Chinese Journal of Tissue Engineering Research ›› 2017, Vol. 21 ›› Issue (11): 1776-1782.doi: 10.3969/j.issn.2095-4344.2017.11.024
Previous Articles Next Articles
Research and progress of high placement technique in total hip arthroplasty
Piao Shang, Du Yin-qiao, Zhou Yong-gang
- Department of Orthopedics, General Hospital of Chinese PLA, Beijing100853, China
-
Online:2017-04-18Published:2017-05-06 -
Contact:Zhou Yong-gang, M.D., Chief physician, Department of Orthopedics, General Hospital of Chinese PLA, Beijing100853, China -
About author:Piao Shang, Studying for master’s degree, Department of Orthopedics, General Hospital of Chinese PLA, Beijing100853, China -
Supported by:the Natural Science Foundation of Beijing, No. 7152139
CLC Number:
Cite this article
Piao Shang, Du Yin-qiao, Zhou Yong-gang. Research and progress of high placement technique in total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2017, 21(11): 1776-1782.
share this article
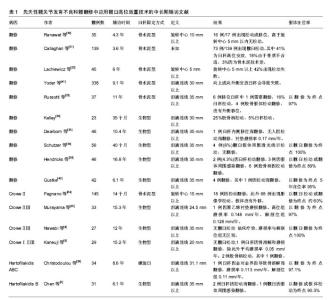
2.1 髋臼高位放置在生物力学上的影响和界面选择 Charnley[1]首次提出髋关节旋转中心的重建位置会引起关节反应力变化。髋臼重建位置改变对于松动率和生存率影响的担忧让某些研究学者做了一些髋臼高位放置的生物力学分析。Johnston等[2]最早设计模型来评估髋臼假体位置变化、颈干角、股骨假体颈长度和大转子位移等对力学改变的影响,研究表明,髋关节在旋转中心位于上、外、后侧时负荷最大。然而没有髋关节中心单纯上移的研究结果。 随后众多体外基础实验和临床实验结果显示,在确保髋臼假体没有外移的情况下,臼杯适当上移放置不会明显增加关节内应力[3-6]。Bicanic等[7]的研究量化了臼杯移位程度与关节反应力,实验显示髋臼假体每外移 1 mm将增加0.7%关节负荷,而臼杯上移1 mm将增加0.1%的关节反应力。主流学界已达成髋臼外移将明显增加关节反应力的共识。 2.2 髋臼高位放置对髋关节功能影响和假体选择 尽管在避免髋臼外移前提下,适当上移不会明显增加关节反应力,但会对长期生物学固定造成一定影响。既往一些实验多使用金对金、金对普通聚乙烯等高摩擦界面,关节内轻度的负荷压力会加重摩擦界面的磨损,进而增加失败率[8-9]。而陶瓷界面和高交联聚乙烯衬垫的耐磨性能改善,可以将髋关节异常位置带来的关节反应力影响降到最低[10]。 然而并不是所有学者都支持髋臼高位放置技术。髋臼向上移位会导致肢体短缩,减少外展肌张力,并且增加脱位风险。关于髋臼高位放置后外展肌失效的难题,研究人员进行一系列体外实验研究。早期Jerosch等[11]通过20例尸体标本评估髋臼高位放置后外展肌功能,使用电脑测量高位放置状态下手术前后等肌肉力量和长度。分析结果证明对比假体置入前初始预测力量,外展肌力臂同时改变的影响对髋关节稳定性必要对肌肉力量从140%增加到250%。作者总结这样可以导致外展肌失效,所以不推荐髋臼高位放置。Delp等[12]通过模型计算髋关节和周围肌肉不同髋臼位置上的应力和力矩。研究显示如果股骨柄颈长度增加以恢复肌肉长度的话,向上放置臼杯可以减少了10%外展肌力臂。与此相反,外上方重建髋关节中心减少28%外展肌力臂,这样影响可能难以使用股骨柄颈长度来调整。国内学者通过模型模拟显示,在垂直上方或上外放置髋中心后,由于缩短了外展肌的力臂,减少了外展肌的力矩,对外展肌的功能造成了负面的影响[13]。Trendelenburg征可以反映臀中肌效能,Kiyama等[14]通过对比髋臼高位放置和低位放置两组,定性分析认为高位放置组Trendelenburg征明显高于对照组,且定量分析臀中肌肌力在高位放置组中降低。 臀中肌效能降低成为髋臼高位放置技术难以回避的问题,其继发的下肢不等长、脱位、撞击等会严重影响临床疗效。髋关节旋转中心位置改变会对髋关节活动度造成影响。目前研究认为髋关节屈曲和内旋过程中前方撞击主要为骨性撞击,旋转中心上移程度越高,撞击部位之间距离越大,而且越影响屈曲和内旋的活动度。