Chinese Journal of Tissue Engineering Research ›› 2024, Vol. 28 ›› Issue (34): 5536-5543.doi: 10.12307/2024.802
Previous Articles Next Articles
Rate of force development and its relationship with functional performance in patients after anterior cruciate ligament reconstruction
Li Qi1, Gao Mingwei2, Li Shihao1, Chu Xiaolei1, Li Yajie2, Ding Ning2, Liu Minqi2
- 1Department of Rehabilitation Medicine, Tianjin University Tianjin Hospital, Tianjin 300211, China; 2Sports and Health College of Tianjin Sport University, Tianjin 301617, China
-
Received:2023-11-30Accepted:2024-01-05Online:2024-12-08Published:2024-03-15 -
Contact:Li Qi, Department of Rehabilitation Medicine, Tianjin University Tianjin Hospital, Tianjin 300211, China -
About author:Li Qi, Master, Associate chief physician, Department of Rehabilitation Medicine, Tianjin University Tianjin Hospital, Tianjin 300211, China -
Supported by:2021 Scientific Research Project of China Medical Association of Minorities, No. 2021Z1063-520701 (to LQ); Tianjin Science and Technology Program, No. 22JCYBJC00210 (to LQ)
CLC Number:
Cite this article
Li Qi, Gao Mingwei, Li Shihao, Chu Xiaolei, Li Yajie, Ding Ning, Liu Minqi. Rate of force development and its relationship with functional performance in patients after anterior cruciate ligament reconstruction[J]. Chinese Journal of Tissue Engineering Research, 2024, 28(34): 5536-5543.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
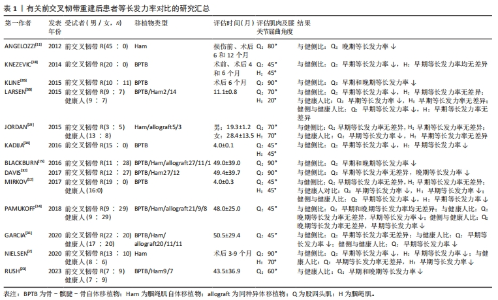
2.1 前交叉韧带重建后患者等长发力率的重要研究概述 在2012年,ANGELOZZI等[11]首次评估前交叉韧带重建后患者的等长发力率,发现其存在显著缺陷,并且与等长峰值力矩存在不同恢复时间,表明等长发力率能够反映除了最大肌力外的其他神经肌肉功能信息。因此在初期研究者主要关注术后患者等长发力率的缺陷情况,包括研究等长发力率的对称性和H∶Q比值[18-19],因为这些比值在最大肌力的应用很广,研究者们试图找出能够反映患者神经肌肉功能缺陷情况的参数,他们发现等长发力率的缺陷情况要高于等长峰值力矩[18],并且更能反映患者的神经受损情况。随后研究者观察到等长发力率能够反映肌肉短时间的发力情况,这和很多功能性活动要求的短时间完成相一致,所以为了了解等长发力率缺陷对功能的影响,不同学者研究了等长发力率与步态、跑步、单腿跳跃性能、侧切等任务的关系[14-15,20-21],发现了等长发力率与功能性运动的相关性要强于等长峰值力矩,改善患者等长发力率可能会降低创伤性膝骨关节炎、二次损伤的风险,并且建议将其作为恢复运动的评价指标之一。考虑到改善等长发力率的重要性,不同学者试图去研究改善等长发力率的方法以及可能机制[22-23],但目前效果尚不清楚。 2.2 等长发力率与等长峰值力矩 等长发力率是在肌肉等长收缩条件下不同时间间隔的力-时间曲线斜率[24],通常用来评估肌肉的爆发力。研究普遍认为早期等长发力率(即肌肉收缩100 ms时间段内任意时间间隔的力-时间曲线斜率)和晚期等长发力率(即肌肉收缩100 ms后时间段内任意时间间隔的力-时间曲线斜率)可能受到不同的神经肌肉机制的影响[11,24-26]。早期等长发力率主要受神经机制影响,而晚期等长发力率主要受肌肉收缩特性影响,具体而言,早期等长发力率反映了神经和肌肉特性对相关时间间隔的综合影响[26-27],包括运动单元放电频率、双重放电和肌纤维类型等,而在评估晚期等长发力率时,这时肌肉的激活已经很多,肌肉的收缩特性占主导,包括肌纤维类型、肌球蛋白重链亚型、肌纤维横截面积和肌腱强度等[27]。 等长发力率与等长峰值力矩之间存在正相关关系[28-29],两者至少部分由不同的神经肌肉特性决定[29]。ANDERSEN等[29]研究了年轻男性膝关节屈曲90°时股四头肌等长峰值力矩和等长发力率的关系,在快速自主收缩的前10,50,100和200 ms内记录的等长发力率,等长峰值力矩分别解释了18%,29%,57%和78%方差,表明等长峰值力矩对晚期等长发力率的影响较大,而对早期等长发力率影响很小。除此之外,等长发力率与等长峰值力矩的短期改善可能需要不同的训练刺激[30],OLIVEIRA等[30]研究了提高爆发力和最大力量的训练对年轻男性膝关节屈曲75°时股四头肌等长峰值力矩和等长发力率的影响,发现训练后早期等长发力率和等长峰值力矩显著增高,而晚期等长发力率无差异。 等长发力率与等长峰值力矩存在不同的恢复时间和不同的缺陷程度[2,11,18],ANGELOZZI等[11]评估了男性职业足球运动员前交叉韧带重建后6,12个月膝关节屈曲80°时股四头肌等长峰值力矩和晚期等长发力率,与损伤前同侧肢体相比,术后6,12个月患侧股四头肌等长峰值力矩均无差异,而术后6个月患侧股四头肌晚期等长发力率显著降低,术后12个月显示无差异,与健侧肢体相比,在患侧发现同样的结果。另外,KNEZEVIC等[18]发现患者术前和术后4个月股四头肌早期等长发力率不对称性均大于股四头肌等长峰值力矩,NIELSEN等[2]还发现与健侧和健康对照组相比,患侧股四头肌早期等长发力率的H∶Q缺陷要高于等长峰值力矩的H∶Q,考虑到早期等长发力率与功能性活动的时间特征相一致,并且较低的H∶Q与损伤风险有关[5],所以更显著的等长发力率缺陷应该受到重视。 2.3 前交叉韧带重建后不同时间段内患者等长发力率的缺陷情况 2.3.1 患侧等长发力率与健侧等长发力率的比较 目前有很多学者进行了患侧等长发力率与健侧等长发力率的相关研究[31-35],关于股四头肌,术后6个月内:大部分研究发现膝关节屈曲45°,90°时早期等长发力率显著降低[2,18,34-35],屈曲80°,90°时晚期等长发力率显著降低[11,35],仅一项研究发现屈曲45°时早期等长发力率无差异[12]。