Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (8): 1275-1280.doi: 10.3969/j.issn.2095-4344.0148
Previous Articles Next Articles
Complications associated with bone transport: a literature review of nonunion at the docking site
Liang Bin, Zhang Kai
- Department of Traumatic Orthopedics, Binzhou Medical University Hospital, Binzhou 256600, Shandong Province, China
-
Received:2017-10-26Online:2018-03-18Published:2018-03-18 -
Contact:Zhang Kai, Professor, Chief physician, Master’s supervisor, Department of Traumatic Orthopedics, Binzhou Medical University Hospital, Binzhou 256600, Shandong Province, China -
About author:Liang Bin, Master candidate, Department of Traumatic Orthopedics, Binzhou Medical University Hospital, Binzhou 256600, Shandong Province, China
CLC Number:
Cite this article
Liang Bin, Zhang Kai. Complications associated with bone transport: a literature review of nonunion at the docking site[J]. Chinese Journal of Tissue Engineering Research, 2018, 22(8): 1275-1280.
share this article

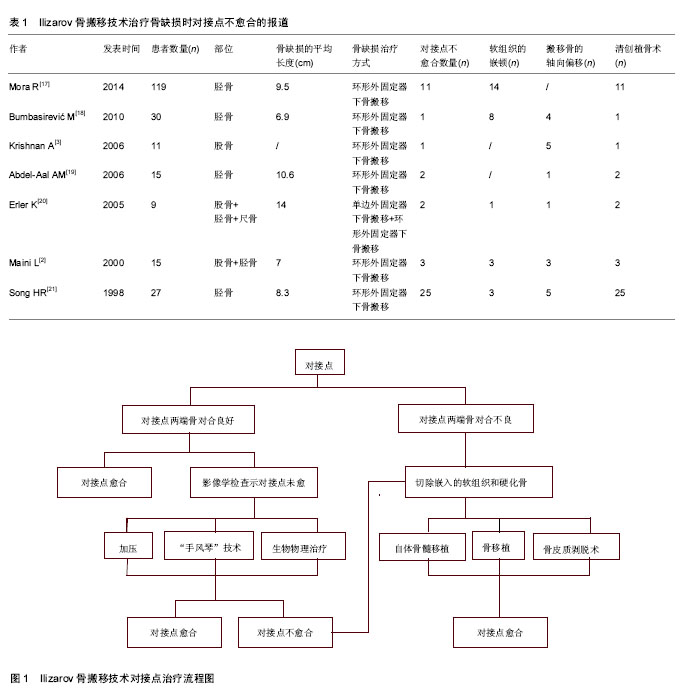
2.1 骨搬移技术概述 长骨大段骨缺损的传统治疗方法主要包括截肢、骨移植、带血管蒂腓骨移植等。截肢是治疗严重肢体损伤的有效方法,但截肢后患者会面临部分肢体功能的缺矢,幻肢痛等一系列问题。而且截肢与保肢的手术指征也存在着争议,从保肢的观点上看,截肢是治疗长骨骨缺损的最终治疗方法[1-2]。骨移植联合髓内钉或钢板内固定是治疗长骨骨缺损的经典方法,骨移植虽可填补长骨大段骨缺损,但不易纠正患肢肢体的短缩,且这种方法受很多因素的限制。例如,大量自体骨的来源问题,骨折固定难度较大,内固定产生的应力遮挡使骨愈合周期延长,且去除内固定物后易发生再骨折等[1,3-4]。带血管蒂腓骨移植是重建长骨骨缺损的有效的治疗方法,吻合血管的腓骨移植因具有丰富的血供,因此具有较强的成骨能力,但切除部分腓骨后会影响踝关节的稳定性,易造成供骨肢体的疼痛,而且对骨科医师要求较高的显微外科技术[1]。大量的临床研究和动物实验发现Ilizarov骨搬移技术是治疗长骨骨缺损的有效方法[5]。 骨搬移技术是前苏联骨科医师伊里扎洛夫教授创造的最为独特的骨缺损治疗方法,经过多年对牵拉成骨的基础实验研究和对外固定装置的改进,骨搬移技术除可治疗严重的开放性骨折外,还可治疗严重的骨折并发症,如肢体的短缩和关节的挛缩畸形等。骨搬移首先是通过外固定装置给予骨骼确切的稳定性,取骨缺损上下端的一段活骨,利用外固定架上的可移动装置,按照既定的方向和频率、合适的速度牵伸截取的活骨,重新激发骨组织的再生潜能,逐渐填补骨缺损,完成肢体的重建与修复[6-7]。 Ilizarov骨搬移技术的基本原理是应用张力-应力法则(Law of tension-stress,LTS),给生长中的组织缓慢牵伸产生一定的张力,可刺激某些组织的再生和活跃生长,其生长方式同胎儿组织一致,均为相同的细胞分裂,通过对活性组织的牵拉来重新激发骨组织的再生潜能,以最小的软组织损伤来恢复患肢正常的功能,挽救了许多濒临截肢的肢体,为治疗长骨大段骨缺损提供了一种全新的治疗方法。骨搬移手术操作步骤简单,手术时间短、安全性高,另外外固定装置组合方便,力学稳定性稳定可靠,有助于搬移骨按照既定的方向牵张,搬移到预期的部位。骨搬移技术在修补长骨大段骨缺损的同时,也可同期延长局部软组织,可最大程度的恢复患肢的功能。目前已成为治疗长骨骨缺损最具潜力的手段之一。与传统的骨缺损治疗手段相比,骨搬移技术可同时修复骨与软组织缺损,明显减少了手术次数,能够提高临床治疗效果,改善了患者的生活质量[8]。 Ilizarov骨搬移技术虽然可成功填补长骨骨缺损,挽救了许多濒临截肢的肢体,但在骨搬移过程中同样存在较为棘手的问题,如对接点愈合困难、搬移骨发生偏移、延长骨长度的丢失、钉道感染、松动及折断和长期佩带外固定装置所造成的患肢痛等一系列问题。而对接点的愈合困难是骨搬移治疗骨缺损中最常见的并发症[9],对接点的骨化愈合时间被认为是决定骨搬移治疗周期长短的关键,如何获得对接点的牢固愈合目前亟须解决的问题。 2.2 对接点的概述 对接点源于经典的骨搬移技术治疗骨缺损。在治疗过程中首先应用外固定装置给予患肢骨骼确切的稳定性,取骨缺损上下端的一段活骨,通过外固定架上的可移动装置,按照既定的方向和频率、合适的速度牵伸截取的活骨,逐渐填补骨缺损,当搬移骨与对应骨的残端会聚时,所形成的区域即为对接点[10-14]。对接点的骨化愈合时间被认为是决定骨搬移治疗周期长短的关键。骨搬移技术在治疗骨缺损过程中主要有两种骨形成方式,截骨后牵伸所形成的新生骨区称为“牵拉性骨再生”,搬移骨填补骨缺损达对接点时的骨形成方式称为“引导性再生”或出现“哈尔滨现象”[15]。 