Chinese Journal of Tissue Engineering Research ›› 2026, Vol. 30 ›› Issue (28): 7494-7504.doi: 10.12307/2026.831
A systematic review and network meta-analysis of neuromodulation techniques for promoting upper limb motor function after stroke
Fan Mengmeng, Ding Jiali, Wan Yujie, Huang Hailiang
- Rehabilitation Medicine School of Shandong University of Traditional Chinese Medicine, Jinan 250355, Shandong Province, China
-
Received:2025-10-29Revised:2025-12-29Online:2026-10-08Published:2026-02-27 -
Contact:Huang Hailiang, MD, Professor, Rehabilitation Medicine School of Shandong University of Traditional Chinese Medicine, Jinan 250355, Shandong Province, China -
About author:Fan Mengmeng, MS candidate, Rehabilitation Medicine School of Shandong University of Traditional Chinese Medicine, Jinan 250355, Shandong Province, China -
Supported by:Construction Project of Liu Zhaochun Inheritance Studio for Famous Traditional Chinese Medicine in Shandong Province, No. [2018]1 (to HHL)
CLC Number:
Cite this article
Fan Mengmeng, Ding Jiali, Wan Yujie, Huang Hailiang. A systematic review and network meta-analysis of neuromodulation techniques for promoting upper limb motor function after stroke[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(28): 7494-7504.
share this article
Add to citation manager EndNote|Reference Manager|ProCite|BibTeX|RefWorks
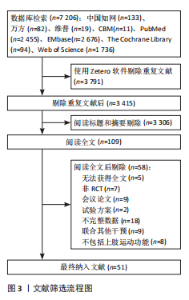
2.1 检索结果 各数据库初步检索共得到6 823篇文献,经Zetero软件剔除重复文献3 408篇,阅读标题摘要剔除3 306篇,通过纳入和排除标准,最终纳入文献51篇,见图3。"
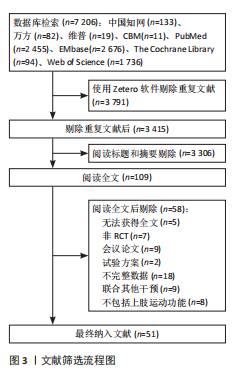

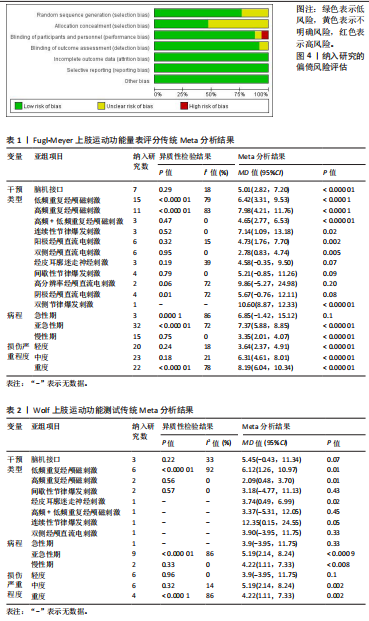
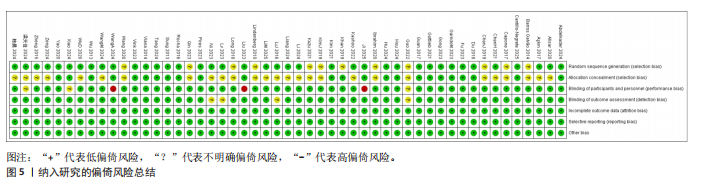
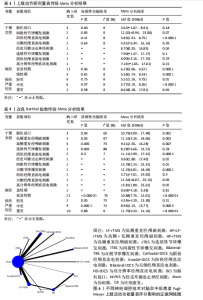
2.2 纳入文献的基本信息 共纳入51篇文献,涉及2 614例脑卒中患者,其中对照组1 180例,试验组1 434例。其中共纳入12种神经调控技术,包括脑机接口7篇[23-29],taVNS 3篇[30-32],低频重复经颅磁刺激(Low-Frequency Repetitive Transcranial Magnetic Stimulation,LF-rTMS) 16篇[33-48],高频+低频重复经颅磁刺激(High-Frequency + Low-Frequency Repetitive Transcranial Magnetic Stimulation, HF+LF-rTMS) 3篇[35,42,49],高频重复经颅磁刺激(High-Frequency Repetitive Transcranial Magnetic Stimulation,HF-rTMS) 11篇[34-39,49-53],连续性节律爆发刺激(Continuous Theta-Burst Stimulation,cTBS) 3篇[47,54-55],间歇性节律爆发刺激(Intermittent Theta-Burst Stimulation,iTBS ) 4篇[33,55-57],双侧节律爆发刺激(Bilateral Theta- Burst Stimulation,Bilateral-TBS) 1篇[58],阴极经颅直流电刺激(Cathodal Transcranial Direct Current Stimulation,Cathodal-tDCS)4篇[59-62],阳极经颅直流电刺激(Anodal Transcranial Direct Current Stimulation,Anodal-tDCS )6篇[59-60,63-66], 双侧经颅直流电刺激(Bilateral Transcranial Direct Current Stimulation,Bilateral-tDCS )6篇[67-72],高分辨率经颅直流电刺激(High-Definition Transcranial Direct Current Stimulation,HD-tDCS) 2篇[63,73]。文献基本信息见附表1。 2.3 文献质量评价 在纳入的51项研究中均报道采用随机分组[23-73],但其中有12项未说明具体的实施方法为不明确风险[28,31,34,38,42-43,46-47,53,57-58,67]。共有24项研究明确采取了不透明信封、加密邮件或储物柜等方式进行分配隐藏为低风险[23-27,33,35,37,44,50,52,54-55,58-62,65-66,69-71,73],其余研究未见相关描述。共有45项试验的研究人员或受试者在分组分配上实施盲法[24,26,30-49,51-73],在47项研究中,结果测量者实施盲法[23-27,29-35,37-44,46-48,50-73]。所纳入的研究数据均完整,没有选择性报告结果或其他偏倚风险。对纳入研究的偏倚风险评估见图4,5。 2.4 Meta分析结果 2.4.1 Fugl-Meyer上肢运动功能评定 纳入的50篇研究结局指标涉及2 502例脑卒中患者[23-39,41-73],其中试验组1 376例,对照组1 126例。异质性检验结果提示研究间差异较大(I2=73%,P < 0.000 01),还因纳入研究中神经调控技术类型差异显著,且患者病程跨度大,采用随机效应模型进行分析。合并效应量显示,神经调控干预在改善患者上肢运动功能方面较常规治疗具有显著优势(MD=6.22,95%CI:4.88-7.54,P < 0.000 01)。为探究异质性来源,依据干预类型、病程、损伤严重程度进行亚组分析,部分亚组的异质性显著降低,提示可能是异质性的重要影响因素。传统Meta分析结果显示干预措施方面脑机接口、低频重复经颅磁刺激、高频重复经颅磁刺激、高频+低频重复经颅磁刺激、连续性节律爆发刺激、阳极经颅直流电刺激、双侧经颅直流电刺激及双侧节律爆发刺激在提升评分改善患者上肢运动功能方面均显著优于常规康复治疗;病程方面,亚急性期与慢性期评分均优于对照组,亚急性期效果最佳;损伤严重程度方面,各程度评分高于对照组,重度损伤患者治疗效果最佳,见表1。 2.4.2 Wolf上肢运动功能测试 纳入的12篇研究结局指标涉及Wolf上肢运动功能测试[23,27-28,32-33,35-36,40,45,48,55,70]。其中试验组526例,对照组415例。异质性检验结果提示研究间差异较大(I2=83%,P < 0.000 01),采用随机效应模型进行分析。合并效应量显示,神经调控干预在改善患者上肢运动功能方面较常规治疗具有显著优势(MD=5.15,95%CI:2.52-7.78,P=0.000 1)。为探究异质性来源,依据干预类型、病程、损伤严重程度进行亚组分析,部分亚组的异质性显著降低,提示以上可能是异质性的重要影响因素。传统Meta分析结果显示低频重复经颅磁刺激与高频重复经颅磁刺激在提升Wolf上肢运动功能测试评分方面均显著优于常规康复治疗;病程方面,亚急性期与慢性期评分均优于对照组,亚急性期效果最佳;损伤严重程度方面,中度与重度损伤患者评分高于对照组,中度损伤患者治疗效果最佳,见表2。"
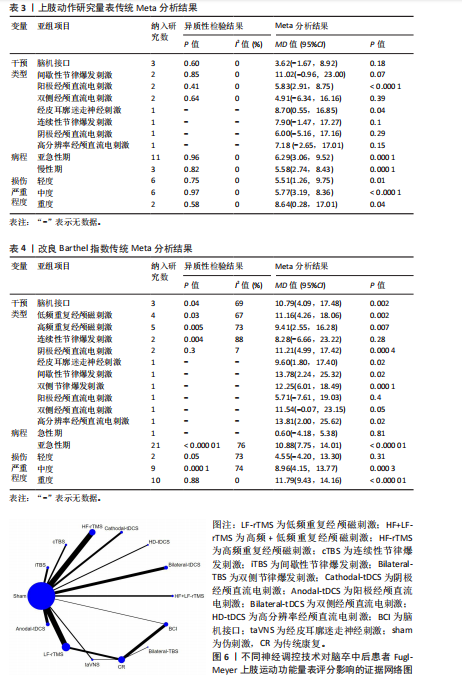
"
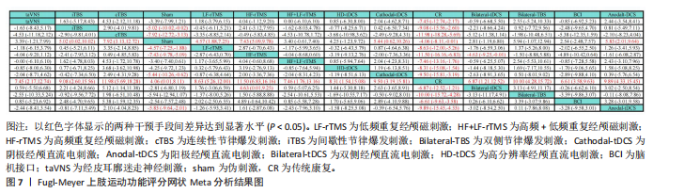
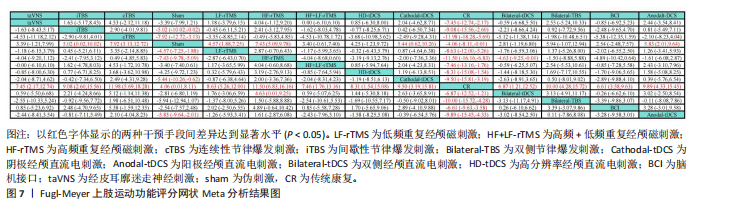
