Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (7): 1009-1003.doi: 10.3969/j.issn.2095-4344.0110
Previous Articles Next Articles
Application of hypobaric ropivacaine spinal anesthesia and nerve block anesthesia in hip surgery of elderly patients
Hao Chun-xiang, Han Chun-ji, Chen Guo-qing, Liu Shu-yun, Zhang Chang-sheng
- Anesthesia and Operation Center, Chinese PLA General Hospital, Beijing 100853, China
-
Online:2018-03-08Published:2018-03-08 -
Contact:Zhang Chang-sheng, M.D., Attending physician, Anesthesia and Operation Center, Chinese PLA General Hospital, Beijing 100853, China -
About author:Hao Chun-xiang, Attending physician, Anesthesia and Operation Center, Chinese PLA General Hospital, Beijing 100853, China -
Supported by:the Key Project of Tissue Engineering and R&D Theme Project for Biological Products and Pharmaceutical Technology (863 Program), No. 2012AA020502
CLC Number:
Cite this article
Hao Chun-xiang, Han Chun-ji, Chen Guo-qing, Liu Shu-yun, Zhang Chang-sheng. Application of hypobaric ropivacaine spinal anesthesia and nerve block anesthesia in hip surgery of elderly patients[J]. Chinese Journal of Tissue Engineering Research, 2018, 22(7): 1009-1003.
share this article
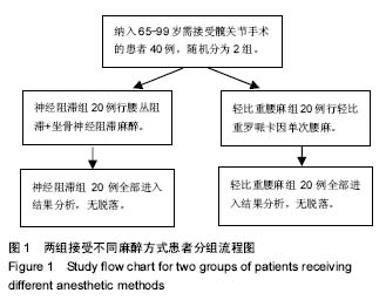
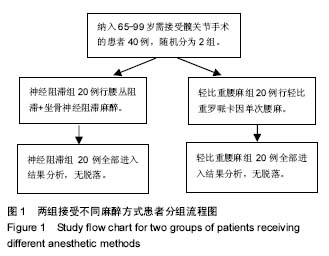
2.1 参与者数量分析 纳入观察对象40例,随机分为2组。全部病例均进入结果分析,无脱落。试验流程图见图1。"
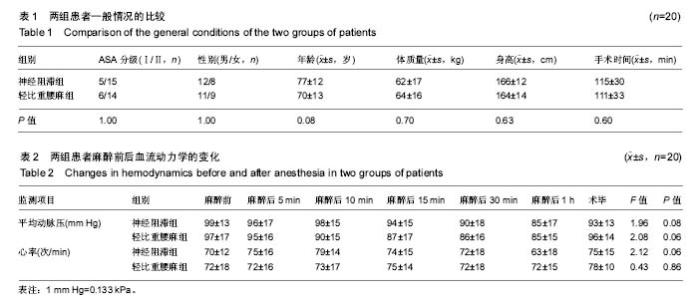
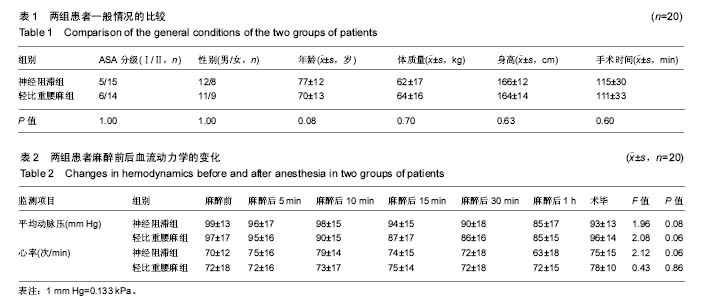
2.2 基线资料比较 两组患者的ASA分级、性别构成比经过Fisher确切概率法计算出P值均为1,年龄、体质量、身高、手术时间的比较中,差异均无显著性意义(P > 0.05),详见表1。 2.3 血流动力学指标 与麻醉前比较,神经阻滞组与轻比重腰麻组患者在麻醉后5,10,15,30 min、1 h和术毕时刻的平均动脉压及心率差异均无显著性意义,详见表2。"
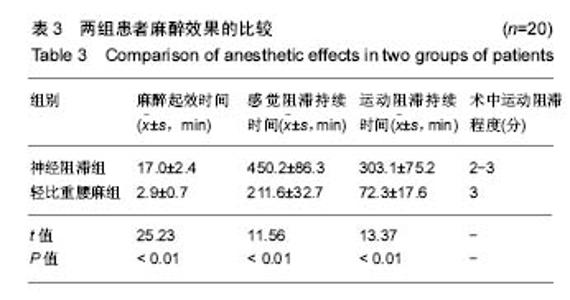
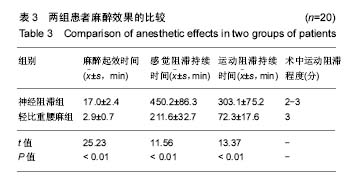
2.4 麻醉效果 腰麻组在麻醉实施后5 min,所有患者均达到手术切皮所需的麻醉平面及效果,即术区表面皮肤感觉消失,术侧肢体肌力消失,麻醉平面均上升至T8-10范围;神经阻滞组在麻醉实施后20 min,所有患者均达到手术切皮所需的麻醉效果。与神经阻滞组相比,轻比重腰麻组的麻醉起效时间更快(P < 0.01),但感觉与运动阻滞的时长较神经阻滞组短,差异有显著性意义(P < 0.01),详见表3。两组患者术后1 h的目测类比评分均为0分。 2.5 辅助用药 轻比重腰麻组患者在术中无需静脉麻醉药物辅助;而神经阻滞组患者有5例患者需增加静脉辅助药物才达到完善的镇痛效果,其中有3例加用右美托咪定1 μg/kg缓慢静脉泵入,2例使用丙泊酚1 mg/kg分次静脉推注。 2.6 不良反应 轻比重腰麻组患者在术中未发生低血压、心动过缓等并发症,术后也未发生头痛、恶心、呕吐等不良反应;神经阻滞组下肢未出现明显异感。"
| [1] Kesmezacar H, Ayhan E, Unlu MC, et al. Predictors of mortality in elderly patients with an intertrochanteric or a femoral neck fracture. J Trauma. 2010; 68(1):153-158.[2] Kanis JA, Oden A, McCloskey EV. A systematic review of hipfracture incidence and probability of fracture worldwide. OsteoporosInt. 2012; 23(9) :2239-2256.[3] Bergstrom U, Johnson H, Gustafson Y, et al. The hip fracture incidence curve is shifting to the right. ActaOrthop. 2009;80(5):520-524.[4] 米勒,邓小明,曾因明. 米勒麻醉学[M]. 北京:北京大学医学出版社, 2011.[5] Cantürk M, K?lc? O, Ornek D, et al. Ropivacaine for unilateral spinal anesthesia; hyperbaric or hypobaric? Rev Bras Anestesiol. 2012; 62(3):298-311.[6] Cooper C, Campion G, Melton L. Hip fractures in the elderly: a worldwide projection. Osteoporos Int. 1992;2(6):285-289. [7] Schurch MA, Rizzoli R, Mermillod B, et al. A prospective study on socioeconomic aspects of fracture of the proximal femur. J Bone Miner Res. 1996;11(12):1935-1942.