对接点因其难愈合而被骨科医师所熟知,但是关于对接点的组织形态学描述的文献报道罕见。查找相关文献后发现Green等[16]在研究人体搬移骨时首先对对接点进行了简单的组织形态学描述,但是缺乏对对接点的显微组织学检查。Giotakis等[11]在研究中发现当搬移骨达对接点时,首先在对接点处形成血肿,后逐渐被纤维软骨组织所替代。对接点骨化愈合的成骨方式主要为软骨内成骨,但对接点处软骨组织升高的趋势却不恒定[12]。对接点的组织形态学检查可直接了解对接点处的骨化愈合过程,但目前仍缺乏对人体对接点处系统的组织学研究。 Ilizarov骨搬移技术治疗长骨大段骨缺损的有效方法,但治疗过程中同样存在对接点不愈合的治疗难点。受限于地域不同、样本量的大小、随访时间的长短以及个体差异,不同学者对对接点不愈合发生率的报道也不同[2-3,17-18,20-22](见表1)。Mora等[17]在应用Ilizarov骨搬移技术治疗长骨骨缺损时,发现对接点不愈合的发生率约10%,而Charalambous等[22-24]则认为对接点的不愈合率约为50%,治疗对接点不愈合的方法主要为清创植骨术。虽然清创植骨术是治疗对接点不愈合的有效方法,但却存在着增加治疗时间和医疗费用等缺点。如何获得对接点的牢固愈合和缩短治疗时间是目前治疗对接点不愈合亟须解决的问题。 2.3 对接点不愈合的原因及预防 对接点的愈合是一个十分复杂的生物学过程,不同于胚胎骨发育及骨折修复过程,目前的生物学机制尚未完全阐明。不同的年龄、是否合并基础疾病、吸烟、患者的依从性和主观能动性等诸多因素对对接点的愈合都有影响。但软组织的嵌入和搬移骨的偏移致使对接点两端骨对合不良,是造成对接点不愈合的最常见原因[25-26]。Magadum等[26]认为没有规范的手术操作、外固定装置安装不当,也是造成对接点不愈合的常见因素。也有学者研究认为截骨的位置和方法、牵张的速度和频率以及搬移骨在软组织袖内无压力的刺激下长距离搬移,致使对接点两端骨发生不同程度的吸收,不能有效的加压,也是造成对接点不愈合的因素[27]。 众所周知最好的治疗是预防。如何促进对接点以更快的速度骨化愈合,预防对接点不愈合等并发症的发生,一些专家学者进行了大量临床实验研究。研究认为定时术后X射线复查可及时观察截骨延长区新生骨痂的生长状况以及搬移骨是否偏于长骨轴线,对纠正搬移骨的偏移具有重要价值。研究证实术者丰富的经验和患者良好的依从性可明显减少骨搬移并发症的发生[19]。Karargyris等[19,28]认为对接点处加压是促进对接点的愈合有效方法。当搬移骨达对接点时,继续以既定的方向和速度向远端牵伸三四天,即对对接点处进行加压,可有效的促进对接点的愈合。有研究联合应用骨搬移和髓内钉技术治疗长骨骨缺损,认为内外结合既可维持患肢的长度和稳定性,减少外固定装置的佩带时间,还可增加临近关节的活动度,避免搬移骨的轴向偏移[4,29-31]。内外结合方法的应用为治疗长骨大段非感染性骨缺损提供了一种新的方法和理念。Somanchi等[28,32-33]应用骨搬移联合封闭负压引流技术(vacuum assisted closure,VAC)治疗慢性骨髓炎所致的骨与软组织缺损,认为封闭负压引流技术既可改善局部血供、减轻局部组织的水肿,还可促进肉芽组织的生长,避免与外界的交叉感染,有效的促进对接点的骨性愈合。Giotakis等[11]认为短缩延长术可有效避免对接点不愈合的发生,感染坏死组织的整段切除可在局部制造一个新鲜的骨折微环境,机体会分泌各种生长因子来启动骨愈合过程。但是一期骨短缩时有时会出现血管危象等棘手问题,应马上恢复肢体长度,待局部组织炎症反应减轻后再行短缩。一些学者建议使用泰勒外固定支架(taylor spatial frame,TSF)行骨搬移技术治疗骨缺损,因为泰勒外固定支架可通过电脑软件设计调整参数,在三维空间准确有效的矫正搬移骨在软组织通道内的偏移,增大对接点两端骨的接触面积,减少对接点不愈合的发 生[9]。 2.4 对接点不愈合的治疗 随着Ilizarov骨搬移技术治疗长骨大段骨缺损的广泛应用,对骨搬移并发症对接点不愈合的处理也变得熟悉起来。积极主动的治疗对接点不愈合,可缩短治疗时间,减轻患者的痛苦。目前治疗对接点不愈合的方法有生物物理治疗、保守治疗和手术治疗。见图1。 2.4.1 生物物理治疗 生物物理学方法均为非侵入性治疗,使用方便,并发症少,治疗费用低廉且无手术并发症,临床应用亦较为广泛。其主要有高压氧、电磁刺激、振动冲击波治疗等。 2.4.2 保守治疗 对接点不愈合的保守治疗操作简便、创伤小,是治疗对接点难愈合的有效方法。加压法是治疗对接点不愈合的最常用的方法,即按照既定的方向以每周2次,每次0.25 mm,连续3个月的方法将对接点处加压[2、11、34]。柴明祥等[35]认为物理加压和部分负重生理"
| [1] DeCoster TA,Gehlert RJ, Mikola EA, et al. Management of posttraumatic segmental bone defects.J Am AcadOrthop Surg.2004;12(1):28-38.[2] Maini L, Chadha M, Vishwanath J, etal.TheIlizarov method in infected nonunion of fractures.Injury.2000;31(7):509-517.[3] Krishnan A, Pamecha C, Patwa JJ.Modified Ilizarov technique for infectedno- nunion of the femur: the principle of distraction-compression osteogenesis.J OrthopSurg (Hong Kong).2006;14(3):265-272.