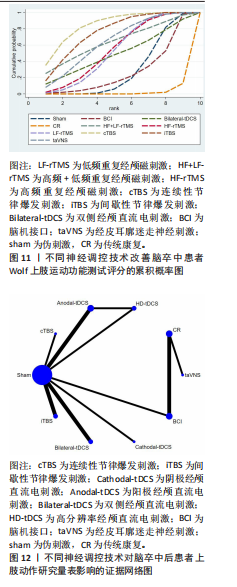
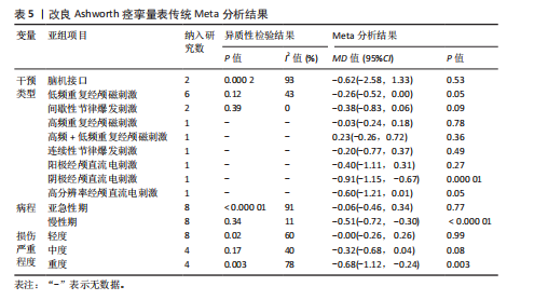
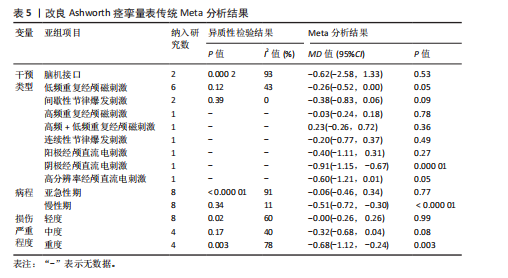
2.4.3 上肢动作研究量表 纳入的12篇研究结局指标涉及764例脑卒中患者[23-25,30。54,56-57,62-64,71-72],均采用上肢动作研究量表进行上肢运动功能评定。其中试验组394例,对照组370例。异质性检验结果提示研究间差异小(I2=0%,P=0.98),采用固定效应模型进行分析。合并效应量显示,神经调控干预在改善患者上肢运动功能方面较常规治疗具有显著优势(MD=5.98,95%CI:3.81-8.15,P < 0.000 01)。 尽管总体异质性较低,此次研究仍进行了亚组分析,以进一步探索不同干预方式、病程、损伤严重程度下的效果差异。传统Meta分析结果显示阳极经颅直流电刺激在提升上肢动作研究量表评分改善患者上肢运动功能方面均显著优于常规康复治疗;病程、损伤严重程度方面,亚急性期与重度损伤患者治疗效果最佳,见表3。 2.4.4 改良Barthel指数 纳入的18篇研究结局指标涉及改良Barthel指数[25,27,29-30,34,39-40,46,50-52,54-55,58,61-63,72]。其中试验组543例,对照组454例。异质性检验结果提示研究间差异较大(I2=76%,P < 0.000 01),采用随机效应模型进行分析。合并效应量显示,神经调控干预在改善患者上肢运动功能方面较常规治疗具有显著优势(MD=10.25,95%CI:7.26-13.25,P=0.000 1)。为探究异质性来源,依据干预类型进行亚组分析,显示异质性仍较高,因此仅对结果进行描述性分析。传统Meta分析结果显示脑机接口、低频重复经颅磁刺激、高频重复经颅磁刺激及阴极经颅直流电刺激在提升改良Barthel指数评分方面均显著优于常规康复治疗,病程、损伤严重程度方面,亚急性期与重度损伤患者治疗效果最佳,见表4。 2.4.5 改良Ashworth痉挛量表 纳入的13篇研究结局指标涉及改良Ashworth痉挛量表[23,28,35,41,43-44,46-47,56-57,61,66,73]。其中试验组365例,对照组317例。异质性检验结果提示研究间差异较大(I2=83%,P < 0.000 01),采用随机效应模型进行分析。合并效应量显示,神经调控干预在改善患者上肢运动功能方面较常规治疗具有显著优势(MD=-0.31,95%CI:-0.57至-0.04,P=0.02)。为探究异质性来源,依据干预类型进行亚组分析,部分亚组的异质性显著降低,提示干预类型差异可能是异质性的重要影响因素,但传统Meta分析结果显示各单项技术未见显著优势,病程、损伤严重程度方面,亚急性期与重度损伤患者治疗效果最佳,见表5。 2.5 网状Meta分析结果 2.5.1 Fugl-Meyer上肢运动功能评定 该结局指标共纳入50项研究[23-39,41-73],涉及12种神经调控技术,包括脑机接口、低频重复经颅磁刺激、高频重复经颅磁刺激、高频+低频重复经颅磁刺激、连续性节律爆发刺激、间歇性节律爆发刺激、双侧节律爆发刺激、阳极经颅直流电刺激、阴极经颅直流电刺激、双侧经颅直流电刺激、高分辨率经颅直流电刺激、经皮耳廓迷走神经刺激。其上肢运动功能评定证据网络,见图6。在网络一致性检验中,节点分析结果显示P=0.904,提示模型整体一致性较为理想。局部一致性通过节点劈裂法进行检验,发现各比较P值均> 0.05,表明未见显著局部不一致性,直接与间接证据保持较高一致性,故采用一致性模型完成后续分析。网状Meta分析结果显示,脑机接口、低频重复经颅磁刺激、高频重复经颅磁刺激、高频+低频重复经颅磁刺激、连续性节律爆发刺激、间歇性节律爆发刺激、双侧节律爆发刺激、阳极经颅直流电刺激、阴极经颅直流电刺激、双侧经颅直流电刺激、高分辨率经颅直流电刺激、经皮耳廓迷走神经刺激对上肢运动功能的改善效果显著优于传统疗法。12种神经调控技术之间,高频重复经颅磁刺激对上肢运动功能的改善效果显著优于双侧经颅直流电刺激,而其他神经调控技术之间对上肢运动功能的改善效果两两比较差异均无显著性意义(P > 0.05),见图7。针对12种干预方式对上肢运动障碍的改善效果进行比较排序,其最优概率依次为:高频重复经颅磁刺激(85.1%) > 连续性节律爆发刺激(84.1%) > 阳极经颅直流电刺激(67.7%) > 双侧节律爆发刺激(66.0%) > 阴极经颅直流电刺激(63.7%) > 间歇性节律爆发刺激(58.6%) > 低频重复经颅磁刺激(54.5%) > 高分辨率经颅直流电刺激(51.3%) > 高频+低频重复经颅磁刺激(43.0%) > 经皮耳廓迷走神经刺激(42.5%) > 双侧经颅直流电刺激(36.8%) > 脑机接口(34.4%),见图8。 2.5.2 Wolf上肢运动功能测试 该结局指标共纳入12项研究[23,27-28,32-33,35-36,40,45,48,55,70],涉及8种神经调控技术,包括脑机接口、低频重复经颅磁刺激、高频重复经颅磁刺激、高频+低频重复经颅磁刺激、连续性节律爆发刺激、间歇性节律爆发刺激、双侧经颅直流电刺激、经皮耳廓迷走神经刺激。其评定证据网络,见图9。在网络一致性检验中,节点分析结果显示P=0.933,提示模型整体一致性较为理想。局部一致性通过节点劈裂法进行检验,发现各比较P值均> 0.05,表明未见显著局部不一致"
"

"
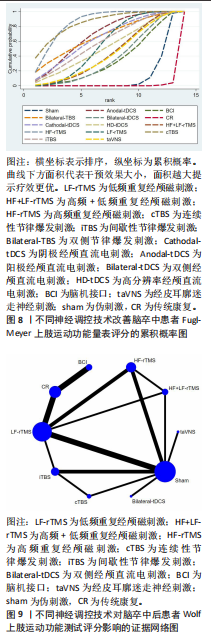
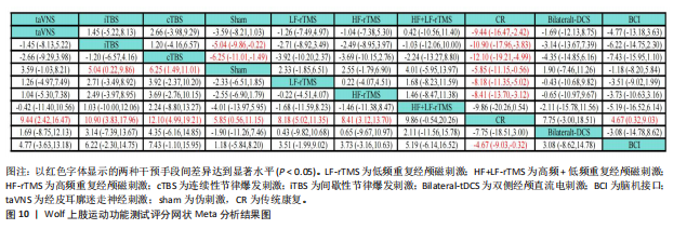
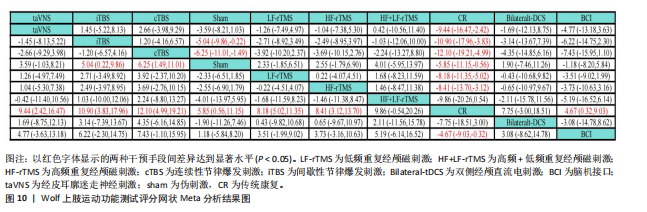
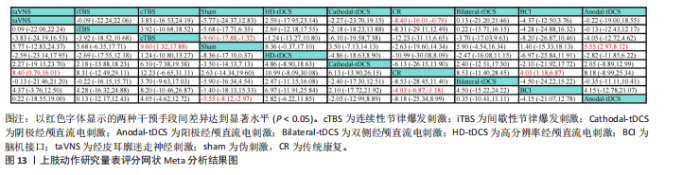
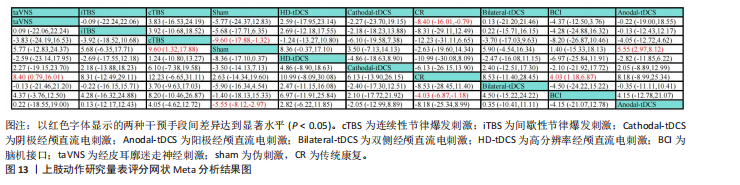
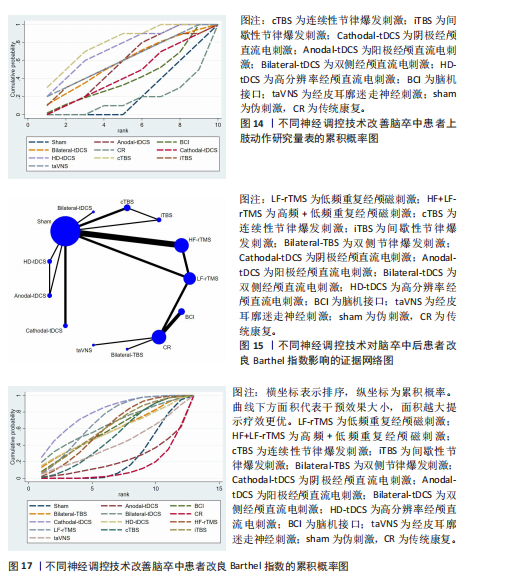
性,直接与间接证据保持较高一致性,故采用一致性模型完成后续分析。网状Meta分析结果显示,脑机接口、低频重复经颅磁刺激、高频重复经颅磁刺激、连续性节律爆发刺激、间歇性节律爆发刺激、经皮耳廓迷走神经刺激对上肢运动功能的改善效果显著优于传统疗法。8种神经调控技术之间对上肢运动功能的改善效果两两比较差异均无显著性意义(P > 0.05),见图10。针对8种干预方式对上肢运动障碍的改善效果进行比较排序,其最优概率依次为:连续性节律爆发刺激(84.6%) > 间歇性节律爆发刺激(75.4%) > 高频+低频重复经颅磁刺激(63.9%) > 经皮耳廓迷走神经刺激(63.8%) > 高频重复经颅磁刺激(54.2%) > 低频重复经颅磁刺激(52.8%) > 双侧经颅直流电刺激(49.2%) > 脑机接口(26.3%),见图11。 2.5.3 上肢动作研究量表 该结局指标共纳入12项研究[23-25,30,54,56-57,62-64,71-72],涉及8种神经调控技术,包括脑机接口、连续性节律爆发刺激、间歇性节律爆发刺激、阳极经颅直流电刺激、阴极经颅直流电刺激、双侧经颅直流电刺激、高分辨率经颅直流电刺激、经皮耳廓迷走神经刺激。其上肢运动功能恢复情况证据网络,见图12。在上肢动作研究量表的网络一致性检验中,节点分析结果显示P=0.552,提示模型整体一致性较为理想。局部一致性通过节点劈裂法进行检验,发现各比较P值均大于0.05,表明未见显著局部不一致性,直接与间接证据保持较高一致性,故采用一致性模型完成后续分析。网状Meta分析结果显示,脑机接口、经皮耳廓迷走神经刺激对上肢运动功能恢复效果显著优于传统疗法。阳极经颅直流电刺激、连续性节律爆发刺激对上肢运动功能的改善效果显著优于伪刺激组。8种神经调控技术之间对上肢运动功能的改善效果两两比较差异均无显著性意义(P > 0.05),见图13。针对8种干预方式对上肢运动障碍的改善效果进行比较排序,其最优概率依次为:连续性节律爆发刺激(77.5%) > 高分辨率经颅直流电刺激(71.0%) > 经皮耳廓迷走神经刺激(60.4%) > 双侧经颅直流电刺激(57.1%) > 阳极经颅直流电刺激(56.2%)=间歇性节律爆发刺激(56.2%) > 阴极经颅直流电刺激(43.9%) > 脑机接口(39.5%),见图14。"

"
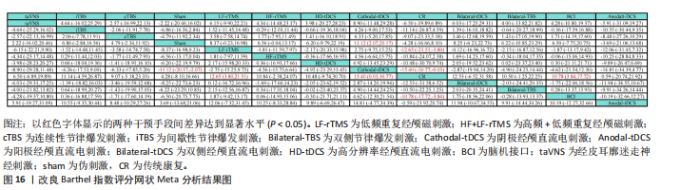
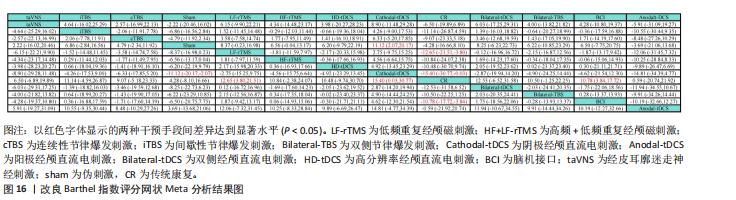
2.5.4 改良Barthel指数 该结局指标共纳入18项研究[25,27,29-30,34,39-40,46,50-52,54-55,58,61-63,72], 涉及11种神经调控技术,包括脑机接口、低"

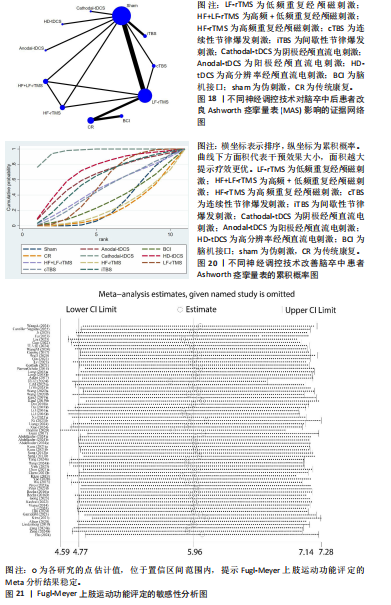