所以这一系列问题只能通过股骨侧解。Shoji等[15]通过电脑模拟证实了股骨柄设计对活动度的影响。为避免前方撞击,可采用小颈干角高偏距假体,并且增加柄前倾的方法。郝跃峰等[13]通过模拟显示,上内放置臼杯后,在一定范围内,通过调整颈长和颈干角可以保持外展肌的力矩,找到保持髋关节接触力不变的位置。有国内研究对DDH患者行全髋关节置换时,在保证合适的假体安放位置和骨性包容的基础上,即使髋臼假体上移偏离解剖中心,只要术前设计合理和术中操作正确,术后对下肢长度恢复无明显不良影响[16]。远端固定锥形组配柄可在保持臀中肌效能同时,通过多种部件的组装配合来调整颈长、前倾角、offset、下肢长短,减少脱位,避免撞击,是在翻修中应用髋臼高位放置技术的必要选择。 大直径股骨头也可以改善术中稳定性。头的大小取决于臼杯尺寸,而髋臼上方骨量的高度和宽度决定了臼杯的大小。有效骨量覆盖决定了生物臼杯骨张入的面积,继而影响远期生物型固定效果。高位放置可以增加臼杯骨量覆盖,Nie等[17]研究显示大于50 mm臼杯高位放置可以保证80%的骨量覆盖。但这样通常限制了生物臼杯的尺寸。同时,随着多孔金属涂层性能的提高,以及jumbo杯理念的推广,臼杯与宿主骨接触面积的最低限值也逐渐降低。髋臼适当上移范围内,高位放置Jumbo杯可以在保证接触面积的同时使用大头以增加稳定性。但Jumbo杯会轻度增加髋关节旋转中心上移程度,Nwankwo等[18-19]通过影像学和计算模拟研究jumbo杯对旋转中心上移程度的影响。结果显示每增加1 mm磨锉将减少前柱0.86 mm的骨量,jumbo杯旋转中心平均上移1 mm。Gustke[20]回顾564例髋臼翻修术,29%的病例应用了Jumbo杯,而其中19%采用联合髋臼高位放置技术在部分复杂髋臼翻修中取得了良好的效果。Jumbo杯和髋臼高位放置均属于简化的手术方法,单独或联合使用都可以在取得良好临床效果同时,降低手术难度,减少手术时间。 2.3 髋臼上方骨量的解剖学和影像学研究 髋臼高位放置技术要求解剖中心上方有足够骨量处放置髋臼,增加髋臼有效覆盖,而髋臼上方骨量仅由髂骨提供。Xiao等[21]对120例国人骨盆进行CT扫描研究发现,在髂骨宽度和厚度在解剖旋转中心上25 mm(即臼顶处)最大,再向上移位明显减小,直径50 mm臼杯在上移10 mm处有43%的覆盖,上移35 mm处只有20%的覆盖。Antoniades等[22]对16例尸体骨盆进行了各旋转中心上移的高度髋臼重建研究,并结合CT测量髋臼高位放置后各层面髂骨的厚度,发现旋转中心距泪滴垂直距离35±3 mm处为髂骨骨量最充足高度,随后随旋转中心上移髂骨骨量明显减少。 由于发育不良,DDH髋臼侧解剖结构不同于普通髋臼。Komiyama等[23]对32例CroweⅡ或Ⅲ型患者进行髋关节CT扫描发现骨量覆盖在中心距泪滴30至35 mm处最大,而在40 mm以后减少。与此相似,Nie等[17]从影像学和生物力学角度研究CroweⅠ和Ⅱ型旋转中心在不同位置下臼顶应力变化,发现旋转中心超过解剖位 5 mm以上后臼顶骨量将明显减少,所以得出旋转中心上5 mm重建髋臼覆盖最大的结论。 2.4 髋臼高位放置的临床应用 髋臼骨缺损患者和松动的髋臼假体为关节医生带来众多挑战。巨大骨缺损难以解剖重建,现存重建方法很多,结构植骨配合半球形生物型髋臼假体结合螺钉固定是一种传统的重建髋臼解剖中心的方法,即刻初始稳定性确切并且费用较少,但是手术时间明显延长且远期随访报道出现植骨溶解及塌陷的比例较高,尤其是翻修中使用的是异体结构植骨,直接影响假体的远期稳定性。近年来流行采用钽金属骨小梁加强块技术,作为一种“不吸收的结构植骨”有替代结构植骨的优势,但是价格昂贵,对翻修患者经济负担较大。并且术中钽金属加强块需要根据缺损结构用磨钻塑形后钻孔螺钉固定,或为了适应加强块的形态而进一步磨锉稀缺的宿主骨,无疑增加手术难度及手术时间。目前中期的随访效果尚可,但远期疗效还有待于更多的长期跟踪随访支持。加强环和打压植骨技术适合巨大复杂的髋臼缺损,但是由于独特的技术挑战,报道结果也是混杂不一。 2.4.1 髋臼高位放置的适应证 对髋臼翻修病例,能通过磨锉使髋臼容纳半球形臼杯即是髋臼高位放置的适应证。但髋臼高位放置并非所有髋臼缺损的首选,重建正常旋转中心仍是首要目标,半球形生物大臼杯和加强块是多数严重缺损的主要翻修手段。对DDH病例,CroweⅡ、Ⅲ型或Hartfilakidis B型为适应证。 2.4.2 禁忌证 翻修中后柱严重骨缺损和骨盆连续性中断为髋臼高位放置的禁忌证。DDH中CroweⅠ、Ⅳ型或Hartfilakidis A、C型为其禁忌证。 2.4.3 髋臼高位放置在DDH中的临床疗效 DDH患者髋臼形态特征包括覆盖不全、空间较浅和骨量不足。在严重的DDH患者中会出现股骨头半脱位,甚至形成继发臼,因此这样难以实现髋臼处解剖位重建。通常可以使用大块骨结构植骨或颗粒骨植骨重建以降低旋转中心,但是对于生物型臼杯这样会减少假体与宿主骨直接接触,延长手术时间,增加异体植骨使用可能。植骨增加手术难度,对手术技术要求较高,术后发生骨吸收、骨不愈合概率增加,进而影响远期生物学固定。所以DDH患者中也常常应用髋臼高位放置技术解决臼杯重建的难题。 如表1所示,早期Pagnano等[24]报道117例CroweⅡ型DDH患者采用骨水泥臼杯结合髋臼高位放置技术,臼杯平均位置高于旋转中心15 mm,结果显示无论是否外移,都会增加松动及翻修率。