Chinese Journal of Tissue Engineering Research ›› 2016, Vol. 20 ›› Issue (46): 6978-6985.doi: 10.3969/j.issn.2095-4344.2016.46.019
Previous Articles Next Articles
The research progress of clinical rehabilitation after acute Achilles tendon rupture
Wang Yu-zhong1, Wang Ji-hong2, Wen Shu-zheng2
- 1Inner Mongolia Medical University, Hohhot 010000, Inner Mongolia Autonomous Region, China; 2the Second Affiliated Hospital of Inner Mongolia Medical University, Hohhot 010000, Inner Mongolia Autonomous Region, China
-
Received:2016-08-22Online:2016-11-11Published:2016-11-11 -
Contact:Wang Ji-hong, M.D., Chief physician, Professor, the Second Affiliated Hospital of Inner Mongolia Medical University, Hohhot 010000, Inner Mongolia Autonomous Region, China -
About author:Wang Yu-zhong, Studying for master’s degree, Inner Mongolia Medical University, Hohhot 010000, Inner Mongolia Autonomous Region, China -
Supported by:the Natural Science Foundation of Inner Mongolia Autonomous Region, No. 2016MS0822; the Scientific and Technological Program of Science and Technology Department of Inner Mongolia Autonomous Region, No. kjt15sf16
CLC Number:
Cite this article
Wang Yu-zhong, Wang Ji-hong, Wen Shu-zheng. The research progress of clinical rehabilitation after acute Achilles tendon rupture[J]. Chinese Journal of Tissue Engineering Research, 2016, 20(46): 6978-6985.
share this article
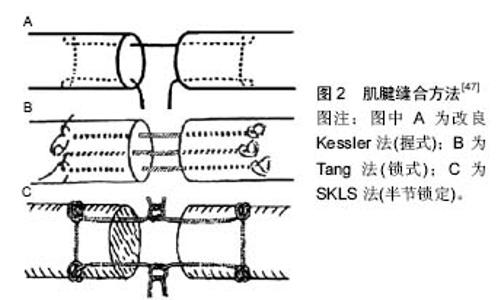
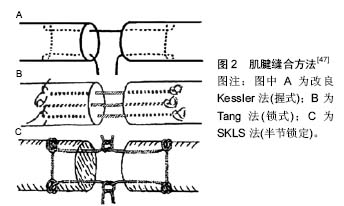
2 结果 Results 2.1 急性跟腱断裂的易发因素 2.1.1 年龄因素 跟腱的主要功能为屈小腿与足跖屈,急性跟腱损伤多由直接暴力、间接拉伤、切割伤所致,具有显著的流行病学特点。研究发现,运动性跟腱断裂的年龄分布呈正态分布曲线变化[7]。青壮年人群为正态分布的中间段,发病人数最密集,而在正态曲线的两端逐渐下降,也就是说年龄较小和较大的人群发病人数相对较少,这与跟腱强度大小,运动强度高低以及保护意识强弱等因素有关[8]。 2.1.2 解剖及病理因素 跟腱局部的解剖特点决定了跟腱组织本身血供较差,尤其跟腱中下端血供最少[9]。Stein等[10]通过放射性核素扫描研究证实跟腱中段血供最少,远端次之,近端最为丰富。某些基础疾病形成的病理改变也是发生跟腱断裂的诱因,如供血血管途径退变减少,跟腱结构也发生病理性退变,腓肠肌-比目鱼肌功能减退[11];应用某些药物,如类固醇类、氟喹诺酮类等[12-13];运动导致的跟腱过热等,导致跟腱组织不坚强,也是跟腱断裂的易发因素[14-15]。 2.1.3 外力运动性损伤因素 损伤机制主要包括2类[9],其一为外力直接切割或打击跟腱致其断裂,多为开放性损伤;其二为跟腱存在退行性变,加之猛然受力促其断裂,多为闭合性损伤。受力方式为膝关节伸直受力下踝关节突然跖曲受力、中立位踝关节突然背伸致其撕裂[16],多发生于羽毛球、篮球、足球、手球等运动过程中[17]。 2.2 跟腱断裂的诊断方法 对急性跟腱断裂的诊断包括:①详细的病史询问。临床上,跟腱断裂患者多主诉剧烈运动后跟腱局部突发疼痛,踝关节后方被打击感,甚至可闻及响声后出现患肢跖屈及背伸功能障碍;②完善的体格检查。体格检查时可见局部肿胀明显,伴有皮下瘀斑[7]。常用的临床检查试验有跟腱连续性触诊、Thompson试验(小腿三头肌挤压试验)、Matles试验(俯卧屈膝试验)、Copeland试验(血压计试验)和O'Brien试验(针刺试验)等。以上检查试验特点不同,其中Copeland试验和O'Brien试验有一定创伤性,依从性较差,临床上使用较少;跟腱连续性触诊检查在非麻醉状态及亚急性期敏感度较低;Thompson试验和Matles试验的敏感性显著高于其他临床检查,且简便易行,以上临床检查可准确有效地诊断急性跟键断裂[18];③影像学检查。跟腱闭合性断裂后会产生剧烈疼痛,查体患者不能合作可能造成一定的误诊、漏诊率,而B超、MRI等影像学检查是临床上作为诊断跟腱断裂及断裂类型的常用方法[19]。 