频重复经颅磁刺激、高频重复经颅磁刺激、连续性节律爆发刺激、间歇性节律爆发刺激、双侧节律爆发刺激、阳极经颅直流电刺激、阴极经颅直流电刺激、双侧经颅直流电刺激、高分辨率经颅直流电刺激、经皮耳廓迷走神经刺激。其日常生活活动证据网络,见图15。在改良Barthel指数的网络一致性检验中,节点分析结果显示P=0.491,提示模型整体一致性较为理想。局部一致性通过节点劈裂法进行检验,发现各比较P值均> 0.05,表明未见显著局部不一致性,直接与间接证据保持较高一致性,故采用一致性模型完成后续分析。网状Meta分析结果显示,脑机接口、低频重复经颅磁刺激、阴极经颅直流电刺激对日常生活活动改善效果显著优于传统疗法。11种神经调控技术之间对上肢运动功能的改善效果两两比较差异均无显著性意义(P > 0.05),见图16。针对12种干预方式对上肢运动障碍的改善效果进行比较排序,其最优概率依次为:阴极经颅直流电刺激(78.8%) > 低频重复经颅磁刺激(68.8%) > 双侧经颅直流电刺激(64.1%) > 间歇性节律爆发刺激(60.0%) > 高频重复经颅磁刺激(59.5%) > 脑机接口(58.7%) > 双侧节律爆发刺激(56.5%)=高分辨率经颅直流电刺激(56.5%) > 连续性节律爆发刺激(49.4%) > 经皮耳廓迷走神经刺激(41.1%) > 阳极经颅直流电刺激(21.0%),见图17。 2.5.5 改良Ashworth痉挛量表 该结局指标共纳入13项研究[23,28,35,41,43-44,46-47,56-57,61,66,73],涉及9种神经调控技术,包括脑机接口、低频重复经颅磁刺激、高频重复经颅磁刺激、高频+低频重复经颅磁刺激、连续性节律爆发刺激、间歇性节律爆发刺激、阳极经颅直流电刺激、阴极经颅直流电刺激、高分辨率经颅直流电刺激。其改良Ashworth痉挛量表证据网络,见图18。在网络一致性检验中,节点分析结果显示"
"

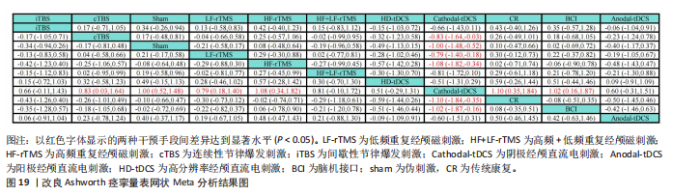
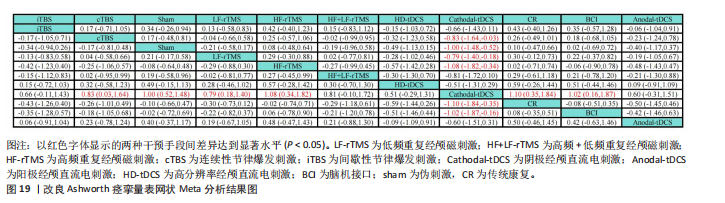
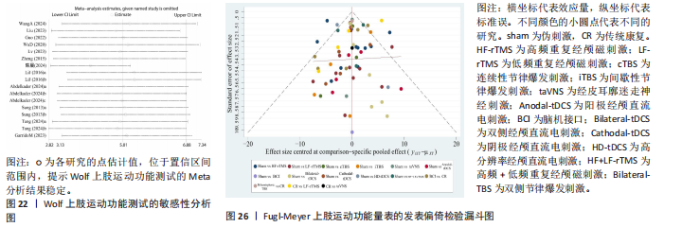
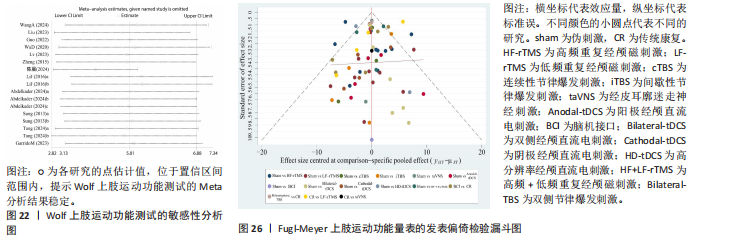
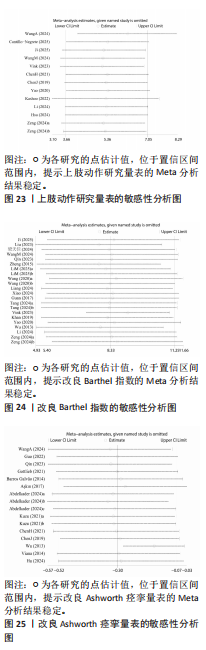
P=0.657,提示模型整体一致性较为理想。局部一致性通过节点劈裂法进行检验,发现各比较P值均 > 0.05,表明未见显著局部不一致性,直接与间接证据保持较高一致性,故采用一致性模型完成后续分析。网状Meta分析结果显示,阴极经颅直流电刺激对上肢运动功能的改善效果显著优于传统疗法与假刺激。9种神经调控技术之间,阴极经颅直流电刺激对上肢运动功能的改善效果显著优于连续性节律爆发刺激、低频重复经颅磁刺激、高频重复经颅磁刺激、脑机接口,而其他神经调控技术之间对上肢痉挛的改善效果两两比较差异均无显著性意义(P > 0.05),见图19。针对9种干预方式对上肢运动障碍的改善效果进行比较排序,其最优概率依次为:阴极经颅直流电刺激(96.7%) > 高分辨率经颅直流电刺激(772.1%) > 阳极经颅直流电刺激(63.6%) > 间歇性节律爆发刺激(61.3%) > 低频重复经颅磁刺激(53.7%) > 高频+低频重复经颅磁刺激(48.9%) > 连续性节律爆发刺激(47.0%) > 脑机接口(31.5%) > 高频重复经颅磁刺激(24.8%),见图20。 2.5.6 敏感性分析结果 对 Fugl-Meyer上肢运动功能评定、Wolf上肢运动功能测试、上肢动作研究量表、改良Barthel指数和改良Ashworth痉挛量表进行了敏感性分析。采用逐一排除单项研究的方法,评估剔除后的异质性变化。结果显示,剔除任一研究均未对5个结局指标的异质性产生显著影响,提示分析结果稳健,见图21-25。 2.6 发表偏倚结果 鉴于次要结局研究数量不足以支撑可靠的统计学检验,此次研究仅对主要结局指标 Fugl-Meyer上肢运动功能评定进行了发表偏倚分析。Begg’s检验(P=0.941)和 Egger’s检验(P=0.789)结果均未提示显著差异,漏斗图亦呈基本对称分布,表明该结局指标的发表偏倚风险较低,结果较为稳健,见图26。 2.7 不良反应 共有10篇文献报道了相关不良事件[23,32,36-37,44-55,62,64,70-71]。干预过程中患者主要表现为皮肤发红、患侧手部疼痛、麻木、短暂性头痛、疲劳、瘙痒及轻度刺痛等症状,但均在治疗结束后迅速缓解,提示整体安全性较高。"
"
"

"
"
| [1] CAMPBELL BCV, KHATRI P. Stroke. The Lancet. 2020; 396(10244):129-142. [2] GBD 2016 Stroke Collaborators.Global, regional, and national burden of stroke, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):439-458. [3] O’FLAHERTY D, ALI K. Recommendations for Upper Limb Motor Recovery: An Overview of the UK and European Rehabilitation after Stroke Guidelines (2023). Healthcare (Basel). 2024;12(14):1433. [4] KHAN MA, FARES H, GHAYVAT H, et al. A systematic review on functional electrical stimulation based rehabilitation systems for upper limb post-stroke recovery. Front Neurol. 2023;14:1272992. [5] PSYCHOULI P, MAMAIS I, ANASTASIOU C. An Exploration of the Effectiveness of Different Intensity Protocols of Modified Constraint-Induced Therapy in Stroke: A Systematic Review. Rehabil Res Pract. 2023;2023:6636987. [6] 赵强, 周跃辉, 董泓, 等. 本体感觉神经肌肉促进技术的基础理论、方法及应用[J]. 中国组织工程研究,2026,30(17):4407-4416. [7] 魏达, 马超, 彭玉涛, 等. 神经调控技术在脑卒中康复中的应用进展[J]. 中国现代神经疾病杂志, 2025,25(1):84-91. [8] TAKEUCHI N, IZUMI SI.Noninvasive Brain Stimulation for Motor Recovery after Stroke: Mechanisms and Future Views. Stroke Res Treat. 2012:2012:584727. [9] DAN B. Neuroscience underlying rehabilitation: what is neuroplasticity?. Dev Med Child Neurol. 2019;61(11): 1240-1240. [10] HUANG XL, WU MY, WU CC, et al. Neuromodulation techniques in poststroke motor impairment recovery: Efficacy, challenges, and future directions. Tzu Chi Med J. 2024;36(2):136-141. [11] MA ZZ, WU J J, CAO Z, et al. Motor imagery-based brain–computer interface rehabilitation programs enhance upper extremity performance and cortical activation in stroke patients. J Neuroeng Rehabil. 2024;21(1): 91. [12] ZHANG J, XING Y, DU W, et al. Analysis of the effect of combined rehabilitation training and transcutaneous vagus nerve electrical stimulation on promoting central nervous system remodeling in stroke patients.Brain Res. 2025;1851:149460. [13] SENADHEERA I, HETTIARACHCHI P, HASLAM B, et al. AI Applications in Adult Stroke Recovery and Rehabilitation: A Scoping Review Using AI. Sensors (Basel). 2024;24(20):6585. [14] VINK JJT, VAN LIESHOUT E CC, OTTE WM, et al. Continuous Theta-Burst Stimulation of the Contralesional Primary Motor Cortex for Promotion of Upper Limb Recovery After Stroke: A Randomized Controlled Trial. Stroke. 