而随着生物臼杯涂层材料的进步,髋臼高位放置结合生物臼杯取得了良好的临床结果。Murayama等[25]对43例 CroweⅡ和Ⅲ型DDH进行15年随访,其中10例为髋臼解剖位放置结合大块骨结构植骨,33例为单纯髋臼高位放置,高位放置组无失败,两组臼杯的年磨损率无明显差别。Nawabi等[4]也随访23例CroweⅡ和Ⅲ型患者使用生物型臼杯结合髋臼高位放置,10年随访结果令人满意。Kaneuji等[5]对30例应用髋臼高位放置结合生物臼杯治疗CroweⅠ至Ⅲ型DDH患者进行平均15年术后随访,结果显示无一例髋臼假体松动,作者认为DDH中在髋臼避免外移前提下,适度高位放置是一种行之有效的方法。Christodoulou等[26]报道34例螺旋臼杯高位放置结合Zweymuller柄治疗DDH患者,平均放置位置高于泪滴40 mm,与70例解剖位置对照组对比磨损率差异无显著性意义。国内学者Chen等[3]对37例采用髋臼高位放置的Harto?lakidis B型DDH患者进行平均6年随访,结果显示5年假体在位率90.3%,临床疗效显著。国内也有短期随访显示DDH结合髋臼高位放置技术均获得良好临床效果[16, 27-29]。总之,对于轻中度脱位的DDH,这种改变正常旋转中心的方法已取得明显的临床疗效,凭借其简化的特点将会得到更多主流学界的认可和接受。"
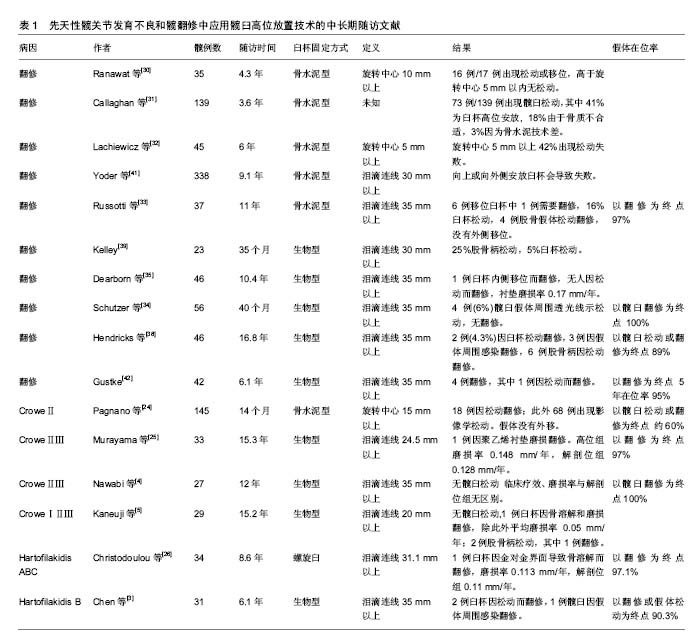

2.4.4 髋臼高位放置在翻修术中的临床疗效 与DDH相比,髋关节翻修术中髋臼侧骨缺损范围大,程度深,术中不确定性更高,而且取假体过程难以避免骨量丢失,增加手术难度。 髋关节翻修术的发展史也是学者对髋臼高位放置技术不断再认识的过程。早期受到涂层材料、摩擦界面、骨水泥技术、解剖学认识等局限,骨水泥臼杯结合髋臼高位放置的临床疗效令人失望。Ranawat等[30]早期报道平均4.3年随访,发现骨水泥臼杯高位放置的17例患者中16例出现松动和假体移位。Callaghan等[31]随访73例骨水泥髋关节翻修中30例发生松动。Lachiewicz等[32]报道42%的骨水泥髋臼假体翻修出现松动。早期髋关节金对普通聚乙烯摩擦界面的高磨损率加重假体松动,所以在使用骨水泥固定假体的情况下,髋臼高位放置技术逐渐为人淡忘,但随着生物型臼杯开始广泛应用,除应用于高脱位DDH的治疗,髋臼高位放置结合半球形生物型假体修复髋臼骨缺损也获得了较为理想的随访结果,见表1。Harris等[33]首先提出高旋转中心概念后与多名学者合作,在同一批患者基础上,持续多年随访并更新样本,相继汇报多篇在髋关节翻修中应用生物臼杯结合高旋转中心技术的随访结果[34-38],其中最长时间(16.8年)的随访报道假体在位率达89%以上,且临床疗效改善明显。此外Gustke[20]、Kelly[39]也报道各自长期随访结果,在位率均在95%以上。作者也报道了解放军总医院的中期随访结果,34例髋仅有1例因金对金反应出现假体松动再翻修,并且强调特小臼杯极度高位放置在个别严重髋臼缺损病例中具有不可替代的优点[40]。典型病例见图1。"


2.5 髋臼高位放置的定义及争议 目前髋臼高位放置技术中旋转中心上移程度尚无明确的标准,英文文献中对髋臼高位放置的命名未达成一致,检索文献可见“proximal placement”、“superior placement”、“high placement”、“high hip center”、“elevated hip center”等名称。而且所参照解剖标志仍不确定,多数学者以泪滴连线作为解剖标志基点测量上移程度的绝对值[41-42],或用非手术对侧旋转中心作为参考以排除个体差异。也有学者利用Ranawat三角法或Pierchon法确定正常旋转中心[43-44],测量结果相对精准,但操作较复杂。 DDH研究中,Fukui等[45]在DDH研究中将旋转中心距泪滴30 mm定为髋臼高位放置纳入标准。Christodoulou等[26]研究对象最低值也是30 mm。Kaneuji等[5]关于Crowe Ⅰ-Ⅲ型DDH应用髋臼高位放置技术中以旋转中心距泪滴20 mm作为纳入标准。Murayama等[25]取高位放置未知距泪滴连线25 mm的DDH患者作为研究对象。Pagnano等[24]将纳入标准制定在解剖位旋转中心 15 mm以上。此外还有学者认可传统高旋转中心(high hip center)的标准。 在髋关节翻修领域,早期Ranawat等[30]将正常旋转中心10 mm以上病例作为髋臼高位组。Russotti等[33]首先提出髋臼翻修中应用高旋转中心技术(High hip center),并将其定义为旋转中心距泪滴连线大于35 mm,此定义被广泛认可并采用。Dearborn等[35]在髋关节翻修中应用生物杯结合高旋转中心技术沿用此标准。Kelley[39]将此标准定为30 mm。由于旋转中心上移程度极高,高旋转中心定义可以成为髋臼高位放置概念的特殊范畴。Yoder 等[41]将髋臼高位放置等标准定位旋转中心距泪滴大于30 mm。Schutzer等[34]将研究纳入标准定在25 mm。 考虑到骨盆高度在国人与西方人种间存在差异,且个体身高差异对旋转中心高度有一定影响,国人的髋臼高位放置标准有待进一步完善。DDH的旋转中心变化程度通常小于翻修手术,此两类疾病应制定各自的旋转中心上移标准。而且从科研名称规范角度上讲,中英文文献对髋臼高位放置的定义未达成一致,此类在文献检索、引用和学术交流中潜在的问题急待解决。"

