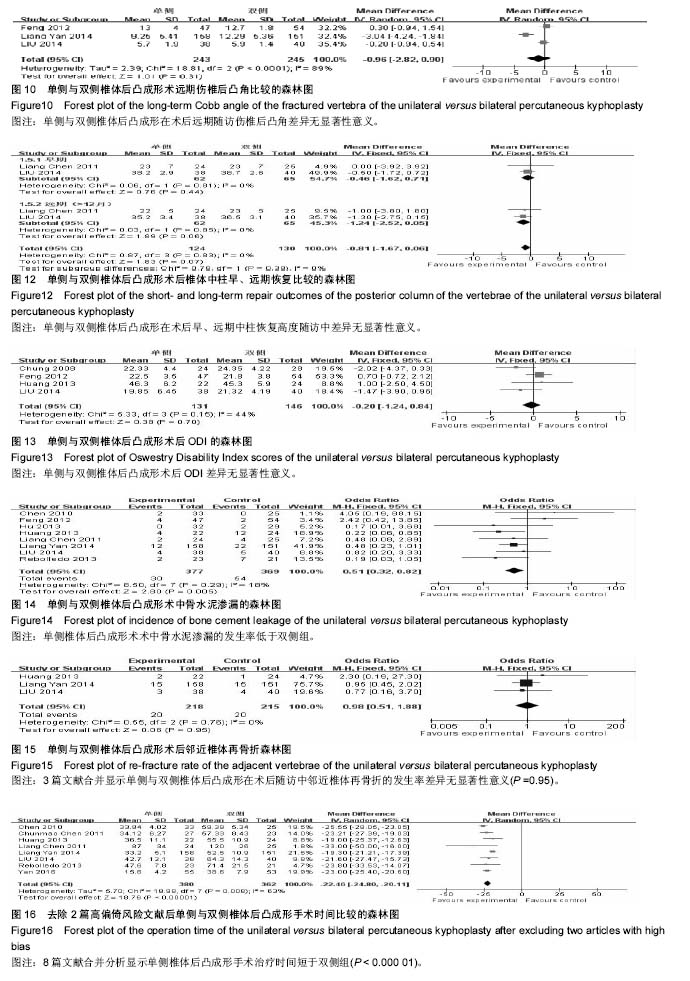
2.2.4 术后目测类比评分 本篇文献通过Meta分析评价评价两种手术方式术后目测类比评分在早期、中期、远期的评分比较。共7篇文献研究后术后早期目测类比评 分[14-16,18-19,22-23],各研究组间无异质性(P=0.38,I²= 6%),采用固定效应模式进行Meta分析示,单侧与双侧手术方式术后早期目测类比评分差异无显著性意义[MD=-0.06,95%CI(-0.20,0.08),P=0.39]。6篇文献报道了目测类比评分中期比较[15,18-19,21-23 ],各研究组间无异质性(P=0.44,I²= 0%),采用固定效应模式进行Meta分析示,单侧与双侧手术方式术后中期随访目测类比评分差异无显著性意义[MD=-0.88,95%CI (-0.24,0.09),P=0.36]。4篇文献报道了目测类比评分远期比较[14-15,19,21],各研究组间无异质性(P=0.88,I²= 0%),采用固定效应模式进行Meta分析示,两种手术方式术后远期随访目测类比评分差异无显著性意义[MD= 0.20,95%CI (-0.08,0.47),P=0.16> 0.05]。综上单侧入路组与双侧入路组在术后早期、中期、远期疼痛缓解程度方面差异无显著性意义,见图7。 2.2.5 术后伤椎后凸角 在最终纳入文献中有7篇文献研究了术后早期伤椎后凸角改善情况[14-15,18-19,22-24],各研究组间存在异质性(P=0.006,I²=67%),采用随机效应模式进行Meta分析示,单侧与双侧手术方式术后早期伤椎后凸角改变情况差异无显著性意义[MD=-0.76,95%CI (-1.62,0.09),P=0.08,图8]。5篇文献研究了术后中期伤椎后凸角变化[15,17,19,23-24 ],各研究组间无异质性(I²=29%),采用固定效应模式进行Meta分析示,单侧与双侧手术方式术后中期伤椎后凸角改变情况差异无显著性意义[MD=-0.34,95%CI(-0.85,0.16),P=0.18,图9]。3篇文献研究了术后远期伤椎后凸角变化[15,18-19],各研究组间存在异质性 (I²=89%),用随机效应模式进行Meta分析示,单侧与双侧手术方式术后远期伤椎后凸角改变情况差异无显著性意义[MD=-0.96,95%CI(-2.82,0.90),P=0.31,图10]。 2.2.6 椎体恢复高度 椎体恢复高度包括前柱和中柱。3篇文献报道了术后早期前柱恢复高度[14-15,23],各研究结果之间无异质性(P=0.18,I²= 42%),采用固定效应模式进行Meta分析示,两种手术方式术后早期椎体前柱恢复高度差异无显著性意义[MD=0.09,95%CI(-0.61,0.79),P=0.80]。2篇文献分别报道了术后中期随访椎体前柱高度[15,23],各研究结果间无异质性(P=0.74,I²=0%),采用固定效应模式进行Meta分析示,两种手术方式术后中期椎体前柱恢复高度差异无显著性意义[MD=0.36,95%CI(-0.35,1.06),P= 0.32]。2篇文献分别报道了术后远期随访椎体前柱高度[14-15],各研究结果间无异质性(P=0.64,I²=0%),采用固定效应模式进行Meta分析示,两种手术方式术后远期椎体前柱恢复高度差异无显著性意义[MD=0.20,95%CI(-1.30,1.69),P=0.80],见图11。2篇文献共同报道了术后早期、远期随访椎体中柱高度[14-15],各研究结果之间无异质性分别是(P=0.81,I²=0%),(P=0.85,I²= 0%),采用固定效应模式进行Meta分析示,两种手术方式术后早期、远期椎体中柱恢复高度差异无显著性意义分别是[MD=-0.46,95%CI(-1.62,0.71),P=0.44]、[MD=-1.24,95%CI(-2.52,0.05),P=0.06],见图12。 2.2.7 术后ODI 在最终纳入文献中有4篇问卷调查了患者术后ODI[15,19-20,22],各研究组间无异质性(P=0.15,I²=44%)。采用固定效应模式进行Meta分析示,2组手术方式见差异无显著性意义[MD=-0.20,95%CI(-1.24,0.84),P=0.70],见图13。 2.2.8 手术并发症 椎体后凸成形术的并发症主要包括术中骨水泥渗漏及术后邻近非手术椎体再骨折。8篇文献报道了骨水泥渗漏的研究情况[14-19,22-23],各组间无异质性 (P=0.29,I=18%),采用固定效应模式进行Meta分析示,单侧与双侧手术方式术中骨水泥渗漏分析差异有显著性意义[MD=0.51,95%CI(0.32,0.82),P=0.00],见图14。3篇文献报道了术后邻近椎体再骨折[15,18,2],各组间无异质性(I²= 0%),采用固定效应模式进行Meta分析示,单侧与双侧手术方式在术后随访中邻近椎体再骨折发生情况差异无显著性意义[MD= 0.98,95%CI(0.51,1.88),P=0.95],见图15。 2.2.9 敏感性分析 纳入的11篇文献中有3篇属于低质量文献[19-20,23],而在这3篇文献中有2篇详细比较了手术时间,故在手术时间方面去除该2篇低质量文献进行敏感性分 析[19,23],8篇文献的各研究组间仍存在异质性[14-18,21-22,24] (P=0.000 8,I²=63%),采用随机效应模式。Meta分析结果显示,单侧与双侧经皮椎体后凸成形术相比,2组差异有显著性意义[MD=-22.46,95%CI(-24.80,-20.11),P < 0.000 01,图16],单侧组经皮椎体后凸成形术治疗骨质疏松性椎体骨折的手术时间比双侧组短,与详细报道了手术时间的10篇文献研究结果相同[14-19,21-24];同时在手术时间方面将10篇文献的随机效应模式改成固定效应模式分析结果一致[14-19,21-24];同样使用上述两种方法分别对各项观察指标进行分析均得到与之相对应的结果。说明本次Meta分析的结果比较稳定。 "

"