文章发现该研究的受试者群体为国家队运动员[12],在术后早期就开始了加速康复方案,包括高强度力量训练和敏捷训练,而这些训练会显著改善发力率[27],所以他们可能在术后早期就恢复了肢体的对称性。术后7-12个月:较少研究发现膝关节屈曲70°时早期等长发力率显著降低[33],屈曲80°时发现晚期等长发力率无差异[11]。但需要注意的是,结果显示晚期等长发力率无差异的研究中所使用的评估设备不能单独评估膝伸肌的肌力,还会涉及到髋伸肌等肌群,这会补偿股四头肌功能的不足,从而掩盖结果的真实性。术后1年以上:早期和晚期等长发力率均存在争议,大部分研究发现膝关节屈曲45°,70°,90°时早期等长发力率无差异[14,19,31-32],一项研究发现屈曲90°时早期等长发力率降低[15]。对于晚期等长发力率,有研究发现在屈曲45°无差异[14],在屈曲90°降低[15,32]。大部分研究的评估时间在术后约4年,并且发现早期等长发力率对称性有显著改善。 关于腘绳肌,术后6个月:2项研究发现膝关节屈曲45°,70°时早期等长发力率均显著降低[2,34],但另外2项研究在屈曲45°时发现早期等长发力率无差异[12,18]。上述研究中重建大多采用自体骨-髌腱-骨作为移植物,据文章所知,患者通常在移植物供体区部位表现出更大的肌肉功能缺陷[4],而相关研究发现腘绳肌早期等长发力率也有显著降低,这表明前交叉韧带重建导致腘绳肌功能出现了明显的缺陷。所以无论自体移植物选自哪种肌腱,重建后膝关节周围肌群的功能训练都要加强。另外在早期等长发力率无差异的研究中[12,18],受试者均为国家队男性运动员,由于身体素质和训练强度等因素[27],这类患者可能在术后早期就恢复了肢体间的对称性。在术后7-12个月和1年以上,不同时间段内有研究在屈曲20°和70°时发现早期等长发力率无差异[19,33],表明腘绳肌早期等长发力率对称性在术后半年以后有所改善。 2.3.2 患侧等长发力率与健康对照组等长发力率的比较 关于股四头肌,术后6个月:MIRKOV等[12]研究发现膝关节屈曲45°时早期等长发力率降低,而NIELSEN等[2]研究发现膝关节屈曲90°时早期等长发力率无差异。相比于膝关节屈曲90°时评估的股四头肌功能,膝关节屈曲45°时的股四头肌功能缺陷更大,并且与功能表现的相关性更强[36]。另外,2项研究中受试者采取的自体移植物不同,MIRKOV等[12]研究中重建移植物是自体骨-髌腱-骨,这种手术方式对股四头肌功能的损害较大。术后7-12个月:LARSEN等[33]发现膝关节屈曲70°时早期等长发力率降低。术后1年以上:4项研究在膝关节屈曲45°,60°和70°时均发现早期等长发力率显著降低[14,19,23,31],而晚期等长发力率在膝关节屈曲45°时无差异[14],屈曲60°时显著降低[23]。 关于腘绳肌,术后6个月:2项研究在膝关节屈曲45°和90°时均发现早期显著降低[2,12]。在术后7-12个月和1年以上,不同时间段内有研究在屈曲20°和70°时发现早期等长发力率无差异[19,33],这2项研究受试者大多采用腘绳肌自体移植物,这更加说明腘绳肌神经功能在术后半年以上就有显著恢复。但目前尚无屈曲角度超过75°的相关研究,而选用腘绳肌自体移植物的前交叉韧带重建患者的腘绳肌功能在超过75°后会出现明显受损[37-38]。 2.3.3 健侧等长发力率与健康对照组等长发力率的比较 关于股四头肌,在术后6个月和7-12个月,分别有1项研究发现膝关节屈曲45°和70°时早期等长发力率均显著降低[12,33]。术后1年以上:研究发现在膝关节45°时发现早期等长发力率降低[14,31],晚期等长发力率无差异[14]。上述结果表明,健侧肢体股四头肌早期等长发力率在术后可出现长期缺陷。 关于腘绳肌,术后6个月:MIRKOV等[12]研究发现膝关节屈曲45°时早期等长发力率显著降低。术后7-12个月:LARSEN等[33]研究发现膝关节屈曲20°时早期等长发力率无差异。 综上,不管是股四头肌还是腘绳肌,其早期和晚期等长发力率对称性在术后半年内均较差,而大部分研究表明早期等长发力率对称性在术后1年以上均有所改善。前交叉韧带损伤发生后,健侧肢体神经肌肉功能同样受损,并且在术后长期存在[39],与健侧进行比较,可能会掩盖患侧等长发力率的缺陷。在患侧、健侧分别与健康对照组的比较中确实观察到双侧股四头肌早期等长发力率在术后持续受损,所以术后1年以上观察到的股四头肌早期等长发力率对称性有所改善并不是患侧恢复正常,而是健侧也持续受损。而双侧腘绳肌早期等长发力率在术后半年后与健康对照组无差异,说明腘绳肌早期等长发力率对称性确实有所改善,但膝关节屈曲大于75°时腘绳肌的等长发力率尚不清楚,这可能会显示出腘绳肌功能的不足。最理想的比较是与同一侧肢体损伤前的数据进行对比[11],但这很难实现,因此有学者建议将术前健侧数据作为对照[18],可能为对称性提供更有效的评估。有关晚期等长发力率的相关研究较少,无法得出结论。 文章总结了有关前交叉韧带重建后患者等长发力率对比的研究进展,见表1。"

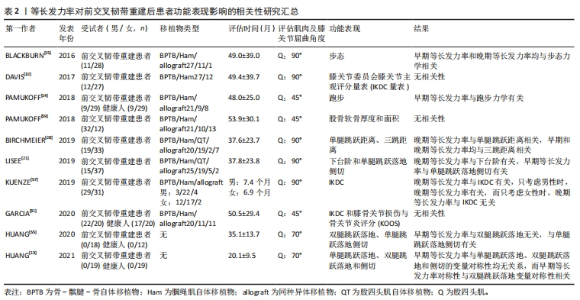
2.4 前交叉韧带重建后患者等长发力率缺陷的潜在神经肌肉机制 前交叉韧带损伤以及重建造成的传入反馈降低可能会导致伽马运动神经元激活减少并且损害脊髓运动神经元的Ⅰa类神经纤维传入,这会导致无法完全激活高阈值运动单元[40]。另外,膝关节感受器传入功能的异常改变导致皮质脊髓兴奋性和脊髓反射兴奋性降低[41-42],这些早期变化会导致中枢神经系统的进一步适应[43],并且在大脑皮质运动区同样发现兴奋性降低[44-45],这会进一步减少自主肌肉的激活,出现关节源性肌肉抑制,造成高阈值运动单元激活受限[46]。在肌肉收缩的初始阶段,Ⅱ型纤维和运动单元放电频率共同影响早期等长发力率的产生,含有Ⅱ型纤维的高阈值运动单元通常具有更快的收缩速度,而较高的放电频率会积极调动Ⅱ型肌纤维的收缩,确保更快的力量上升。但前交叉韧带损伤和重建后,患侧出现关节源性肌肉抑制和伽马运动神经元的反馈抑制,导致在肌肉主动收缩期间无法激活高阈值运动单元[47],从而抑制Ⅱ型肌纤维的收缩,这可能是早期等长发力率缺陷的重要原因。 研究表明重建侧肢体股四头肌体积和面积均较健侧和健康人降低[48-49],这同样在腘绳肌中发现[50]。另外从细胞和形态学方面观察到Ⅱa型纤维选择性减少,而Ⅱa/x混合型纤维选择性增加,并且伴有细胞外基质体积增加,这些改变可能是前交叉韧带重建后观察到肌肉产生力量能力下降的原因[51-52],考虑到肌肉体积和横截面积以及肌束的成角会影响等长峰值力矩的产生能力[53],而等长峰值力矩对晚期等长发力率的影响较大[29],所以这些肌肉因素的改变可能是晚期等长发力率缺陷的重要原因,除了肌肉组织,肌腱的刚度同样会影响晚期等长发力率的产生,BOJSEN-MOLLER等[54]发现肌腱-腱膜复合体的刚度能够解释晚期等长发力率的30%方差。 尽管神经因素和肌肉因素可能分别是早期和晚期等长发力率缺陷的重要原因,但很难确定神经和肌肉因素对等长发力率能力的具体贡献[16]。早期和晚期等长发力率可能受到神经和肌肉因素的共同影响[26-27],而影响的程度大小不同,因此文章只是分别概述了影响早期和晚期等长发力率主要的潜在因素。 2.5 等长发力率与功能表现的关系 2.5.1 跳跃能力 BIRCHMEIER等[20]发现股四头肌等长峰值力矩和晚期等长发力率与单腿跳远距离呈正相关,股四头肌等长峰值力矩、早期等长发力率和晚期等长发力率与单腿三跳距离呈正相关。