| [1] Charnley J. Total hip replacement by low-friction arthroplasty. Clin Orthop Relat Res.1970;72:7-21.[2] Johnston RC, Brand RA , Crowninshield RD. Reconstruction of the hip. A mathematical approach to determine optimum geometric relationships.J Bone Joint Surg Am.1979;61(5): 639-652.[3] Chen M, Luo ZL, Wu KR, et al. Cementless Total Hip Arthroplasty With a High Hip Center for Hartofilakidis Type B Developmental Dysplasia of the Hip: Results of Midterm Follow-Up.J Arthroplasty. 2016;31(5):1027-1034.[4] Nawabi DH, Meftah M, Nam D, et al. Durable fixation achieved with medialized, high hip center cementless THAs for Crowe II and III dysplasia. Clin Orthop Relat Res. 2014; 472(2):630-636.[5] Kaneuji A, Sugimori T, Ichiseki T, et al. Minimum Ten-Year Results of a Porous Acetabular Component for Crowe I to III Hip Dysplasia Using an Elevated Hip Center.J Arthroplasty. 2009;24(2):187-194.[6] Doehring TC, Rubash HE, Shelley FJ, et al. Effect of superior and superolateral relocations of the hip center on hip joint forces. An experimental and analytical analysis.J Arthroplasty. 1996;11(6):693-703.[7] Bicanic G, Delimar D, Delimar M, et al. Influence of the acetabular cup position on hip load during arthroplasty in hip dysplasia.Intl Orthop. 2009;33(2):397-402.[8] Smith AJ, Dieppe P, Vernon K, et al. Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales.Lancet. 2012; 379(9822):1199-1204.[9] Qu X, Huang X, Dai K. Metal-on-metal or metal-on-polyethylene for total hip arthroplasty: a meta-analysis of prospective randomized studies. Arch Orthop Trauma Surg. 2011;131(11):1573-1583.[10] Hu D, Tie K, Yang X, et al. Comparison of ceramic-on-ceramic to metal-on-polyethylene bearing surfaces in total hip arthroplasty: a meta-analysis of randomized controlled trials.J Orthop Surg Res. 2015;10:22.[11] Jerosch J, Steinbeck J, Stechmann J, et al. Influence of a high hip center on abductor muscle function. Arch Orthop Trauma Surg. 1997;116(6-7):385-389.[12] Delp SL, Wixson RL, Komattu AV, et al. How superior placement of the joint center in hip arthroplasty affects the abductor muscles.Clin Orthop Relat Res. 1996;(328):137-146.