2.3 影响跟腱愈合和功能恢复的因素 2.3.1 临床损伤类型因素 研究表明,跟腱断裂损伤情况多种多样,不同情况、不同类型的损伤也伴发不同组织损伤[16]。临床上,急性跟腱断裂按损伤特征一般归纳为横断型、撕脱型、撕裂型3个类型[9]。横断型多见于因切割伤所致的开放性损伤,其部位多在止点上3 cm左右,断端较整,近端可视损伤时间不同回缩3-5 cm。撕脱型多见于足跟腱遭受钝器砸伤,开放性或闭合性均可见,跟腱撕脱、断裂,断端不规则,甚至可回缩5 cm以上。撕裂型多见于剧烈运动者,于跟腱中段撕裂,断端呈马尾状,且多伴有退行性病理变化[19-20]。 不同类型的跟腱断裂损伤程度有所不同,失活跟腱组织的面积有所差别,故跟腱修复后愈合时间、愈合质量、愈合形式也有所不同。横断型跟腱断端较为整齐,失活组织较少,肌腱缝合后张力较小,血运重建更为容易,术后愈合情况好,功能恢复早[20]。撕脱型及撕裂型由于损伤较重,根据不同的损伤程度,有些术式需要进行肌腱坏死物质的清创,可导致肌腱缝合后张力较高,影响肌腱的血运,不利于肌腱的愈合,这种情况肌腱的修复更多需要依靠腱周组织[21]。 2.3.2 自身体质因素 跟腱损伤后愈合和功能恢复有赖于机体组织内外环境的调节,影响跟腱愈合的自身体质因素主要有4种:组织血运程度、基础疾病、服用药物及吸烟。 组织血运程度对肌腱愈合是至关重要的,而血运较少既是跟腱断裂的易发因素,又是影响跟腱愈合的根本原因[22]。某些自身基础疾病,诸如跟腱炎、糖尿病、自身免疫疾病及各种原因所致跟腱水肿、增厚等是发生跟腱断裂的诱因。McCormick等[23]通过分析糖尿病因素对肌腱愈合的影响,发现糖尿病组跟腱损伤修复术后发生并发症的概率明显高于非糖尿病组。一些临床研究认为,应用某些药物(如:非类固醇类抗炎药,肾上腺糖皮质激素类药物等)会导致肌腱水肿变性,从而使肌腱的强度减低[24];长期服用糖皮质激素或喹诺酮类抗生素导致跟腱变性成为影响跟腱愈合的间接因素[22]。Pajala等[22]研究认为使用皮质激素是增加术后并发症的重要因素。此外,吸烟也是影响跟腱的愈合重要因素之一[25]。Ishikawa等[26]认为吸烟影响远端肢体损伤的愈合;Pajala等[22]认为吸烟会导致末梢血管的挛缩,从而使肌腱修复后血运减少,延缓肌腱的愈合,甚至造成肌腱坏死。吸烟影响肌腱愈合的具体机制尚需进一步探究。 2.3.3 治疗方式 由于跟腱的独特功能,修复治疗是极为重要的。目前,急性跟腱断裂常规的治疗方法包括保守治疗、传统开放手术及经皮微创手术[27-28]。3种方式治疗急性跟腱断裂均得到临床肯定,但各有利弊,临床医师多根据患者的具体情况选择适当的治疗方法。 保守治疗:可以避免感染、切口不愈合、瘢痕形成等手术带来的相关问题,以往观点认为,跟腱断裂保守治疗相比手术治疗再断裂率较高。Keating等[17]通过研究发现,随机对照组中保守治疗和手术治疗急性跟腱断裂的再断裂率分别为9.8%和5.1%。Nilsson-Helander等[29]设计的随机对照研究同样发现保守治疗与手术治疗相比具有较高的跟腱再断裂率(12.5% vs. 4.1%)。而近期研究有观点补充认为,保守治疗后早期功能锻炼可以减少跟腱再断裂的发生[30]。大样本研究表明,使用足部矫形器进行跟腱断裂后保守治疗可以明显降低其再断裂率,但治疗周期较长[31]。虽然保守临床观察尚可,但相比手术治疗其再断裂发生率较高,且功能锻炼没有统一标准,安全性尚需考究[30]。 传统开放手术:作为治疗跟腱断裂的经典术式,具有术野相对直观、效果相对肯定、操作相对简单的特点。治疗过程充分暴露跟腱断端,准确牢固的修复断裂跟腱,可根据损伤类型的差异性采用不同的方法进行修复。Keyhani等[32]应用开放手术方式治疗32例急性跟腱损伤患者,用肌腱和筋膜将其覆盖,术后恢复好,随访表明,此方法可降低术后并发症发生率。卜晗等[33]应用开放式手术移植肌腱治疗23例不同分型的跟腱断裂患者,术后观察恢复情况均未发生感染及伤口不愈合。也有研究认为,多种开放式手术治疗急性跟腱断裂效果均可肯定,术后随访均恢复较好,但因术中需充分显露而牵拉皮肤和充分的剥离腱膜,较大的损伤了腱周组织的血运,容易出现术后感染、瘢痕粘连、皮肤和跟腱坏死等术后并发症,发生率高达10%-20%[34-35]。 经皮微创手术:目前,微创手术术式多样,多数认为,修复肌腱有手术切口小、组织损伤小、术后恢复快等优点。但治疗过程不能充分的暴露跟腱,术中操作难度较大,较容易发生腓肠神经损伤,缝合强度也明显劣于开放手术[36],跟腱再断裂、跟腱延长也较容易发生[37]。石波等[38]应用双小切口治疗跟腱断裂,愈后较好,且对肌腱损伤较少,术后恢复快,瘢痕小。陈华等[39]应用经通道辅助缝合系统修复急性跟腱断裂,延续了其他微创手术的优点且通道不经过腓肠神经,使腓肠神经损伤的概率减小。祁洁等[40]发现跟腱损伤后断端多为马尾状,给临床修复带来很大困难,然而应用铆钉固定于跟骨不仅可以减少对跟腱断端的过分加压而导致血运减少,也减少了缝合的难度,减轻了患者的痛苦。而Lin等[41]认为跟腱同肩袖损伤类似,因而应用Suture Bridge双排固定技术治疗9名跟腱损伤患者,术后踝关节能较好地恢复正常活动。还有一些研究表明,微创切口治疗新鲜跟腱断裂疗效满意,可以减少切口并发症[42-43]。 2.3.4 缝合方法 缝合方法对肌腱修复、愈合有着重要影响,肌腱缝合最经典的缝合方法为改良Kessler法[44]。为寻找力学特性最佳、损伤最小、操作最简便的缝合方式,增加其抗张能力及断端的光滑度,促进肌腱早期愈合,国内外学者进行了研究、改进和引申,新的缝合方法层出不穷,目前文献报道及临床常用的缝合方法还有ZM法、Bunnell法、Tang法、SKLS法、Halsted法及联合缝合法等,各种缝合方法根据缝合结构不同又可分为锁式结构和握式结构[44-47]。锁式结构能够有效的锁住肌腱组织,加强缝合强度;而握式缝合则对肌腱的抓锁能力较小,在外力作用下脱落、撕脱可能性大,因此锁式比握式更有效抵御间隙形成,加大缝合强度(图2)[45]。"