单腿跳跃距离作为前交叉韧带重建后患者是否回归运动的重要评估指标之一[20],并未发现与早期等长发力率有相关性,而在单腿三跳距离方面,等长峰值力矩解释了其6.6%的方差,高于早期等长发力率的3.1%和晚期等长发力率的4.6%。所以不论是一次跳跃还是连续3次跳跃,肌肉最大力量的贡献都是高于早期等长发力率,这表明跳跃距离的评估可能不能反映前交叉韧带重建后患者神经功能的缺陷,另外需要寻找一种能够反映患者神经肌肉功能的简单方便、可实施的测试来作为患者能否回归运动的评估手段之一。 另外,HUANG等[13]发现股四头肌早期等长发力率无法预测单腿跳跃落地和双腿跳跃落地运动中100 ms内的膝关节矢状面净力矩、垂直地面反作用力峰值以及平均负荷率的肢体对称性,而早期等长发力率对称性与双腿跳跃落地运动中膝关节矢状面净力矩对称性呈正相关。以往的一项研究表明发生二次损伤的患者比一次损伤患者在着陆时膝关节矢状面净力矩存在更大的不对称性[56],所以通过增加患侧等长发力率来减少发力率不对称性可能会降低前交叉韧带二次损伤的风险。HUANG等[55]的另一项研究还发现股四头肌早期等长发力率与双腿跳跃落地运动中100 ms内的动力学参数和运动学参数均无相关性。双腿任务相比于单腿任务需要激活更多的大脑区域。研究发现前交叉韧带重建后患者双腿同时进行股四头肌等长发力率测试时,患侧股二头肌激活程度要高于健侧,而在分别测试两侧肢体时并未发现[10],所以对于双腿任务来说,只进行患侧股四头肌等长发力率的评估似乎无法反映双腿任务的能力。 2.5.2 侧切 HUANG等[13]分析了股四头肌早期等长发力率对侧切任务中100 ms内膝关节矢状面净力矩、垂直地面反作用力峰值和平均负荷率肢体对称性的影响,但未发现早期等长发力率与任何动力学参数对称性有相关性。而HUANG等[55]的另一项研究分析了股四头肌早期等长发力率对单腿跳跃落地侧切任务中运动学和动力学参数的影响,发现早期等长发力率与平均负荷率(垂直地面反作用力峰值/达峰值时间)呈负相关,而与达垂直地面反作用力峰值时间呈正相关,与运动学参数无关,即等长发力率越大,负荷率越低,达垂直地面反作用力峰值时间越长。但是LISEE等[21]在股四头肌早期等长发力率与单腿跳跃落地侧切任务关系的研究中发现了不同的结果,他们发现早期等长发力率无法预测平均负荷率,却发现早期等长发力率与初始触地时膝关节屈曲角度和膝关节屈曲角度峰值呈正相关。在单腿侧切任务中观察到早期等长发力率与动力学参数对称性无关,这在单腿跳跃落地任务中也同样发现[13],这表明仅评估患侧股四头肌等长发力率可能无法预测单腿任务中的对称性指标。 2.5.3 日常生活活动(下台阶、走和跑) LISEE等[21]研究了股四头肌等长峰值力矩、早期和晚期等长发力率对下台阶任务的影响,发现只有晚期等长发力率与下台阶任务中膝关节峰值伸展力矩呈正相关。关于步态的研究,BLACKBURN等[15]发现股四头肌早期等长发力率与平均负荷率(垂直地面反作用力峰值/达峰值时间)、瞬时负荷率(力-时间曲线的一阶导数峰值)、足跟撞击力(heelstrike transient,HST)以及HST瞬时负荷率呈负相关,晚期等长发力率与平均负荷率呈负相关。 除此之外,PAMUKOFF等[14]研究了股四头肌等长峰值力矩、等速峰值力矩、早期和晚期等长发力率与跑步动力学参数的关系,发现只有等速峰值力矩和早期等长发力率与跑步过程中膝关节伸展发力率(站立阶段时间的10%-30%曲线斜率)呈正相关。上述三项日常生活功能均未发现与等长峰值力矩有相关性,但都和等长发力率有关,尤其是早期等长发力率,功能性活动往往在短时间内完成,而早期等长发力率更能反映肌肉对功能性活动的影响。 2.5.4 自我报告的身体功能 KUENZE等[57]研究了股四头肌等长峰值力矩、早期和晚期等长发力率对国际膝关节委员会膝关节主观评分量表(IKDC量表)的影响,IKDC量表用于量化膝关节损伤对患者报告的功能和日常生活活动的影响,得分越高表明患者功能越好。研究仅发现晚期等长发力率与IKDC量表呈正相关,当只考虑男性时,发现晚期等长发力率能够解释IKDC量表的27.7%方差,但只考虑女性时,晚期等长发力率与IKDC量表无相关性。这表明等长发力率和自我报告的膝关节功能之间的关系会受到性别的影响。DAVIS等[32]却发现了相反的结果,即IKDC与股四头肌等长峰值力矩有关,而与等长发力率相关性不大。甚至在GARCIA等[31]的研究中并未发现股四头肌等长峰值力矩和早期等长发力率与IKDC量表有关,并且也与膝骨关节损伤与骨关节炎评分(KOOS)量表无关。以往研究发现患者股四头肌功能和自我报告的身体功能的相关性与术后评估时间有关,术后早期有强相关性[58],而DAVIS和GARCIA等评估时间平均为术后约4年,这可能部分解释了低相关性的原因。 2.5.5 其他 有一项研究分析了股四头肌等长峰值力矩、早期和晚期等长发力率与股骨软骨成分的关系[59],但仅发现等长峰值力矩与股骨内侧髁软骨厚度呈正相关,并未发现等长发力率与股骨软骨成分有相关性。 文章总结了等长发力率对前交叉韧带重建后患者功能表现影响的相关性研究进展,见表2。"


2.6 振动训练对前交叉韧带重建后患者等长发力率影响 PAMUKOFF 等[60]研究了6次1 min的全身振动和局部振动训练(加速度:2×g;频率:30 Hz)对股四头肌早期和晚期等长发力率的即刻效应,发现只有全身振动训练显著提高了早期等长发力率,以往的研究已经表明振动训练能够改善关节源性肌肉抑制[61],并且增强皮质兴奋性[62],这可能解释了只观察到早期等长发力率改善的原因。而TROY BLACKBURN等[22]在进行同样的干预后却发现两种振动训练都无法立刻改善患者股四头肌等长发力率(早期和晚期等长发力率),并且在随后的10,20,30,45和60 min时间点也并未出现改善。"

| [1] 陈连旭,付立功.前交叉韧带断裂和重建的临床流行病学分析[J].中国组织工程研究,2016,20(24):3602-3608. [2] NIELSEN JL, ARP K, VILLADSEN ML, et al. Rate of force development remains reduced in the knee flexors 3 to 9 months after anterior cruciate ligament reconstruction using medial hamstring autografts: a cross-sectional study. Am J Sports Med. 2020;48:3214-3223. [3] LISEE C, LEPLEY AS, BIRCHMEIER T, et al. Quadriceps strength and volitional activation after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Sports Health. 2019;11:163-179. [4] THOME R, KAPLAN Y, KVIST J, et al. Muscle strength and hop performance criteria prior to return to sports after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2011;19:1798-1805. [5] ZEBIS MK, ANDERSEN LL, ELLINGSGAARD H, et al. Rapid hamstring/quadriceps force capacity in male vs. female elite soccer players. J Strength Cond Res. 2011;25:1989-1993. [6] ARDERN CL, WEBSTER KE, TAYLOR NF, et al. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med. 2011;45:596-606. [7] HUI C, SALMON LJ, KOK A, et al. Fifteen-year outcome of endoscopic anterior cruciate ligament reconstruction with patellar tendon autograft for “isolated” anterior cruciate ligament tear. Am J Sports Med. 2011;39:89-98. [8] KOGA H, NAKAMAE A, SHIMA Y, et al. Mechanisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. Am J Sports Med. 2010;38:2218-2225. [9] LEPLEY AS, GROOMS DR, BURLAND JP, et al. Quadriceps muscle function following anterior cruciate ligament reconstruction: systemic differences in neural and morphological characteristics. Exp Brain Res. 2019;237:1267-1278. [10] DI GIMINIANI R, MARINELLI S, LA GRECA S, et al. Neuromuscular characteristics of unilateral and bilateral maximal voluntary isometric contractions following ACL reconstruction. Biology (Basel). 2023;12:1173. [11] ANGELOZZI M, MADAMA M, CORSICA C, et al. Rate of force development as an adjunctive outcome measure for return-to-sport decisions after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 2012;42:772-780. [12] MIRKOV DM, KNEZEVIC OM, MAFFIULETTI NA, et al. Contralateral limb deficit after ACL-reconstruction: an analysis of early and late phase of rate of force development. J Sports Sci. 2017;35:435-440. [13] HUANG YL, MULLIGAN CMS, JOHNSON ST, et al. Explosive quadriceps strength symmetry and landing mechanics limb symmetry after anterior cruciate ligament reconstruction in females. J Athl Train. 2021;56:912-921. [14] PAMUKOFF DN, MONTGOMERY MM, CHOE KH, et al. Bilateral alterations in running mechanics and quadriceps function following unilateral anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 2018;48:960-967. [15] BLACKBURN JT, PIETROSIMONE B, HARKEY MS, et al. Quadriceps function and gait kinetics after anterior cruciate ligament reconstruction. Med Sci Sports Exerc. 2016;48:1664-1670. [16] TURPEINEN JT, FREITAS TT, RUBIO-ARIAS J, et al. Contractile rate of force development after anterior cruciate ligament reconstruction-a comprehensive review and meta-analysis. Scand J Med Sci Sports. 2020;30: 1572-1585. [17] WILSON GJ, MURPHY AJ. The use of isometric tests of muscular function in athletic assessment. Sports Med. 1996;22:19-37. [18] KNEZEVIC OM, MIRKOV DM, KADIJA M, et al. Asymmetries in explosive strength following anterior cruciate ligament reconstruction. Knee. 2014; 21:1039-1045. [19] JORDAN MJ, AAGAARD P, HERZOG W. Rapid hamstrings/quadriceps strength in ACL-reconstructed elite Alpine ski racers. Med Sci Sports Exerc. 2015;47:109-119. [20] BIRCHMEIER T, LISEE C, GEERS B, et al. Reactive strength index and knee extension strength characteristics are predictive of single-leg hop performance after anterior cruciate ligament reconstruction. J Strength Cond Res. 2019;33:1201-1207. [21] LISEE C, BIRCHMEIER T, YAN A, et al. Associations between isometric quadriceps strength characteristics, knee flexion angles, and knee extension moments during single leg step down and landing tasks after anterior cruciate ligament reconstruction. Clin Biomech (Bristol, Avon). 