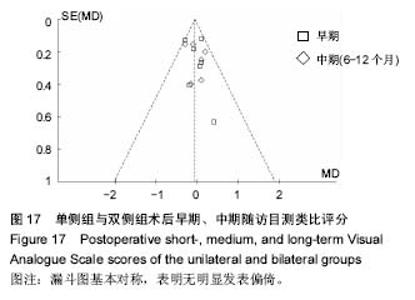
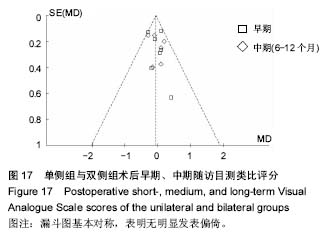
2.2.10 发表偏倚 对两种手术方式术后早、中期目测类比评分绘制漏斗图(图17),漏斗图对称,各纳入研究对象基本呈对称均匀分布,表明研究无明显发表偏倚。"
| [1] Amin S, Achenbach SJ, Atkinson EJ, et al. Trends in fracture incidence: a population-based study over 20 years. J Bone Miner Res. 2014; 29(3):581-589.[2] Alexandru D, So W. Evaluation and management of vertebral compression fractures. Perm J.2012;16(4):46-51.[3] McCarthy J, Davis A. Diagnosis and management of vertebral compression fractures. Am Fam Physician.2016;94(1): 44-50.[4] Galibert P, Deramond H, Rosat P, et al. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie.1987;33(2):166-168.[5] Lin JH, Chien LN, Tsai WL, et al. Early vertebroplasty associated with a lower risk of mortality and respiratory failure in aged patients with painful vertebral compression fractures: a population-based cohort study in Taiwan. Spine J. 2017;17(9):1310-1318.[6] Leali PT, Solla F, Maestretti G, et al. Safety and efficacy of vertebroplasty in the treatment of osteoporotic vertebral compression fractures: a prospective multicenter international randomized controlled study. Clin Cases Miner Bone Metab.2016; 13(3):234-236.[7] Goldstein CL, Chutkan NB, Choma TJ, et al. Management of the elderly with vertebral compression fractures. Neurosurgery.2015;77 Suppl 4:S33-45.[8] Zhang SM, Zhang ZJ, Liu YZ, et al. Treatment of senile osteoporotic vertebral compression fractures with percutaneous kyphoplasty. Zhongguo Gu Shang. 2011;24(7):570-573.[9] Steinmann J, Tingey CT, Cruz G, et al. Biomechanical comparison of unipedicular versus bipedicular kyphoplasty. Spine (Phila Pa 1976). 2005;30(2):201-205.[10] Schupfner R, Stoevelaar HJ, Blattert T, et al. Treatment of osteoporotic vertebral compression fractures: applicability of appropriateness criteria in clinical practice. Pain Phys.2016;19(1):E113-120[11] Ates A, Gemalmaz HC, Deveci MA, et al. Comparison of effectiveness of kyphoplasty and vertebroplasty in patients with osteoporotic vertebra fractures. Acta Orthop Traumatol Turc. 2016;50(6):619-622.[12] Chen H, Tang P, Zhao Y, et al. Unilateral versus bilateral balloon kyphoplasty in the treatment of osteoporotic vertebral compression fractures. Orthopedics.2014;37(9):e828-835.[13] Li LH, Sun TS, Liu Z, et al. Comparison of unipedicular and bipedicular percutaneous kyphoplasty for treating osteoporotic vertebral compression fractures: a meta-analysis. Chin Med J (Engl).2013; 126(20):3956-3961.[14] Chen L, Yang H, Tang T. Unilateral versus bilateral balloon kyphoplasty for multilevel osteoporotic vertebral compression fractures: a prospective study. Spine (Phila Pa 1976).2011;36(7):534-540.