[13] 郝跃峰,孙俊英,杨佩彦,等. 有限高位髋关节旋转中心数学模型的推导[J].中华关节外科杂志(电子版),2007,1(3):161-167.[14] Kiyama T, Naito M, Shitama H, et al. Effect of superior placement of the hip center on abductor muscle strength in total hip arthroplasty.J Arthroplasty. 2009;24(2):240-245.[15] Shoji T, Yamasaki T, Izumi S, et al. The influence of stem offset and neck shaft angles on the range of motion in total hip arthroplasty.Int Orthop. 2016;40(2):245-253.[16] 黄志宇,张志奇,傅明,等. 髋臼假体上移放置对髋关节发育不良全髋关节置换术后下肢长度及功能的影响[J].中华骨科杂志, 2014,34(12):1225-1230.[17] Nie Y, Pei F, Li Z. Effect of high hip center on stress for dysplastic hip.Orthopedics. 2014;37(7):e637-643.[18] Nwankwo C, Dong NN, Heffernan CD, et al. Do jumbo cups cause hip center elevation in revision THA? A computer simulation.Clin Orthop Relat Res. 2014;472(2): 572-576.[19] Nwankwo CD, Ries MD. Do jumbo cups cause hip center elevation in revision THA? A radiographic evaluation.Clin Orthop Relat Res. 2014;472(9):2793-2798.[20] Gustke KA. Jumbo cup or high hip center: is bigger better? J Arthroplasty. 2004;19(4 Suppl 1):120-123.[21] Xiao JL, Zuo JL, Liu P, et al. Cross-sectional Anatomy of Ilium for Guiding Acetabular Component Placement Using High Hip Center Technique in Asian Population.Chin Med J (Engl). 2015;128(12):1579-1583.[22] Antoniades J, Pellegrini VD Jr. Cross-sectional anatomy of the ilium: implications for acetabular component placement in total hip arthroplasty. Clin Orthop Relat Res. 2012;470(12): 3537-3541.[23] Komiyama K, Nakashima Y, Hirata M, et al. Does High Hip Center Decrease Range of Motion in Total Hip Arthroplasty? A Computer Simulation Study.J Arthroplasty. 2016.[24] Pagnano W, Hanssen AD, Lewallen DG, et al. The effect of superior placement of the acetabular component on the rate of loosening after total hip arthroplasty.J Bone Joint Surg Am. 1996;78(7):1004-1014.[25] Murayama T, Ohnishi H, Okabe S, et al. 15-year comparison of cementless total hip arthroplasty with anatomical or high cup placement for Crowe I to III hip dysplasia.Orthopedics. 2012;35(3):e313-318.[26] Christodoulou NA, Dialetis KP, Christodoulou AN. High hip center technique using a biconical threaded Zweymuller cup in osteoarthritis secondary to congenital hip disease.Clin Orthop Relat Res. 2010;468(7):1912-1919.