2023;54(8):1962-1971. [15] AHMED I, MUSTAFAOGLU R, BENKHALIFA N, et al. Does noninvasive brain stimulation combined with other therapies improve upper extremity motor impairment, functional performance, and participation in activities of daily living after stroke? A systematic review and meta-analysis of randomized controlled trial. Top Stroke Rehabil. 2023;30(3):213-234. [16] CHEN S, ZHANG S, YANG W, et al.The effectiveness of intermittent theta burst stimulation for upper limb motor recovery after stroke: a systematic review and meta-analysis of randomized controlled trials. Front Neurosci. 2023;17:1272003. [17] 王海桥, 鲍春龄, 李鹤, 等. 针刺联合运动想象对脑卒中软瘫上肢精细动作的影响[J]. 中国针灸, 2015,35(6):534-538. [18] MASIERO S, CARRARO E. Upper limb movements and cerebral plasticity in post-stroke rehabilitation. Aging Clin Exp Res. 2008;20(2):103-108. [19] YU P, DONG R, WANG X, et al. NeuroImage. Clinical. 2024;43:103636. [20] STERNE JAC, SAVOVIĆ J, PAGE MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ (Clinical research ed.). 2019;366:l4898. [21] WOUDA N C, KNIJFF B, PUNT M, et al. Predicting Recovery of Independent Walking After Stroke: A Systematic Review. Am J Phys Med Rehabil. 2024; 103(5):458-464. [22] ROESNER K, BRODOWSKI H, STRUTZ N. Measuring severe stroke: a scoping review of RCTs. Front Neurol. 2025;16:1631275. [23] WANG A, TIAN X, JIANG D, et al. Rehabilitation with brain-computer interface and upper limb motor function in ischemic stroke: A randomized controlled trial. Med. 2024;5(6):559-569.e4. [24] CANTILLO-NEGRETE J, RODRÍGUEZ-GARCÍA ME, CARRILLO-MORA P, et al. The ReHand-BCI trial: a randomized controlled trial of a brain-computer interface for upper extremity stroke neurorehabilitation. Front Neurosci. 2025;19:1579988. [25] JI X, LU X, XU Y, et al. Effects and neural mechanisms of a brain-computer interface-controlled soft robotic glove on upper limb function in patients with subacute stroke: a randomized controlled fNIRS study.J Neuroeng Rehabil. 2025;22(1): 171. [26] FU J, CHEN S, SHU X, et al. Functional-oriented, portable brain–computer interface training for hand motor recovery after stroke: a randomized controlled study. Front Neurosci. 2023;17:1146146. [27] LIU X, ZHANG W, LI W, et al. Effects of motor imagery based brain-computer interface on upper limb function and attention in stroke patients with hemiplegia: a randomized controlled trial. BMC Neurol. 2023;23(1):136. [28] GUO N, WANG X, DUANMU D, et al. SSVEP-Based Brain Computer Interface Controlled Soft Robotic Glove for Post-Stroke Hand Function Rehabilitation. IEEE Trans Neural Syst Rehabil Eng. 2022;30:1737‐1744. [29] 梁天佳, 龙耀斌, 陆丽燕, 等. 绳带辅助本体感觉神经肌肉促进技术训练联合绳带辅助脑机接口训练对脑卒中偏瘫上肢康复效果的随机对照试验[J]. 中国康复理论与实践,2024,30(8):972-978. [30] WANG MH, WANG YX, XIE M, et al.Transcutaneous auricular vagus nerve stimulation with task-oriented training improves upper extremity function in patients with subacute stroke: a randomized clinical trial. Front Neurosci. 2024;18:1346634. [31] CAPONE F, MICCINILLI S, PELLEGRINO G, et al.Transcutaneous Vagus Nerve Stimulation Combined with Robotic Rehabilitation Improves Upper Limb Function after Stroke. Neural Plast. 2017;2017: 7876507. [32] WU D, MA J, ZHANG L, et al. Effect and Safety of Transcutaneous Auricular Vagus Nerve Stimulation on Recovery of Upper Limb Motor Function in Subacute Ischemic Stroke Patients: A Randomized Pilot Study. Neural Plast. 2020;2020:8841752. [33] SUNG WH, WANG CP, CHOU CL, et al. Efficacy of coupling inhibitory and facilitatory repetitive transcranial magnetic stimulation to enhance motor recovery in hemiplegic stroke patients. Stroke. 2013; 44(5):1375-1382. [34] WANG Q, ZHANG D, ZHAO YY, et al. Effects of high-frequency repetitive transcranial magnetic stimulation over the contralesional motor cortex on motor recovery in severe hemiplegic stroke: A randomized clinical trial. Brain Stimul. 