[15] Liu XJ, Wang XH, Zuo CG. The randomized controlled study of unilateral versus bilateral percutaneous kyphoplasty for the treatment of elderly osteoporotic vertebral compression fractures. J Cervicodynia Lumbodynia. 2014.[16] Chen C, Chen L, Gu Y, et al. Kyphoplasty for chronic painful osteoporotic vertebral compression fractures via unipedicular versus bipedicular approachment: A comparative study in early stage. Injury. 2010;41(4):356-359.[17] Rebolledo BJ, Gladnick BP, Unnanuntana A, et al. Comparison of unipedicular and bipedicular balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures: a prospective randomised study. Bone Joint J. 2013;95-B(3):401-406.[18] Yan L, He B, Hao D. A Comparison between unilateral transverse process-pedicle and bilateral puncture techniques in percutaneous kyphoplasty. Spine (Phila Pa 1976).2014;39(39):19-26.[19] Feng J, Zheng QX, Xiao SX, et al. Clinical comparison of unilateral and bilateral percutaneous kyphoplasty for treating osteoporotic vertebral compression fractures. Chin J Trad Med Traumatol Orthop. 2012; 20(10): 26-29.[20] Chung HJ, Chung KJ, Yoon HS, et al. Comparative study of balloon kyphoplasty with unilateral versus bilateral approach in osteoporotic vertebral compression fractures. Int Orthop. 2008;32(6):817-820.[21] Chen C, Wei H, Zhang W, et al. Comparative study of kyphoplasty for chronic painful osteoporotic vertebral compression fractures via unipedicular versus bipedicular approach. J Spinal Disord Tech. 2011;24(7):E62-65.[22] Huang S, Jing XU, Xiang YC. Comparative study of unipedicular versus bipedicular percutaneous vertebroplasty for the treatment of osteoporotic vertebral compression fractures. Orthop J China. 2013;21(2):115-118.[23] Hu AW, Xia CY, Zhou M, et al. Efficacy comparison of the effect on unipedicular versus bipedicular percutaneous kyphoplasty for osteoporotic vertebral compression fractures. J Clin Orthop. 2013.[24] Yan L, He B, Guo H, et al. The prospective self-controlled study of unilateral transverse processpedicle and bilateral puncture techniques in percutaneous kyphoplasty. Osteoporos Int. 2016;27(5):1849-1855.[25] Ensrud KE, Schousboe JT. Clinical practice. Vertebral fractures. N Engl J Med.2011;364(17):1634-1642.[26] Colangelo D, Nasto LA, Genitiempo M, et al. Kyphoplasty vs conservative treatment: a case-control study in 110 post-menopausal women population. Is kyphoplasty better than conservative treatment. Eur Rev Med Pharmacol Sci.2015;19(21):3998-4003.