[27] 任鹏,柴伟,周勇刚,等. 人工全髋关节置换治疗CroweⅡ、Ⅲ型发育性髋关节发育不良—非骨水泥臼杯高旋转中心安放的短期随访结果[J].中华骨与关节外科杂志,2015,8(2):145-150.[28] 徐瑞泽,吴刚,张晓南,等. 选择不同髋臼旋转中心行髋关节发育不良全髋置换术后的短期疗效比较[J].中国医科大学学报, 2012, 41(8):756-758.[29] 陈凯,蔡俊丰,秦玉星,等. 髋臼发育不良全髋关节置换术髋臼旋转中心原位固定与上移的比较研究[J].中华关节外科杂志(电子版),2014,8(1):56-59.[30] Ranawat CS, Dorr LD, Inglis AE. Total hip arthroplasty in protrusio acetabuli of rheumatoid arthritis.J Bone Joint Surg Am. 1980;62(7):1059-1065.[31] Callaghan JJ, Salvati EA, Pellicci PM, et al. Results of revision for mechanical failure after cemented total hip replacement, 1979 to 1982. A two to five-year follow-up. J Bone Joint Surg Am. 1985;67(7):1074-1085.[32] Lachiewicz PF, McCaskill B, Inglis A, et al. Total hip arthroplasty in juvenile rheumatoid arthritis. Two to eleven-year results.J Bone Joint Surg Am. 1986;68(4):502-508.[33] Russotti GM, Harris WH. Proximal placement of the acetabular component in total hip arthroplasty. A long-term follow-up study.J Bone Joint Surg Am. 1991;73(4): 587-592.[34] Schutzer SF, Harris WH. High placement of porous-coated acetabular components in complex total hip arthroplasty.J Arthroplasty. 1994;9(4):359-367.[35] Dearborn JT, Harris WH. High placement of an acetabular component inserted without cement in a revision total hip arthroplasty. Results after a mean of ten years.J Bone Joint Surg Am. 1999;81(4):469-480.[36] Harris WH. Reconstruction at a high hip center in acetabular revision surgery using a cementless acetabular component. Orthopedics. 1998;21(9):991-992.[37] Hampton BJ, Harris WH. Primary cementless acetabular components in hips with severe developmental dysplasia or total dislocation. A concise follow-up, at an average of sixteen years, of a previous report.J Bone Joint Surg Am. 2006;88(7): 1549-1552.[38] Hendricks KJ, Harris WH. High placement of noncemented acetabular components in revision total hip arthroplasty. A concise follow-up, at a minimum of fifteen years, of a previous report. J Bone Joint Surg Am. 2006;88(10):2231-2236.[39] Kelley SS. High hip center in revision arthroplasty.J Arthroplasty. 1994;9(5):503-510.[40] 朴尚,周勇刚,杜银桥,等. 髋关节翻修术中生物型臼杯高位放置技术的可行性研究[J].中华骨科杂志,2016,36(23):1503-1511.[41] Yoder SA, Brand RA, Pedersen DR, et al. Total hip acetabular component position affects component loosening rates.Clin Orthop Relat Res. 1988;(228):79-87.