| [1] Nyyssönen T, Lüthje P, Kröger H. The increasing incidence and difference in sex distribution of Achilles tendon rupture in Finland in 1987-1999. Scand J Surg. 2008;97(3):272-275. [2] Freedman BR, Gordon JA, Soslowsky LJ. The Achilles tendon: fundamental properties and mechanisms governing healing. Muscles Ligaments Tendons J. 2014;4(2):245-255. [3] 姜楠,相大勇,余斌.急性跟腱断裂治疗的研究进展[J].中国修复重建外科杂志,2013,27(5):628-632. [4] 伍亮,熊小龙,相大勇,等.TGF-β1和VEGF在富血小板血浆治疗跟腱断裂模型中的表达及意义[J].中华临床医师杂志(电子版),2013,7(4):1639-1645. [5] Katzel EB, Wolenski M, Loiselle AE, et al. Impact of Smad3 loss of function on scarring and adhesion formation during tendon healing. J Orthop Res. 2011; 29(5):684-693. [6] Wong JK, Lui YH, Kapacee Z, et al. The cellular biology of flexor tendon adhesion formation: an old problem in a new paradigm. Am J Pathol. 2009;175(5): 1938-1951. [7] 薛剑锋,施忠民.急性跟腱断裂诊断与治疗进展[J].国际骨科学杂志,2013,34(1):29-31. [8] 杨威,苏伟,李书振,等.南宁市运动性跟腱断裂的流行病学调查[J].广西医科大学学报,2013,30(5):810-812. [9] 胥少汀,葛宝丰,徐印坎.实用骨科学[M].4版.人民军医出版社,2014. [10] Stein V, Laprell H, Tinnemeyer S, et al. Quantitative assessment of intravascular volume of the human Achilles tendon. Acta Orthop Scand. 2000;71(1): 60-63. [11] Maffulli N. Achilles tendon rupture. Br J Sports Med. 1995;29(4):279-280. [12] McQuillan R, Gregan P. Tendon rupture as a complication of corticosteroid therapy. Palliat Med. 2005;19(4):352-353. [13] Seeger JD, West WA, Fife D, et al. Achilles tendon rupture and its association with fluoroquinolone antibiotics and other potential risk factors in a managed care population. Pharmacoepidemiol Drug Saf. 2006;15(11):784-792. [14] Wilson AM, Goodship AE. Exercise-induced hyperthermia as a possible mechanism for tendon degeneration. J Biomech. 1994;27(7):899-905. [15] Birch HL, Wilson AM, Goodship AE. The effect of exercise-induced localised hyperthermia on tendon cell survival. J Exp Biol. 1997;200(Pt 11):1703-1708. [16] Arner O, Lindholm A. Subcutaneous rupture of the Achilles tendon; a study of 92 cases. Acta Chir Scand Suppl. 1959;116(Supp 239):1-51. [17] Keating JF, Will EM. Operative versus non-operative treatment of acute rupture of tendo Achillis: a prospective randomised evaluation of functional outcome. J Bone Joint Surg Br. 2011;93(8): 1071-1078. [18] Chiodo CP, Glazebrook M, Bluman EM, et al. American Academy of Orthopaedic Surgeons clinical practice guideline on treatment of Achilles tendon rupture. J Bone Joint Surg Am. 2010;92(14):2466-2468. [19] 王丽华.急性闭合性跟腱断裂高频超声与低场MRI诊断价值的比较[J].