One complication of OWHTO is the change of patellar location, especially the patellar height[25], which would result in the progress of patellofemoralr arthritis and anterior knee pain. However, no consistent results have been achieved[11-13], so it is necessary to establish an effective, simple and reproducible evaluation method for OWHTO. The four methods in the present study are the most popular and widely used all over the world for their simplicity. However, each method has its limitations. According to the their anatomical characteristics, the exact identification of tibial tubercle is not always easy, which easily affect the accuracy of IS index and MIS index[26]. BP index and CD index are associated with the tibial plateau, which may not clear enough to identify, especially in knee osteoarthritis[26].
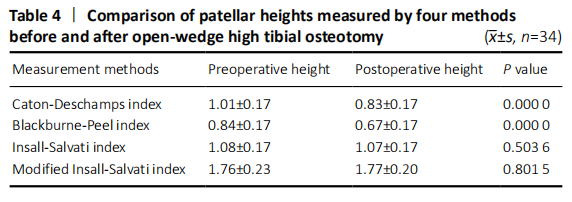
In the present study, our group measured patellar height through four widely used methods-CD, BP, IS and MIS indices. We found that the PH did not change significantly after HTO according to IS and MIS indices, but decreased according to CD and BP indices. A possible reason in our results indicates that the joint line elevation may play a vital role for influencing the change of patellar height[27]. The OWHTO led to elevation of the joint line due to an elongation of the proximal tibial, which resulted in the depression of the patella[28]. Additionally, owing to no direct contact with patellar tendon, little stimulation and no scarring in the early stage after surgery, there was no change in the length of the patellar tendon reasonably[29]. Hence, the PH changes depend on the length of the patellar tendon. This can explain the changes in both CD and BP, but not in IS and MIS. This result was also in consistent with previous study[30].
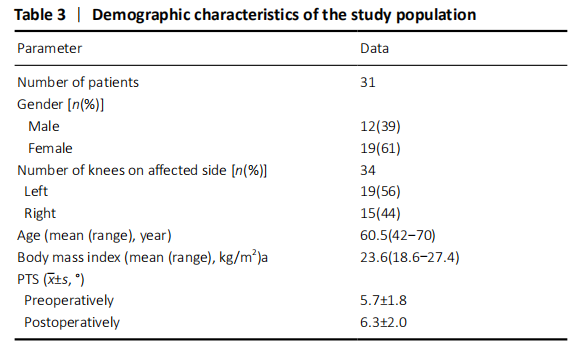
However, PTS and BP index were proved going hand in hand[27, 31], because the enlargement of PTS would elevate the anterosuperior angle of the tibial plateau simultaneously. Several studies found that PTS was increased after OWHTO[32, 33]. To overcome this unplanned change of PTS, Noyes et al.[34] suggested that the opening gap at the posteromedial cortex should be kept twice as wide as the gap at the tibial tuberosity. Hinterwimmer et al.[35] and Hernigou et al.[36] advised that placing the plate at the poster medial corner of the tibia as closely as possible and making a complete posterior osteotomy can preserve the original PTS. We followed their protocol in our study and found that there was an insignificant change in PTS (Table 3). Recently, Kaya et al.[13] recommended posteromedial OWHTO to prevent PTS Increase. In addition, one study reported that oversized correction gap would lead to increase of PTS and decrease of patellar height[37]. When the correction angle was too large, especially more than 12°, surgeons should pay attention to the change of patellar height, take some measures to maintain it and even consider modified HTO or other surgical approaches[37-39].