[4] Lin CC, Chen CM, Chiu FY,et al. Staged protocol for the treatment of chronic tibial shaft osteomyelitis with Ilizarov's technique followed by the application of intramedullary locked nail. Orthopedics.2012;35(12):e1769-1774.[5] Thirumal M, Shong HK. Bone transport in the management of fractures of the tibia. Med J Malaysia. 2001;56(1):44-52.[6] 秦泗河.读《骨搬移治疗骨缺损与骨不连》有感[J].中国矫形外科杂志2009,17(24):1919-1920.[7] 秦泗河,孙磊.Ilizarov技术在矫形外科的应用进展[J].中国矫形外科杂志,2002,9(3):295-298.[8] Yin P, Ji Q, Li T, et al. A systematic review and meta-analysis of Ilizarov methods in the treatment of infected nonunion of tibia and femur. PloS one.2015;10(11): e0141973.[9] Robinson PM, Papanna M, Younis F,et al. Arthroscopic debridement of docking site in Ilizarov bone transport. Ann R CollSurg Engl.2010;92(5):437-438.[10] Peng J, Min L, Xiang Z, et al.Ilizarov bone transportcombined with antibiotic cement spacer for infected tibial nonunion.Int J ClinExp Med. 2015;8(6):10058-10065. [11] Giotakis N, Narayan B, Nayagam S.Distraction osteogenesis and nonunion of the docking site: is there an ideal treatment option? Injury. 2007;38 Suppl1:S100-107.[12] Garcia FL, Picado CH, Garcia SB. Histology of the regenerate and docking site in bone transport. Arch Orthop Trauma Surg.2009;129(4):549-558.[13] Tresley J, Schoenleber SJ, Singer AD, et al. "Ilizarov" external fixation: what the radiologist needs to know. Skeletal Radiol. 2015;44(2):179-195.[14] DeCoster TA, Simpson AH, Wood M. Biologic model of bone transport distraction osteogenesis and vascular response. J Orthop Res. 1999;17(2):238-45.[15] 曲龙,施京辉,刘黎亮,等.骨搬移法治疗骨感染、骨缺损及软组织缺损[J].中华外科杂志,2004,42(23):1469.[16] Green SA, Jackson JM, Wall DM, et al. Management of segmental defects by the Ilizarov intercalary bone transport method.ClinOrthopRelat Res. 1992;(280): 136-142.[17] Mora R, Maccabruni A, Bertani B, etal. Revision of 120 tibial infected non-unions with bone and soft tissue loss treated with epidermato-fascialosteoplasty according to Umiarov.Injury. 2014;45(2):383-387.[18] Bumbasirevi? M, Tomi? S, Lesi? A, et al. War-related infected tibial nonunion with bone and soft-tissue loss treated with bone transport using the Ilizarov method. Arch Orthop Trauma Surg.2010;130(6):739-749.[19] Abdel-Aal AM.Ilizarov bone transport for massive tibial bone defects. Orthopedics. 2006;29(1):70-74.[20] Erler K, Yildiz C, Baykal B, et al.Reconstruction of defects following bone tumor resections by distraction osteogenesis. Arch Orthop Trauma Surg. 2005;125(3):177-183. [21] Song HR, Cho SH, Koo KH, et al.Tibial bone defects treated by internal bone transport using the Ilizarov method. Int Orthop.1998;22(5):293-297.