2020;13(4):979-986. [35] ABDELKADER AA, AFIFI LM, MAHER EA, et al. Comparison of Bilateral Versus Unilateral 5 Hz or 1 Hz Repetitive Transcranial Magnetic Stimulation in Subacute Stroke: Assessment of Motor Function in a Randomized Controlled Study. J Clin Neurophysiol. 2024;41(5):478-483. [36] LI J, MENG XM, LI RY, et al. Effects of different frequencies of repetitive transcranial magnetic stimulation on the recovery of upper limb motor dysfunction in patients with subacute cerebral infarction. Neural Regen Res. 2016;11(10):1584-1590. [37] DU J, YANG F, HU J, et al. Effects of high- and low-frequency repetitive transcranial magnetic stimulation on motor recovery in early stroke patients: Evidence from a randomized controlled trial with clinical, neurophysiological and functional imaging assessments. Neuroimage Clin. 2018;21:101620. [38] KIM JS, KIM DH, KIM HJ, et al. Effect of Repetitive Transcranial Magnetic Stimulation in Post-stroke Patients with Severe Upper-Limb Motor Impairment.Brain Neurorehabil. 2019;13(1):e3. [39] LI M, JIA F, LIU P, et al. Effects of Repetitive Transcranial Magnetic Stimulation on Upper Limb Motor Function and Serum Lipid Metabolomics in Patients With Ischemic Stroke: A Randomized Controlled Study. Brain Behav. 2025;15(5):e70558. [40] ZHENG C, LIAO W, XIA W. Effect of combined low-frequency repetitive transcranial magnetic stimulation and virtual reality training on upper limb function in subacute stroke: a double-blind randomized controlled trail.J Huazhong Univ Sci Technolog Med Sci. 2015;35(2):248-254. [41] AŞKIN A, TOSUN A, DEMIRDAL ÜS. Effects of low-frequency repetitive transcranial magnetic stimulation on upper extremity motor recovery and functional outcomes in chronic stroke patients: A randomized controlled trial. Somatosens Mot Res. 2017;34(2): 102-107. [42] LONG H, WANG H, ZHAO C, et al. Effects of combining high- and low-frequency repetitive transcranial magnetic stimulation on upper limb hemiparesis in the early phase of stroke. Restor Neurol Neurosci. 2018;36(1):21-30. [43] BARROS GALVÃO SC, BORBA COSTA DOS SANTOS R, BORBA DOS SANTOS P, et al. Efficacy of coupling repetitive transcranial magnetic stimulation and physical therapy to reduce upper-limb spasticity in patients with stroke: A randomized controlled trial. Arch Phys Med Rehabil. 2014;95(2):222-229. [44] GOTTLIEB A, BOLTZMANN M, SCHMIDT SB, et al. Treatment of upper limb spasticity with inhibitory repetitive transcranial magnetic stimulation: A randomized placebo-controlled trial. NeuroRehabilitation. 2021;49(3):425-434. [45] LV Y, ZHANG JJ, WANG K, et al. Determining the Optimal Stimulation Sessions for TMS-Induced Recovery of Upper Extremity Motor Function Post Stroke: A Randomized Controlled Trial. Brain Sci. 2023; 13(12):1662. [46] QIN Y, LIU X, ZHANG Y, et al. Effects of transcranial combined with peripheral repetitive magnetic stimulation on limb spasticity and resting-state brain activity in stroke patients. Front Hum Neurosci. 2023; 17:992424. [47] KUZU Ö, ADIGUZEL E, KESIKBURUN S, et al. The Effect of Sham Controlled Continuous Theta Burst Stimulation and Low Frequency Repetitive Transcranial Magnetic Stimulation on Upper Extremity Spasticity and Functional Recovery in Chronic Ischemic Stroke Patients.J Stroke Cerebrovasc Dis.2021; 30(7): 105795. [48] 陈晨, 孟兆祥, 杨康, 等. 智能镜像手套任务导向性训练联合低频重复经颅磁刺激对脑卒中患者手功能效果的随机对照试验[J]. 中国康复理论与实践,2024,30(7):831-838. [49] NI J, JIANG W, GONG X, et al. Effect of rTMS intervention on upper limb motor function after stroke: A study based on fNIRS. Front Aging Neurosci. 2023;14:1077218. [50] XIAO J, SUN Y, LIU ZJ, et al. Ipsilesional 5 Hz Repetitive Transcranial Magnetic Stimulation for Motor Dysfunction in Subacute Intracerebral Hemorrhage: An Exploratory Trial. Arch Rehabil Res Clin Transl. 2024;7(1):100386. [51] LIANG S, WANG W, YU F, et al. Repetitive peripheral magnetic stimulation combined with transcranial magnetic stimulation in rehabilitation of upper extremity hemiparesis following stroke: A pilot study. J Rehabil Med. 2024;56:19449. [52] GUAN YZ, LI J, ZHANG XW, et al. Effectiveness of repetitive transcranial magnetic stimulation (rTMS) after acute stroke: A one‐year longitudinal randomized trial. CNS Neurosci Ther. 2017;23(12):940. [53] IBRAHIM EM, ZAKI MA, GABR MGM. Effect of high frequency repetitive transcranial mgnetic stimulation of the contralesional dorsal premotor cortex on recovery from post-stroke severe motor impairment. Eur J Neurology. 