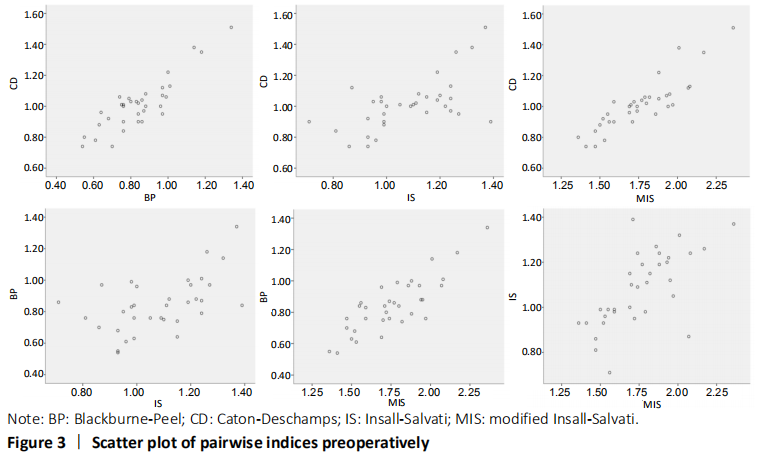
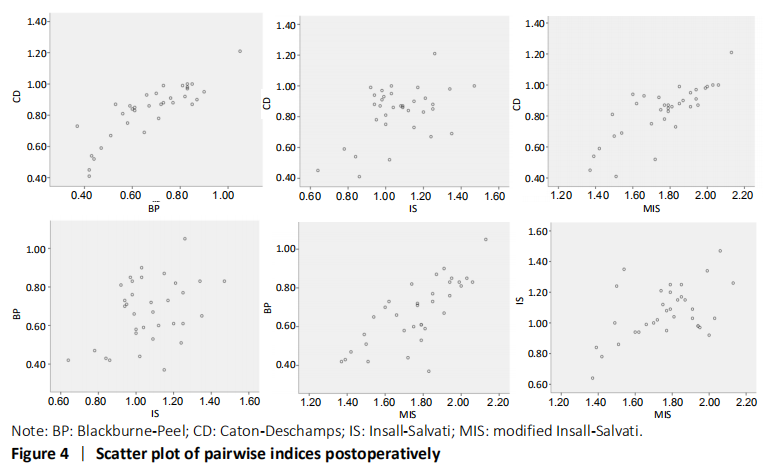
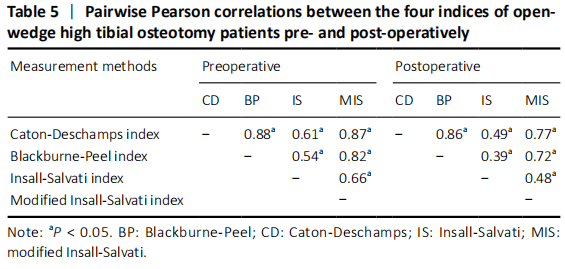
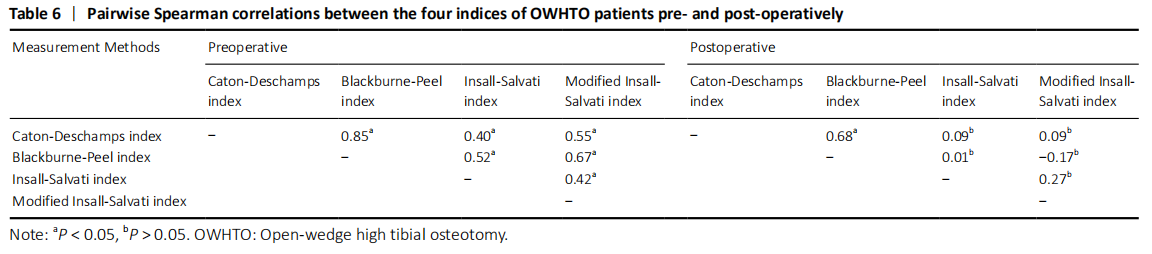
We also evaluated correlation among the 4 methods, and naturally found that among the quantitative correlations, BP and CD indices were best correlated with each other. It is possibly clarified by the fact that the two indices possess the similar measuring method. As for IS index, it offered a lower correlation with the other 3 indices, reflecting some restrictions of this method. In fact, it has been found that IS was responsible for maintaining the constant distance between the tibial tuberosity and the tibial plateau[26], and was not concerned with the anatomic variability of patellar shape[26, 40]. Moreover, in the qualitative analysis, CD and BP indices still showed the highest correlations among the four methods.