[42] Gustke KA, Levering MF, Miranda MA. Use of jumbo cups for revision of acetabulae with large bony defects.J Arthroplasty. 2014;29(1):199-203.[43] 刘亚斌, 马信龙. Ranawat三角法对确定正常髋关节旋转中心的意义[J].中国组织工程研究,2015,19(17): 2625-2630.[44] Malik A, Wan Z, Jaramaz B, et al. A validation model for measurement of acetabular component position.J Arthroplasty. 2010;25(5):812-819.[45] Fukui K, Kaneuji A, Sugimori T, et al. How far above the true anatomic position can the acetabular cup be placed in total hip arthroplasty? Hip Int. 2013;23(2):129-134. |
| [1] | Xue Yadong, Zhou Xinshe, Pei Lijia, Meng Fanyu, Li Jian, Wang Jinzi . Reconstruction of Paprosky III type acetabular defect by autogenous iliac bone block combined with titanium plate: providing a strong initial fixation for the prosthesis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1424-1428. |
| [2] | Zhuang Zhikun, Wu Rongkai, Lin Hanghui, Gong Zhibing, Zhang Qianjin, Wei Qiushi, Zhang Qingwen, Wu Zhaoke. Application of stable and enhanced lined hip joint system in total hip arthroplasty in elderly patients with femoral neck fractures complicated with hemiplegia [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1429-1433. |
| [3] | Zhang Lichuang, Xu Hao, Ma Yinghui, Xiong Mengting, Han Haihui, Bao Jiamin, Zhai Weitao, Liang Qianqian. Mechanism and prospects of regulating lymphatic reflux function in the treatment of rheumatoid arthritis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1459-1466. |
| [4] | Yao Xiaoling, Peng Jiancheng, Xu Yuerong, Yang Zhidong, Zhang Shuncong. Variable-angle zero-notch anterior interbody fusion system in the treatment of cervical spondylotic myelopathy: 30-month follow-up [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1377-1382. |
| [5] | Zhang Jinglin, Leng Min, Zhu Boheng, Wang Hong. Mechanism and application of stem cell-derived exosomes in promoting diabetic wound healing [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1113-1118. |
| [6] | An Weizheng, He Xiao, Ren Shuai, Liu Jianyu. Potential of muscle-derived stem cells in peripheral nerve regeneration [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1130-1136. |