2020;27:397-398. [54] VINK JJT, VAN LIESHOUT ECC, OTTE WM, et al. Continuous Theta-Burst Stimulation of the Contralesional Primary Motor Cortex for Promotion of Upper Limb Recovery After Stroke: A Randomized Controlled Trial. Stroke. 2023;54(8):1962-1971. [55] TANG Z, HUANG J, ZHOU Y, et al. Efficacy and Safety of High-Dose TBS on Poststroke Upper Extremity Motor Impairment: A Randomized Controlled Trial. Stroke. 2024;55(9):2212-2220. [56] CHEN YH, CHEN CL, HUANG YZ, et al. Augmented efficacy of intermittent theta burst stimulation on the virtual reality-based cycling training for upper limb function in patients with stroke: a double-blinded, randomized controlled trial. J Neuroeng Rehabil. 2021;18(1):91. [57] CHEN YJ, HUANG YZ, CHEN CY, et al. Intermittent theta burst stimulation enhances upper limb motor function in patients with chronic stroke: a pilot randomized controlled trial.BMC Neurol. 2019;19(1):69. [58] KHAN F, RATHORE C, KATE M, et al. The comparative efficacy of theta burst stimulation or functional electrical stimulation when combined with physical therapy after stroke: a randomized controlled trial.Clin Rehabil. 2019;33(4):693-703. [59] ROCHA S, SILVA E, FOERSTER Á, et al. The impact of transcranial direct current stimulation (tDCS) combined with modified constraint-induced movement therapy (mCIMT) on upper limb function in chronic stroke: a double-blind randomized controlled trial. Disabil Rehabil. 2016;38(7):653-660. [60] PIRES R, BALTAR A, SANCHEZ MP, et al. Do Higher Transcranial Direct Current Stimulation Doses Lead to Greater Gains in Upper Limb Motor Function in Post-Stroke Patients?. Int J Environ Res Public Health. 2023;20(2):1279. [61] WU D, QIAN L, ZOROWITZ RD, et al. Effects on Decreasing Upper-Limb Poststroke Muscle Tone Using Transcranial Direct Current Stimulation: A Randomized Sham-Controlled Study. Arch Phys Med Rehabil. 2013; 94(1):1-8. [62] YAO X, CUI L, WANG J, et al. Effects of transcranial direct current stimulation with virtual reality on upper limb function in patients with ischemic stroke: a randomized controlled trial. J Neuroeng Rehabil. 2020;17:73. [63] ZENG Y, CHENG R, ZHANG L, et al.Clinical Comparison between HD-tDCS and tDCS for Improving Upper Limb Motor Function: A Randomized, Double-Blinded, Sham-Controlled Trial. Neural Plast. 2024;2024: 2512796. [64] KASHOO FZ, AL-BARADIE RS, ALZAHRANI M, et al. Effect of Transcranial Direct Current Stimulation Augmented with Motor Imagery and Upper-Limb Functional Training for Upper-Limb Stroke Rehabilitation: A Prospective Randomized Controlled Trial. Int J Environ Res Public Health. 2022;19(22): 15199. [65] GONG Q, YAN R, CHEN H, et al. Effects of cerebellar transcranial direct current stimulation on rehabilitation of upper limb motor function after stroke. Front Neurol. 2023;14:1044333. [66] VIANA RT, LAURENTINO GEC, SOUZA RJP, et al. Effects of the addition of transcranial direct current stimulation to virtual reality therapy after stroke: A pilot randomized controlled trial. NeuroRehabilitation. 2014;34(3):437-446. [67] LINDENBERG R, RENGA V, ZHU LL, et al. Bihemispheric brain stimulation facilitates motor recovery in chronic stroke patients. Neurology. 2010;75(24):2176-2184. [68] ALISAR DC, OZEN S, SOZAY S. Effects of Bihemispheric Transcranial Direct Current Stimulation on Upper Extremity Function in Stroke Patients: A randomized Double-Blind Sham-Controlled Study. J Stroke Cerebrovasc Dis. 2020;29(1):04454. [69] KIM SH. Effects of Dual Transcranial Direct Current Stimulation and Modified Constraint-Induced Movement Therapy to Improve Upper-Limb Function after Stroke: A Double-Blinded, Pilot Randomized Controlled Trial. J Stroke Cerebrovasc Dis. 2021;30(9): 105928. [70] GARRIDO MM, ÁLVAREZ EE, ACEVEDO PF, et al. Early transcranial direct current stimulation with modified constraint-induced movement therapy for motor and functional upper limb recovery in hospitalized patients with stroke: A randomized, multicentre, double-blind, clinical trial. Brain Stimul. 