[27] Kanatli U, Ataoglu B, Ozer M, et al. Kyphoplasty for intractable pain due to glucocorticosteroid-induced osteoporotic vertebra fracture of a 9-year-old patient with systemic lupus erythematosus: 8-year follow-up. J Pediatr Orthop.2015;35(6):e55-59.[28] Oberkircher L, Struewer J, Bliemel C, et al. Height restoration and preservation in osteoporotic vertebral compression fractures: a biomechanical analysis of standard balloon kyphoplasty versus radiofrequency kyphoplasty in a cadaveric model. J Spinal Disord Tech.2014;27(5):283-289.[29] Qu HB, Tong PJ, Ji WF, et al. Percutaneous kyphoplasty for the treatment of osteoporotic vertebral compression fracture with degenerative scoliosis. Zhongguo Gu Shang. 2016;29(1):38-40.[30] Yuan WH, Hsu HC, Lai KL. Vertebroplasty and balloon kyphoplasty versus conservative treatment for osteoporotic vertebral compression fractures: A meta-analysis. Medicine (Baltimore).2016;95(31):e4491.[31] 申勇,刘法敬,张英泽,等. 单、双侧经皮椎体后凸成形术治疗骨质疏松性椎体压缩骨折的疗效[J]. 中国脊柱脊髓杂志,2011,21(3):202-206.[32] Papadopoulos EC, Edobor-Osula F, Gardner MJ, et al. Unipedicular balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures: early results. J Spinal Disord Tech. 2008;21(8): 589-596.[33] Sun G, Jin P, Li FD, et al. Preliminary study on a single balloon cross-midline expansion via unipedicular approach in kyphoplasty. Chin Med J (Engl).2008;121(18):1811-1814.[34] Gulseren A. Pain and Quality of Life in Osteoporosis. Int J Rehabil Res. 2009;32 Supplement 1:S26-S27.[35] 张平会. 探讨骨质疏松疼痛原因[J]. 世界最新医学信息文摘(连续型电子期刊),2015,15(81):169-170.[36] 曲源. 骨质疏松症疼痛原因临床分析[J]. 云南中医中药杂志,2011,32(5): 24-25.[37] 陈柏龄,黎艺强,谢登辉. TNF-α在骨质疏松性疼痛中的作用[J]. 中国病理生理杂志, 2010,26(10):1931-1935.[38] 吴文坚,梁裕,郑涛,等. 椎体压缩性骨折疼痛缓解程度与骨水泥充盈程度的关系[J]. 中国临床康复,2005,9(38):30-32.[39] He X, Li H, Meng Y, et al. Percutaneous kyphoplasty evaluated by cement volume and distribution: an analysis of clinical data. Pain Phys. 2016;19(7):495-506.[40] Fu Z, Hu X, Wu Y, et al. Is There a Dose-Response Relationship of Cement Volume With Cement Leakage and Pain Relief After Vertebroplasty. Dose Response. 2016;14(4):1559325816682867.[41] Yin F, Sun Z, Song S, et al. A comparative study on treatment of mid-thoracic osteoporotic vertebral compression fracture using percutaneous kyphoplasty with unilateral and bilateral approaches. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2016;30(1):77-81.[42] Park JS, Shin JH, Lim SH, et al. Lethal cement leakage embolization after kyphoplasty. Circ J. 2016;81(1):119-120.