[22] Charalambous CP, Wilkes RA. Bone grafting of the un-united docking site in bone transport: description of a percutaneous approach.Ann R CollSurg Engl.2008;90(7):613.[23] Marsh DR, Shah S, Elliott J, et al. The Ilizarov method in nonunion, malunion and infection of fractures. J Bone Joint Surg Br. 1997;79(2):273-279.[24] Tokizaki T, Abe S, Tateishi A, et al. Distraction osteogenesis for knee arthrodesis in infected tumor prostheses. Clin Orthop Relat Res. 2004;(424):166-172.[25] Lowenberg DW, Feibel RJ, Louie KW, et al. Combined muscle flap and Ilizarov reconstruction for bone and soft tissue defects. Clin Orthop Relat Res. 1996;(332):37-51.[26] Magadum MP,BasavarajYadav CM,Phaneesha MS,et al. Acute compression and lengthening by the Ilizarov technique for infected nonunion of the tibia with large bone defects. J Orthop Surg (Hong Kong). 2006;14(3):273-279.[27] Tsuchiya H, Sakurakichi K, Yamashiro T. Bone transport with frozen devitalized bone: an experimental study using rabbits and a clinical application. J Orthop Sci. 2004;9(6):619-24.[28] Karargyris O, Polyzois VD, Karabinas P, et al.Papineau debridement, Ilizarov bone transport, and negative-pressure wound closure for septic bone defects of the tibia. Eur J Orthop SurgTraumatol.2014;24(6):1013-1017.[29] Paley D, Catagni MA, Argnani F, et al. Ilizarov treatment of tibial nonunions withbone loss. Clin Orthop Relat Res. 1989; (241):146-165.[30] 徐永清,朱跃良,范新宇,等.二处截骨骨搬运治疗胫骨干大段感染性骨缺损合并软组织缺损的再认识[J].中华创伤骨科杂志,2015, 17(10):850-853.[31] Gulabi D,Erdem M,Cecen GS,et al.Ilizarov fixator combined with an intramedullary nail for tibialnonunions with bone loss: is it effective? Clin Orthop RelatRes.2014;472(12):3892-3901.[32] Somanchi BV, Khan S. Vacuum-assisted wound closure (VAC) with simultaneous bone transport in the leg: a technical note. Acta Orthop Belg. 2008;74(4):538-541.[33] Stannard JP, Robinson JT, Anderson ER. Negative pressure wound therapy to treat hematomas and surgical incisions following high-energy trauma. J Trauma. 2006;60(6): 1301-1306.[34] Lovisetti G, Sala F, Miller AN, et al. Clinical reliability of closed techniques and comparison with open strategies to achieve union at the docking site. Int Orthop. 2012;36(4):817-825.[35] 柴明祥,臧建成,吴天昊,等.胫骨骨搬运后对合端不愈合的原因与治疗[J].中华创伤骨科杂志,2013,15(10):840-844.[36] Hatzokos I, Stavridis SI, Iosifidou E, et al.Autologous bone marrow grafting combined with demineralized bone matrix improves consolidation of docking site after distraction osteogenesis. J Bone Joint Surg Am. 2011;93(7):671-678.[37] Moghaddam MH, Vahedi E.Effect of decortications on union rate of tibial plating.Orthopedics. 2015;38(3):e213-216.