中国临床医学影像杂志,2012,23(10): 748-750. [20] McMahon SE, Smith TO, Hing CB. A meta-analysis of randomised controlled trials comparing conventional to minimally invasive approaches for repair of an Achilles tendon rupture. Foot Ankle Surg. 2011;17(4):211-217. [21] 刘诚.肌腱修复愈合影响因素的研究[J].重庆医学,2011, 40(22):2273-2275. [22] 邵雷,张长青,陈圣宝.跟腱术后再断裂的相关因素分析[J].实用骨科杂志,2010,16(10):743-746. [23] McCormack RG, Leith JM. Ankle fractures in diabetics. Complications of surgical management. J Bone Joint Surg Br. 1998;80(4):689-692. [24] Pajala A, Kangas J, Ohtonen P, et al. Rerupture and deep infection following treatment of total Achilles tendon rupture. J Bone Joint Surg Am. 2002;84-A(11): 2016-2021. [25] 桑伟林,马金忠.跟腱断裂影响因素及发生机制[J].国际骨科学杂志,2006,27(2):105-107. [26] Ishikawa SN, Murphy GA, Richardson EG. The effect of cigarette smoking on hindfoot fusions. Foot Ankle Int. 2002;23(11):996-998. [27] Leppilahti J, Puranen J, Orava S. Incidence of Achilles tendon rupture. Acta Orthop Scand. 1996;67(3): 277-279. [28] Jones MP, Khan RJ, Carey Smith RL. Surgical interventions for treating acute achilles tendon rupture: key findings from a recent cochrane review. J Bone Joint Surg Am. 2012;94(12):e88. [29] Nilsson-Helander K, Silbernagel KG, Thomeé R, et al. Acute achilles tendon rupture: a randomized, controlled study comparing surgical and nonsurgical treatments using validated outcome measures. Am J Sports Med. 2010;38(11):2186-2193. [30] Metz R, Verleisdonk EJ, van der Heijden GJ, et al. Acute Achilles tendon rupture: minimally invasive surgery versus nonoperative treatment with immediate full weightbearing--a randomized controlled trial. Am J Sports Med. 2008;36(9):1688-1694. [31] Wallace RG, Heyes GJ, Michael AL. The non-operative functional management of patients with a rupture of the tendo Achillis leads to low rates of re-rupture. J Bone Joint Surg Br. 2011;93(10):1362-1366. [32] Keyhani S, Mardani-Kivi M, Abbasian M, et al. Achilles tendon repair, a modified technique. Arch Bone Jt Surg. 2013;1(2):86-89. [33] 卜晗,张梅刃,蒋际钊,等.基于跟腱断裂Kuwade分型采用三种自体肌腱移植重建方法的临床疗效分析[J].中华移植杂志(电子版).2014,8(2):85-89 [34] ?liwa M. Percutaneous and minimally invasive Achilles tendon repair - review of surgical techniques. Pol Orthop Traumatol. 2014;79:92-96. [35] Movin T, Ryberg A, McBride DJ, et al. Acute rupture of the Achilles tendon. Foot Ankle Clin. 2005;10(2):331-356. [36] Keyhani S, Mardani-Kivi M, Abbasian M, et al. Achilles tendon repair, a modified technique. Arch Bone Jt Surg. 2013;1(2):86-89. [37] Chiodo CP, Wilson MG. Current concepts review: acute ruptures of the achilles tendon. Foot Ankle Int. 2006; 27(4):305-313. [38] 石波,李宗原.