2019;70:231-236. [22] TROY BLACKBURN J, DEWIG DR, JOHNSTON CD. Time course of the effects of vibration on quadriceps function in individuals with anterior cruciate ligament reconstruction. J Electromyogr Kinesiol. 2021;56:102508. [23] RUSH JL, NORTE GE. Hamstrings fatigue does not improve quadriceps function in individuals with anterior cruciate ligament reconstruction. Phys Ther Sport. 2023;61:20-26. [24] AAGAARD P, SIMONSEN EB, ANDERSEN JL, et al. Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol (1985). 2002;93:1318-1326. [25] FOLLAND JP, BUCKTHORPE MW, HANNAH R. Human capacity for explosive force production: neural and contractile determinants. Scand J Med Sci Sports. 2014;24:894-906. [26] RODR GUEZ-ROSELL D, PAREJA-BLANCO F, AAGAARD P, et al. Physiological and methodological aspects of rate of force development assessment in human skeletal muscle. Clin Physiol Funct Imaging. 2018;38:743-762. [27] MAFFIULETTI NA, AAGAARD P, BLAZEVICH AJ, et al. Rate of force development: physiological and methodological considerations. Eur J Appl Physiol. 2016; 116:1091-1116. [28] PREBEG G, CUK I, SUZOVIC D, et al. Relationships among the muscle strength properties as assessed through various tests and variables. J Electromyogr Kinesiol. 2013;23:455-461. [29] ANDERSEN LL, AAGAARD P. Influence of maximal muscle strength and intrinsic muscle contractile properties on contractile rate of force development. Eur J Appl Physiol. 2006;96:46-52. [30] OLIVEIRA FB, OLIVEIRA AS, RIZATTO GF, et al. Resistance training for explosive and maximal strength: effects on early and late rate of force development. J Sports Sci Med. 2013;12:402-408. [31] GARCIA SA, MOFFIT TJ, VAKULA MN, et al. Quadriceps muscle size, quality, and strength and self-reported function in individuals with anterior cruciate ligament reconstruction. J Athl Train. 2020;55:246-254. [32] DAVIS HC, TROY BLACKBURN J, RYAN ED, et al. Quadriceps rate of torque development and disability in individuals with anterior cruciate ligament reconstruction. Clin Biomech (Bristol, Avon). 2017;46:52-56. [33] LARSEN JB, FARUP J, LIND M, et al. Muscle strength and functional performance is markedly impaired at the recommended time point for sport return after anterior cruciate ligament reconstruction in recreational athletes. Hum Mov Sci. 2015;39:73-87. [34] KADIJA M, KNEZEVIĆ OM, MILOVANOVIĆ D, et al. The effect of anterior cruciate ligament reconstruction on hamstring and quadriceps muscle function outcome ratios in male athletes. Srp Arh Celok Lek. 2016;144: 151-157. [35] KLINE PW, MORGAN KD, JOHNSON DL, et al. Impaired quadriceps rate of torque development and knee mechanics after anterior cruciate ligament reconstruction with patellar tendon autograft. Am J Sports Med. 2015;43: 2553-2558. [36] KRISHNAN C, THEUERKAUF P. Effect of knee angle on quadriceps strength and activation after anterior cruciate ligament reconstruction. J Appl Physiol (1985). 2015;119:223-231. [37] JOHNSON AK, PALMIERI-SMITH RM, LEPLEY LK. Contribution of neuromuscular factors to quadriceps asymmetry after anterior cruciate ligament reconstruction. J Athl Train. 