[38] Tall M, Bonkoungou D, Sawadogo M, et al.Bone and Joint Trauma Study Group (GETRAUM). Treatment of nonunion in neglected long bone shaft fractures by osteoperiosteal decortication. OrthopTraumatolSurg Res.2014;100(6 Suppl): S299-303.[39] 陶大为,王志刚,张 锴.骨皮质剥脱与其他固定方式联用修复骨不连:是否需植骨及内置物的处理[J].中国组织工程研究, 2015, 19(31):5079-5084.[40] Kucukkaya M, Kabukcuoglu Y, Tezer M, et al. Management of childhood chronic tibial osteomyelitis with the Ilizarov method. J Pediatr Orthop. 2002;22(5):632-637.[41] Cattaneo R, Catagni M, Johnson EE. The treatment of infected nonunions and segmental defects of the tibia by the methods of Ilizarov. Clin Orthop Relat Res. 1992;(280): 143-152.[42] Lovisetti G, Sala F. Clinical strategies at the docking site of distraction osteogenesis: are open procedures superior to the simple compression of Ilizarov? Injury. 2013;44Suppl 1: S58-62. [43] Yin P, Zhang L, Zhang L, et al. Ilizarov bone transport for the treatment of fibular osteomyelitis: a report of five cases. BMC Musculoskelet Disord. 2015;16:242.[44] El-Mowafi H, Elalfi B, Wasfi K. Functional outcome following treatment of segmental skeletal defects of the forearm bones by Ilizarov application. Acta Orthop Belg. 2005;71(2):157-162. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [3] | Yang Weiqiang, Ding Tong, Yang Weike, Jiang Zhengang. Combined variable stress plate internal fixation affects changes of bone histiocyte function and bone mineral density at the fractured end of goat femur [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 890-894. |
| [4] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [5] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [6] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [7] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [8] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [9] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [10] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [11] | Cheng Shigao, , Wang Wanchun, Jiang Dong, Li Tengfei, Li Xun, Ren Lian. Comparison of the standard and long-stem bone cement prosthesis replacement in the treatment of intertrochanteric fractures in elderly patients [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 362-367. |
| [12] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [13] | Zeng Xianghong, Liang Bowei. A new strategy for the treatment of osteonecrosis of the femoral head [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 431-437. |
| [14] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [15] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||