双小切口手术修复急性闭合性跟腱断裂[J].中国骨伤,2015,28(9):820-823. [39] 陈华,郝明,张巍,等.经通道辅助缝合系统微创修复急性闭合跟腱断裂的疗效观察[J].中国修复重建外科杂志, 2015, 29(1):35-38. [40] 祁洁,段亮,李伟伟,等.带线锚钉半Kessler缝合法修复自发性跟腱断裂[J].中国修复重建外科杂志,2016,30(2): 165-168. [41] Lin Y, Wang ZW, Zhang B, et al. Central tendon splitting combined with SutureBridge double-row technique as a surgical treatment for insertional Achilles tendinopathy. Chin Med J (Engl). 2013; 126(20):3860-3864. [42] Del Buono A, Volpin A, Maffulli N. Minimally invasive versus open surgery for acute Achilles tendon rupture: a systematic review. Br Med Bull. 2014;109:45-54. [43] Keller A, Ortiz C, Wagner E, et al. Mini-open tenorrhaphy of acute Achilles tendon ruptures: medium-term follow-up of 100 cases. Am J Sports Med. 2014;42(3):731-736. [44] 白庆兵,张哲敏,邵新中,等.两种肌腱缝合方法的对比研究[J].中华手外科杂志,2012,28(5):303-306. [45] Hotokezaka S, Manske PR. Differences between locking loops and grasping loops: effects on 2-strand core suture. J Hand Surg Am. 1997;22(6):995-1003. [46] 李吉友.大鼠跟腱断裂缝合中3种肌腱缝合方法的生物力学和组织学比较[J].中国组织工程研究与临床康复,2009, 13(37):7305-7308. [47] 郑振伟,李朝旭.三种缝合方法一期修复屈指肌腱的临床疗效分析[J].实用医药杂志,2013,30(11):980-981. [48] Tang JB, Wang B, Chen F, et al. Biomechanical evaluation of flexor tendon repair techniques. Clin Orthop Relat Res. 2001;(386):252-259. [49] 徐海栋,赵建宁,卢俊浩,等.聚乳酸防粘连膜在肌腱修复中的应用[J].中国组织工程研究,2012,16(16):3025-3028. [50] Yasuda T, Kinoshita M, Abe M, et al. Unfavorable effect of knee immobilization on Achilles tendon healing in rabbits. Acta Orthop Scand. 2000;71(1):69-73. [51] 王振宇.制动对骨关节影响的研究现状[J].医学综述, 2012,18(7):1066-1068. [52] Killian ML, Cavinatto L, Galatz LM, et al. The role of mechanobiology in tendon healing. J Shoulder Elbow Surg. 2012;21(2):228-237. [53] Wang J, Jiang D, Wen S, et al. Improved Achilles tendon healing by early mechanical loading in a rabbit model. Int J Clin Exp Med. 2015;8(1):1144-1149. [54] Bayer ML, Schjerling P, Herchenhan A, et al. Release of tensile strain on engineered human tendon tissue disturbs cell adhesions, changes matrix architecture, and induces an inflammatory phenotype. PLoS One. 2014;9(1):e86078. [55] 罗伦,董晖,杨映月,等.手伸指肌腱修复术后康复方案临床疗效对比观察[J].华西医学,2014,29(2):289-292. [56] Wang JH, Guo Q, Li B. Tendon biomechanics and mechanobiology--a minireview of basic concepts and recent advancements. J Hand Ther. 2012;25(2): 133-140; quiz 141. [57] 李兰春.60例屈指肌腱修复术后的康复治疗[J].中国医药科学,2013,3(19):208-209. [58] 王继宏,温树正,樊东升,等.医用可吸收防粘连膜在肌腱修复中的临床应用[J].