2018;53:347-354. [38] SHARMA A, FLANIGAN DC, RANDALL K, et al. Does gracilis preservation matter in anterior cruciate ligament reconstruction? a systematic review. Arthroscopy. 2016;32:1165-1173. [39] CHUNG KS, HA JK, YEOM CH, et al. Are muscle strength and function of the uninjured lower limb weakened after anterior cruciate ligament injury? Two-year follow-up after reconstruction. Am J Sports Med. 2015;43:3013-3021. [40] KONISHI Y, FUKUBAYASHI T, TAKESHITA D. Mechanism of quadriceps femoris muscle weakness in patients with anterior cruciate ligament reconstruction. Scand J Med Sci Sports. 2002;12:371-375. [41] LEPLEY AS, GRIBBLE PA, THOMAS AC, et al. Quadriceps neural alterations in anterior cruciate ligament reconstructed patients: a 6-month longitudinal investigation. Scand J Med Sci Sports. 2015;25:828-839. [42] LEPLEY AS, ERICKSEN HM, SOHN DH, et al. Contributions of neural excitability and voluntary activation to quadriceps muscle strength following anterior cruciate ligament reconstruction. Knee. 2014;21:736-742. [43] NEEDLE AR, LEPLEY AS, GROOMS DR. Central nervous system adaptation after ligamentous injury: a summary of theories, evidence, and clinical interpretation. Sports Med. 2017;47:1271-1288. [44] BAUMEISTER J, REINECKE K, SCHUBERT M, et al. Altered electrocortical brain activity after ACL reconstruction during force control. J Orthop Res. 2011;29:1383-1389. [45] BAUMEISTER J, REINECKE K, WEISS M. Changed cortical activity after anterior cruciate ligament reconstruction in a joint position paradigm: an EEG study. Scand J Med Sci Sports. 2008;18:473-484. [46] PIETROSIMONE B, LEPLEY AS, KUENZE C, et al. Arthrogenic muscle inhibition following anterior cruciate ligament injury. J Sport Rehabil. 2022;31:694-706. [47] RICE DA, MCNAIR PJ. Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Semin Arthritis Rheum. 2010;40: 250-266. [48] BIRCHMEIER T, LISEE C, KANE K, et al. Quadriceps muscle size following acl injury and reconstruction: a systematic review. J Orthop Res. 2020;38:598-608. [49] KONISHI Y, IKEDA K, NISHINO A, et al. Relationship between quadriceps femoris muscle volume and muscle torque after anterior cruciate ligament repair. Scand J Med Sci Sports. 2007;17:656-661. [50] KONISHI Y, FUKUBAYASHI T. Relationship between muscle volume and muscle torque of the hamstrings after anterior cruciate ligament reconstruction. J Sci Med Sport. 2010;13:101-105. [51] NOEHREN B, ANDERSEN A, HARDY P, et al. Cellular and morphological alterations in the vastus lateralis muscle as the result of ACL injury and reconstruction. J Bone Joint Surg Am. 2016;98:1541-1547. [52] GUMUCIO JP, SUGG KB, ENSELMAN ERS, et al. Anterior cruciate ligament tear induces a sustained loss of muscle fiber force production. Muscle Nerve. 2018;58:1. [53] ARDERN CL, WEBSTER KE. Knee flexor strength recovery following hamstring tendon harvest for anterior cruciate ligament reconstruction: a systematic review. Orthop Rev (Pavia). 2009;1:1-7. [54] BOJSEN-MOLLER J, MAGNUSSON SP, RASMUSSEN LR, et al. Muscle performance during maximal isometric and dynamic contractions is influenced by the stiffness of the tendinous structures. J Appl Physiol (1985). 