| [7] | Shao Yangyang, Zhang Junxia, Jiang Meijiao, Liu Zelong, Gao Kun, Yu Shuhan. Kinematics characteristics of lower limb joints of young men running wearing knee pads [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 832-837. |
| [8] | Huang Hao, Hong Song, Wa Qingde. Finite element analysis of the effect of femoral component rotation on patellofemoral joint contact pressure in total knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 848-852. |
| [9] | Yuan Jing, Sun Xiaohu, Chen Hui, Qiao Yongjie, Wang Lixin. Digital measurement and analysis of the distal femur in adults with secondary knee valgus deformity [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 881-885. |
| [10] | Zhou Jianguo, Liu Shiwei, Yuan Changhong, Bi Shengrong, Yang Guoping, Hu Weiquan, Liu Hui, Qian Rui. Total knee arthroplasty with posterior cruciate ligament retaining prosthesis in the treatment of knee osteoarthritis with knee valgus deformity [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 892-897. |
| [11] | Song Jiawei, Yang Yongdong, Yu Xing, Yang Jizhou, Wang Fengxian, Qu Yi, Bi Lianyong. Mid-term effect of Isobar EVO non-fusion dynamic fixation in the treatment of adjacent segment disease after lumbar fusion [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 908-913. |
| [12] | Xu Kuishuai, Zhang Liang, Chen Jinli, Ren Zhongkai, Zhao Xia, Li Tianyu, Yu Tengbo. Effect of force line changes on lower limb joints after medial open wedge high tibial osteotomy [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(6): 821-826. |
| [13] | Wang Shaoling, Wang Yanxue, Zheng Yaochao, Yu Shaojun, Ma Chao, Wu Shaoling. Feasibility of ultrasound-guided intra-articular injection in rabbit hip joint [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(5): 657-662. |
| [14] | Lu Qinxue, Xu Ning, Yang Yinglan, Han Qianqian, Duanmu Xianyu, Guo Yuwei, Han Qing. Femoroacetabular impingement: strength trainings for nerve-muscle, peripheral muscle and core muscle [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(5): 786-791. |
| [15] | Tang Jiping, Zhang Yeting. Exercise regulates adult hippocampal neurogenesis in Alzheimer’s disease: mechanism and role [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(5): 798-803. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||