[8] 毛烨,赵晶,高玉凤,等.右美托咪啶和丙泊酚对老年髋部骨折术后重症患者镇静效果的比较[J].中华医学杂志,2015,95(19):1493-1495.[9] 季英楠,阿良,赵忠海,等.骨折分型及外侧壁厚度对动力髋螺钉治疗外侧壁完整的股骨粗隆间骨折的影响[J].中国医科大学学报,2015,44(9) : 818-821.[10] 刘粤,郝玮,张岩,等. 多学科协作综合治疗老年髋部骨折的疗效[J].中国老年学杂志,2014,34(19) :5481-5484.[11] 王伯尧,王云华,高志强,等.多学科综合治疗对老年髋部骨折预后的影响[J].实用老年医学,2017, 31(12):1121-1131.[12] 杨格,赵猛,徐圣康,建立老年髋部骨折绿色通道的早期疗效分析[J].中国骨与关节损伤杂志年,2017,32(12):1281-1282.[13] 张长青,张伟.我国老年髋部骨折绿色通道建设的现实意义[J].中华创伤骨科杂志,2014,30(3):196-198.[14] Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int. 2004;15(11):897-902. [15] Keene GS, Parker MJ, Pryor GA. Mortality and morbidity after hip fractures. BMJ. 1993;307(6914):1248-1250. [16] Vestergaard P, Rejnmark L, Mosekilde L. Increased mortality in patients with a hip fracture-effect of pre-morbid conditions and post-fracture complications. Osteoporos Int. 2007;18(12):1583-1593. [17] Valizadeh M, Mazloomzadeh S, Golmohammadi S, et al. Mortality after low trauma hip fracture: a prospective cohort study. BMC Musculoskelet Disord. 2012;13:143. [18] Leibson CL, Tosteson AN, Gabriel SE, et al. Mortality, disability, and nursing home use for persons with and without hip fracture: a population-based study. J Am Geriatr Soc. 2002; 50(10):1644-1650.[19] Gijsen R, Hoeymans N, Schellevis FG, et al. Causes and consequencesof comorbidity: a review. J Clin Epidemiol. 2001;54 (7) : 661-674.[20] 胡强,汤守营,郑立生,等.老年髋部骨折患者围术期并发症影响因素分析[J].临床合理用药,2018,11(1):167-168.[21] 塔拉提百克•买买提居马,刘恒. 老年髋部骨折患者住院期间死亡和严重并发症危险因素分析[J].实用骨科杂志,2017,23(10):937-941.[22] Dorotka R, Schoechtner H, Buchinger W. The influence of immediatesurgical treatment of proximal femoral fractures on mortality and qualityof life. Operation within sex hours of the fracture versus lateral thansix hours. J Bone Joint Surg Br.2003;85: 1107-1113.[23] 邓遵生,叶作明,雷廷文,等.骨科老年髋部骨折围手术期内科处理体会[J].中国社区医疗医学专业,2018 ,11(1):167-168.[24] Hoenig H,Rubenstein LV,Sloane R,et al. What is the role of timmingin the surgical and rehabilitative case of community dwelling olderpatients with acture hip fracture. Arch Int Med.1997;157:513-520.[25] Raats JW, van Eijsden WA, Crolla RM, et al. Risk factors and outcomes for postoperative delirium after major surgery in elderly patients. PLoS One. 2015;10(8):e0136071.[26] Ruggiero C, Bonamassa L, Pelini L, et al. Early post-surgical cognitive dysfunction is a risk factor for mortality among hip fracture hospitalized older persons. Osteoporos Int. 2017;28(2):667-675.[27] Mazzola P, Bellelli G, Brogginni V, et al. Postoperative delirium and pre-fracture disability predict 6-month mortality among the oldest old hip fracture patients. Aging Clin Exp Res. 2015;27(1):53-60.[28] Shih YJ, Hsieh CH, Kang TW, et al. General versus spinal anesthesia:which is a risk factor for octogenarian hip fracture repair patients. Int J Gerontol. 2010;4(1):37-42.