2005;99:986-994. [55] HUANG YL, CHANG E, JOHNSON ST, et al. Explosive quadriceps strength and landing mechanics in females with and without anterior cruciate ligament reconstruction. Int J Environ Res Public Health. 2020;17:7431. [56] PATERNO MV, SCHMITT LC, FORD KR, et al. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med. 2010;38:1968-1978. [57] KUENZE C, LISEE C, BIRCHMEIER T, et al. Sex differences in quadriceps rate of torque development within 1 year of ACL reconstruction. Phys Ther Sport. 2019;38:36-43. [58] BODKIN S, GOETSCHIUS J, HERTEL J, et al. Relationships of muscle function and subjective knee function in patients after ACL reconstruction. Orthop J Sports Med. 2017;5:2325967117719041. [59] PAMUKOFF DN, MONTGOMERY MM, MOFFIT TJ, et al. Quadriceps function and knee joint ultrasonography after ACL reconstruction. Med Sci Sports Exerc. 2018;50:211-217. [60] PAMUKOFF DN, PIETROSIMONE B, RYAN ED, et al. Whole-body vibration improves early rate of torque development in individuals with anterior cruciate ligament reconstruction. J Strength Cond Res. 2017;31:2992-3000. [61] BLACKBURN JT, PAMUKOFF DN, SAKR M, et al. Whole body and local muscle vibration reduce artificially induced quadriceps arthrogenic inhibition. Arch Phys Med Rehabil. 2014;95:2021-2028. [62] PAMUKOFF DN, PIETROSIMONE B, LEWEK MD, et al. Whole-body and local muscle vibration immediately improve quadriceps function in individuals with anterior cruciate ligament reconstruction. Arch Phys Med Rehabil. 2016;97:1121-1129. [63] HART HF, CULVENOR AG, COLLINS NJ, et al. Knee kinematics and joint moments during gait following anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Br J Sports Med. 2016;50:597-612. [64] GONNELLI F, REJC E, FLOREANI M, et al. Effects of NMES-elicited versus voluntary low-level conditioning contractions on explosive knee extensions. J Musculoskelet Neuronal Interact. 2022;22:465-473. [65] NAKANISHI R, TAKEUCHI K, AKIZUKI K, et al. The effect of neuromuscular electrical stimulation on muscle EMG activity and the initial phase rate of force development during tetanic contractions in the knee extensor muscles of healthy adult males. Phys Ther Res. 2020;23:195-201. [66] KNAFLITZ M, MERLETTI R, DE LUCA CJ. Inference of motor unit recruitment order in voluntary and electrically elicited contractions. J Appl Physiol (1985). 1990;68:1657-1667. [67] DEAN JC, YATES LM, COLLINS DF. Turning on the central contribution to contractions evoked by neuromuscular electrical stimulation. J Appl Physiol (1985). 2007;103:170-176. [68] HE X, LEONG HT, LAU OY, et al. Altered neuromuscular activity of the lower-extremities during landing tasks in patients with anterior cruciate ligament reconstruction: a systematic review of electromyographic studies. J Sport Rehabil. 2020;29:1194-1203. [69] BUTLER RJ, MINICK KI, FERBER R, et al. Gait mechanics after ACL reconstruction: implications for the early onset of knee osteoarthritis. Br J Sports Med. 2009;43:366-370. |
| [1] | Li Xiaoqiang, Chen Wei, Li Mingyue, Shan Tianchi, Shen Wen. Value of preoperative quantitative ultrasound analysis of quadriceps femoris in predicting chronic post-surgical pain after total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(9): 1388-1393. |