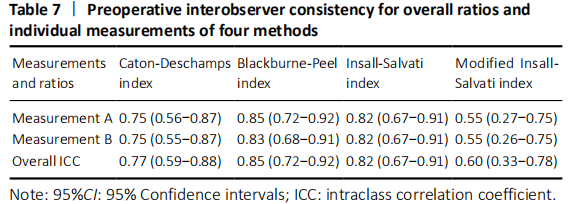
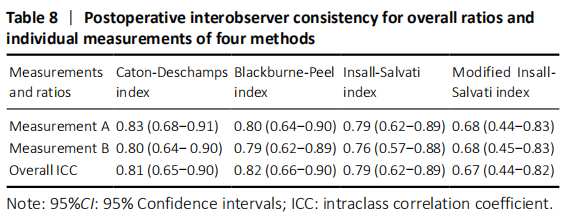
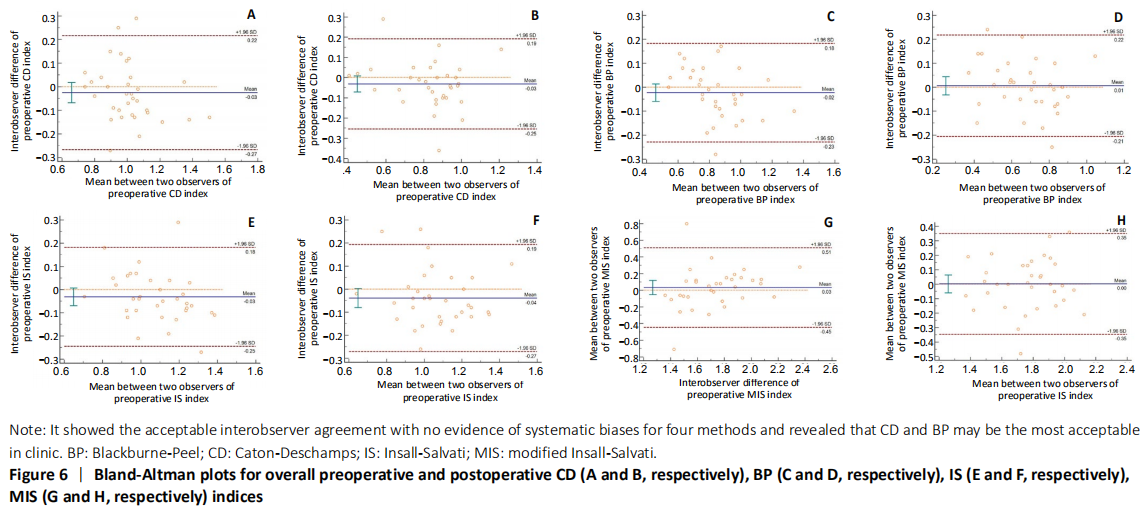
For the four indices measured, we achieved high ICC in CD, BP and IS. In particularly, BP and IS were found the highest interobserver agreement before operation. CD and BP were found to be the highest ICC after operation. In our study, these results were not only in consonance with the statistical results evaluated by Bland-Altman plots but also very close to the results described previously[41].
Accompanied by evident strengths, several limitations also exist in this study. Our study was an imaging article without clinical correlations among the four patellar height assessment methods, because the primary goal of the study was to evaluate their consistency and reproducibility. Furthermore, we simply assessed the four kinds of parameters preoperatively and 6 months postoperatively without long-dated follow-up, in which bone healing almost finishes without the loss of osteotomy gap and there is change of tibial plateau, which can veritably reflect effects of surgical techniques in early stage after OWHTO. Another limitation was the small sample size, which was resulted from the strict screening of high-quality radiographs. In addition, X-ray employed in this study was not as accurate and clear as CT scan due to the superposition of anatomical landmarks, but it will never conceal the advantages of its faster speed, lower costs, less radiation dose and convenience for follow up.
In conclusion, there was no decrease of the patellar height according to IS and MIS in the six-month follow up period after OWHTO. However, while considering variation of the tibial plateau, patellar height significantly decreased according to BP and CD, which means that OWHTO is strongly related to the tibial joint line elevation. After a systematic consideration of the better inter-and intra-observer agreement and correlation coefficient, we recommend preferentially the use of BP for evaluating patellar height, and secondly the use of CD. Due to the small sample size and the lack of clinical assessment, further larger-sample investigations are required to assess long-term changes of PH and their clinical relevance.
中国组织工程研究杂志出版内容重点:人工关节;骨植入物;脊柱;骨折;内固定;数字化骨科;组织工程