[29] Parker MJ, Handoll HH, Griffiths R. Anaesthesia for hip fracture surgeryin adults. Cochrane Database Syst Rev. 2004;(4):CD000521.[30] Brandt C, Hott U, Sohr D, et al. Operating room ventilation with laminarairflow shows no protective effect on the surgical site infectionratein orthopedic and abdominal surgery. Ann Surg.2008;248( 5):695-700.[31] Wei B, Zhang H, Xu M, et al. Effect of different anesthetic methods on postoperative outcomes in elderly patients undergoinghip fracture surgery. Beijing Da Xue Xue Bao Yi Xue Ban. 2017;49(6):1008-1013.[32] Guay J, Parker MJ, Gajendragadkar PR, et al. Anaesthesia for hip fracture surgery in adults. Cochrane Database Syst Rev. 2016;2:CD000521.[33] Murthy S, Hepner DL, Cooper Z, et al. Controversies in anaesthesia for noncardiac surgery in older adults. Br J Anaesth. 2015;115(Suppl 2): ii15-25.[34] Roberts KC, Brox WT. AAOS clinical practice guideline: management of hip fractures in the elderly. J Am Acad Orthop Surg. 2015;23:138-140.[35] Wang XT, MA WH, Li RS. Dose-effect relationship of hypobaric ropivacaine in spinal anesthesia in the elderly undergoing hip replacement. J Clin Anesthesiol. 2008.[36] Zhou J, Jia R. Application of spinal anesthesia with ropivacaineor bupivacaine in the elderly. J Clin Anesthesiol. 2006;22(8):580-581.[37] Demirel I, Ozer AB, Duzgol O, et al. Comparison of unilateral spinal anesthesia and L1paravertebral block combined with psoas compartment and sciatic nerve block in patients to undergo partial hip prosthesis. Eur Rev Med Pharmacol Sci. 2014; 18(7):1067-1072.[38] Gamli M, Sacan O, Baskan S, et al. Combined lumbar plexus and sciatic nerve block for hip fracture surgery in a patient with severe aortic stenosis. J Anesthesia. 2011; 25(5):784-785. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [3] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [4] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [5] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [6] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [7] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [8] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [9] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [10] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [11] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [12] | Cheng Chongjie, Yan Yan, Zhang Qidong, Guo Wanshou. Diagnostic value and accuracy of D-dimer in periprosthetic joint infection: a systematic review and meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3921-3928. |
| [13] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [14] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| [15] | Mo Jianling, He Shaoru, Feng Bowen, Jian Minqiao, Zhang Xiaohui, Liu Caisheng, Liang Yijing, Liu Yumei, Chen Liang, Zhou Haiyu, Liu Yanhui. Forming prevascularized cell sheets and the expression of angiogenesis-related factors [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3479-3486. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||