| [2] | Yu Weijie, Liu Aifeng, Chen Jixin, Guo Tianci, Jia Yizhen, Feng Huichuan, Yang Jialin. Advantages and application strategies of machine learning in diagnosis and treatment of lumbar disc herniation [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(9): 1426-1435. |
| [3] | Bai Chen, Yang Wenqian, Meng Zhichao, Wang Yuze. Strategies for repairing injured anterior cruciate ligament and promoting graft healing [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(9): 1457-1463. |
| [4] | Lin Zeyu, Xu Lin. Research progress in gout-induced bone destruction mechanism [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(8): 1295-1300. |
| [5] | Ma Shuwei, He Sheng, Han Bing, Zhang Liaoyun. Exosomes derived from mesenchymal stem cells in treatment of animals with acute liver failure: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(7): 1137-1142. |
| [6] | Zhang Kefan, Shi Hui. Research status and application prospect of cytokine therapy for osteoarthritis [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(6): 961-967. |
| [7] | Li Jiaqi, Huang Yuanli, Li Yan, Wang Chunren, Han Qianqian. Mechanism and influencing factors in molecular weight degradation of non-cross-linked hyaluronic acid [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(5): 747-752. |
| [8] | Xu Rong, Wang Haojie, Geng Mengxiang, Meng Kai, Wang Hui, Zhang Keqin, Zhao Huijing. Research advance in preparation and functional modification of porous polytetrafluoroethylene artificial blood vessels [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(5): 759-765. |
| [9] | Chen Xiaofang, Zheng Guoshuang, Li Maoyuan, Yu Weiting. Preparation and application of injectable sodium alginate hydrogels [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(5): 789-794. |
| [10] | Liu Chuang, Shan Shuo, Yu Tengbo, Zhou Huan, Yang Lei. Advantages, discomfort and challenges of clinical application of orthopedic hemostatic materials [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(5): 795-803. |
| [11] | Zhang Ming, Wang Bin, Jia Fan, Chen Jie, Tang Wei. Application of brain-computer interface technology based on electroencephalogram in upper limb motor function rehabilitation of stroke patients [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(4): 581-586. |
| [12] | He Yuanjie, Chen Yuheng, Zhao Yongchao, Wang Zhenglong. Progress in epigenetic regulation of vascular smooth muscle cell remodeling in the occurrence and development of aortic aneurysms [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(4): 602-608. |
| [13] | Ma Sicong, Chen Jing, Li Yunqing. Functions and roles of connective tissue growth factor in nervous systems [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(4): 615-620. |
| [14] | Yan Binghan, Li Zhichao, Su Hui, Xue Haipeng, Xu Zhanwang, Tan Guoqing. Mechanisms of traditional Chinese medicine monomers in the treatment of osteoarthritis by targeting autophagy [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(4): 627-632. |
| [15] | Wang Juan, Wang Ling, Zuo Huiwu, Zheng Cheng, Wang Guanglan, Chen Peng. Rehabilitative efficacy of kinesio taping following anterior cruciate ligament reconstruction: a Meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2024, 28(4): 651-656. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||