[43] Yang S, Liu Y, Yang H, et al. Risk factors and correlation of secondary adjacent vertebral compression fracture in percutaneous kyphoplasty. Int J Surg. 2016;36(Pt A):138-142.[44] 郑召民. 经皮椎体成形术和经皮椎体后凸成形术灾难性并发症——骨水泥渗漏及其预防[J]. 中华医学杂志,2006,86(43):3027-3030.[45] Maramattom BV. Extraosseous cement leakage after vertebroplasty producing intractable low back pain. Neurol India. 2017;65(2):375-376.[46] Zhu SY, Zhong ZM, Wu Q, et al. Risk factors for bone cement leakage in percutaneous vertebroplasty: a retrospective study of four hundred and eighty five patients. Int Orthop. 2016;40(6):1205-1210.[47] Xie W, Jin D, Ma H, et al. Cement leakage in percutaneous vertebral augmentation for osteoporotic vertebral compression fractures: analysis of risk factors. Clin Spine Surg. 2016;29(4):E171-176.[48] Cao J, Kong L, Meng F, et al. Risk factors for new vertebral compression fractures after vertebroplasty: a meta-analysis. ANZ J Surg. 2016;86(7-8):549-554.[49] Yamashita K, Higashino K, Wada K, et al. Radiation exposure to the surgeon and patient during a fluoroscopic procedure: how high is the exposure dose? A cadaveric study. Spine (Phila Pa 1976). 2016;41(15): 1254-1260. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [3] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [4] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [5] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [6] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [7] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [8] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [9] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [10] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [11] | Zhong Yuanming, Wan Tong, Zhong Xifeng, Wu Zhuotan, He Bingkun, Wu Sixian. Meta-analysis of the efficacy and safety of percutaneous curved vertebroplasty and unilateral pedicle approach percutaneous vertebroplasty in the treatment of osteoporotic vertebral compression fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 456-462. |
| [12] | Xu Weilong, Zuo Yuan, Xin Daqi, He Chenyang, Zhao Peng, Shi Ming, Zhou Boyuan, Liu Yating, Zhao Yan. Selection of modeling methods for acute compressive spinal cord injury: a network Meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(23): 3767-3772. |
| [13] | Feng Guancheng, Fang Jianming, Lü Haoran, Zhang Dongsheng, Wei Jiadong, Yu Bingbing. How does bone cement dispersion affect the early outcome of percutaneous vertebroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3450-3457. |
| [14] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [15] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||