2023;16(1):40-47. [71] HSU SP, LU CF, LIN BF, et al. Effects of bihemispheric transcranial direct current stimulation on motor recovery in subacute stroke patients: a double-blind, randomized sham-controlled trial. J Neuroeng Rehabil. 2023;20(1):27. [72] LI C, CHEN Y, TU S, et al. Dual-tDCS combined with sensorimotor training promotes upper limb function in subacute stroke patients: A randomized, double-blinded, sham-controlled study. CNS Neurosci Ther. 2024;30(4):e14530. [73] HU C, TI CHE, YUAN K, et al. Effects of high-definition tDCS targeting individual motor hotspot with EMG-driven robotic hand training on upper extremity motor function: a pilot randomized controlled trial. J Neuroeng Rehabil. 2024;21(1):169. [74] WARD NS.Mechanisms underlying recovery of motor function after stroke. Postgrad Med J. 2005; 81(958):510-514. [75] TAUCHI Y, KYOUGOKU M, TAKAHASHI K, et al. Dimensionality and item-difficulty hierarchy of the Fugl-Meyer assessment of the upper extremity among Japanese patients who have experienced stroke.Top Stroke Rehabil. 2022;29(8):579-587. [76] TIAN D, IZUMI SI. Interhemispheric Facilitatory Effect of High-Frequency rTMS: Perspective from Intracortical Facilitation and Inhibition. Brain Sci. 2022;12(8):970. [77] RIZZO V, SIEBNER HR, MODUGNO N, et al. Shaping the excitability of human motor cortex with premotor rTMS. J Physiol. 2004;554(Pt 2):483-495. [78] CORTI M, PATTEN C, TRIGGS W. Repetitive Transcranial Magnetic Stimulation of Motor Cortex after Stroke: A Focused Review. Am J Phys Med Rehabil. 2012;91(3): 254-270. [79] NOWAK DA, GREFKES C, AMELI M, et al. Interhemispheric competition after stroke: brain stimulation to enhance recovery of function of the affected hand. Neurorehabil Neural Repair. 2009; 23(7):641-656. [80] 邵丹丽, 徐雪迪, 高晓平, 等. 基于上肢动作研究量表设计的改良块评价脑卒中患者上肢功能恢复潜能[J].中国组织工程研究,2020,24(35):5682-5687. [81] 吴娱倩, 张玉梅, 孟霞, 等. Wolf运动功能测试量表评定卒中患者偏瘫侧上肢功能的效度和信度研究[J]. 中国卒中杂志,2022,17(3):244-250. [82] 蔡伟强, 李浩正, 朱玉连, 等. 持续短阵脉冲刺激对脑卒中偏瘫患者静息态脑功能连接模式的影响[J]. 中国康复医学杂志,2023,38(7):898-903, 923. [83] DIONÍSIO A, GOUVEIA R, CASTELHANO J, et al. The Role of Continuous Theta Burst TMS in the Neurorehabilitation of Subacute Stroke Patients: A Placebo-Controlled Study. Front Neurol. 2021;12: 749798. [84] CHEN B, YANG T, LIAO Z, et al.Pathophysiology and Management Strategies for Post-Stroke Spasticity: An Update Review. Int J Mol Sci. 2025;26(1):406. [85] KATO N, HASHIDA G,KOBAYASHI M, et al.Characteristics and factors associated with independence in the activities of daily living of patients with amyotrophic lateral sclerosis at diagnosis. J Phys Ther Sci. 2024; 36(11):692-698. [86] HORDACRE B, GOLDSWORTHY MR, VALLENCE AM, et al. Variability in neural excitability and plasticity induction in the human cortex: A brain stimulation study. Brain Stimul. 2017;10(3):588-595. [87] BODDINGTON LJ, REYNOLDS JNJ. Targeting interhemispheric inhibition with neuromodulation to enhance stroke rehabilitation. Brain Stimul. 2017; 10(2):214-222. [88] FARAHANI F, KRONBERG G, FALLAHRAD M, et al. Effects of direct current stimulation on synaptic plasticity in a single neuron. Brain Stimul. 2021;14(3): 588-597. [89] QI F, NITSCHE MA, REN X, et al.Top-down and bottom-up stimulation techniques combined with action observation treatment in stroke rehabilitation: a perspective. Front Neurol. 2023;14:1156987. [90] QI S, CAO L, WANG Q, et al.The Physiological Mechanisms of Transcranial Direct Current Stimulation to Enhance Motor Performance: A Narrative Review. Biology. 2024;13(10):790. [91] DEL FELICE A, DALOLI V, MASIERO S, et al. Contralesional Cathodal versus Dual Transcranial Direct Current Stimulation for Decreasing Upper Limb Spasticity in Chronic Stroke Individuals: A Clinical and Neurophysiological Study. J Stroke Cerebrovasc Dis. 2016;25(12):2932-2941. |
| [1] | Wang Zheng, Cheng Ji, Yu Jinlong, Liu Wenhong, Wang Zhaohong, Zhou Luxing. Progress and future perspectives on the application of hydrogel materials in stroke therapy [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2081-2090. |
| [2] | Gao Feng, Zhang Jun, Yu Wenjun, Chanyu Yujing, Zhao Le, Hu Yuting, Wang Junhua, Liu Yongfu. Effects of wrist-hand orthosis on hand dysfunction in stroke patients: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(8): 2124-2131. |
| [3] | Tao Daiju, Su Haiyu, Wang Yuqi, Shen Zhiqiang, He Bo . Construction and identification of stable PC12 cell lines with high/low expression of miR-122-5p [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(7): 1790-1799. |
| [4] | Cao Xinyan, Yu Zifu, Leng Xiaoxuan, Gao Shiai, Chen Jinhui, Liu Xihua. Effect of repetitive transcranial magnetic stimulation and transcranial direct current stimulation on motor function and gait in children with cerebral palsy: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1539-1548. |
| [5] | Leng Xiaoxuan, Zhao Yuxin, Liu Xihua. Effects of different neuromodulatory stimulation modalities on non-motor symptoms in Parkinson’s patients: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1282-1293. |
| [6] | Yang Zeyu, Zhi Liang, Wang Jia, Zhang Jingyi, Zhang Qingfang, Wang Yulong, Long Jianjun. A visualized analysis of research hotspots in high-frequency repetitive transcranial magnetic stimulation from the macroscopic perspective [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(5): 1320-1330. |
| [7] | Yang Yuanyuan, Zhou Shanshan, Cheng Xiaofei, Feng Luye, Tang Jiqin. Network meta-analysis of non-invasive brain stimulation in the treatment of lower limb motor dysfunction after stroke [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 1008-1018. |
| [8] | Wang Xueting, Yang Wei, Wang Pengqin. Post-stroke rehabilitation robotics: current research status and hot topics in and outside China [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(28): 7404-7409. |
| [9] | Li Sihui, Wang Qin, Cui Shenhong, Cheng Xiaofei, Feng Ziyun, Wang Dehua, Liang Chunting, Leng Jun. A network meta-analysis of effects of non-invasive neuromodulation techniques on language function in patients with aphasia after stroke [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(28): 7485-7493. |
| [10] | Fang Enhui, Guan Hui, Ma Lihong. Non-invasive brain stimulation for core symptoms in children with autism spectrum disorder: a network meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(24): 6373-6381. |
| [11] | Cao Xinyan, Leng Xiaoxuan, Gao Shiai, Chen Jinhui, Liu Xihua. Analysis of influencing factors and risk prediction model for spasticity severity in stroke patients with hemiplegia [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(23): 6092-6098. |
| [12] | Wang Lejun, Chi Wenxin, Song Xiaoqian, Li Qian, Qiao Minjie, Tao Haifeng. Performance of unstable barbell bench press and changes in electromyographic activity after transcranial direct current stimulation [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(23): 6099-6109. |
| [13] | Gao Hongmei, Zhang Kun, Xiao Dongjie, Liu Hua. Human adipose multilineage-differentiating stress-enduring cells on treatment of ischemic stroke in rats [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(19): 4853-4859. |
| [14] | Meng Zhuo, Zhao Renghao, Zhang Anqi, Hua Haotian, Wang Zicheng, Xu Yingtian, Tong Peijian. Literature visualization analysis of brain-computer interface applications in stroke rehabilitation [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(18): 4802-4813. |
| [15] | Lu Anran, Wang Chenyu, Zhang Yan, Huang Huasheng. High-intensity interval training improves the function of exosomes derived from endothelial progenitor cells in spontaneously hypertensive rats [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(18): 4627-4637. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||