中华临床医师杂志(电子版), 2014, 8(7):1372-1374. [59] Hakimi O, Murphy R, Stachewicz U, et al. An electrospun polydioxanone patch for the localisation of biological therapies during tendon repair. Eur Cell Mater. 2012;24:344-357; discussion 357. [60] 田明波,李守峰.医用可吸收膜和玻璃酸钠在肌健修复术中的应用效果分析[J].中医正骨,2011,23(8):17-19. [61] 王继宏,温树正.可吸收表皮生长因子复合膜防止肌腱粘连的研究[J].中国组织工程研究与临床康复, 2011,15(21): 3900-3904. [62] Demirkan F, Colakoglu N, Herek O, et al. The use of amniotic membrane in flexor tendon repair: an experimental model. Arch Orthop Trauma Surg. 2002; 122(7):396-399. [63] Bernardo V, Luz GM, Alves NM, et al. Cell behaviour in new poly(l-lactic acid) films with crystallinity gradients. Mater Lett. 2012,87(1):105-108. [64] Lu H, Qin L, Fok P, et al. Low-intensity pulsed ultrasound accelerates bone-tendon junction healing: a partial patellectomy model in rabbits. Am J Sports Med. 2006;34(8):1287-1296. [65] 刘沐青,于志军,秦永平,等.低强度脉冲超声波对肌腱愈合的促进作用[J].现代生物医学进展,2014,14(10):1879-1882. [66] 李敏.一氧化氮与肌腱愈合[J].中国组织工程研究, 2012, 16(50):9496-9500. [67] Osarumwense D, Wright J, Gardner K, et al. Conservative treatment for acute Achilles tendon rupture: survey of current practice. J Orthop Surg (Hong Kong). 2013;21(1):44-46. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [3] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [4] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [5] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [6] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [7] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [8] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [9] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [10] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [11] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [12] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| [13] | Mo Jianling, He Shaoru, Feng Bowen, Jian Minqiao, Zhang Xiaohui, Liu Caisheng, Liang Yijing, Liu Yumei, Chen Liang, Zhou Haiyu, Liu Yanhui. Forming prevascularized cell sheets and the expression of angiogenesis-related factors [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3479-3486. |
| [14] | Liu Chang, Li Datong, Liu Yuan, Kong Lingbo, Guo Rui, Yang Lixue, Hao Dingjun, He Baorong. Poor efficacy after vertebral augmentation surgery of acute symptomatic thoracolumbar osteoporotic compression fracture: relationship with bone cement, bone mineral density, and adjacent fractures [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3510-3516. |
| [15] | Liu Liyong, Zhou Lei. Research and development status and development trend of hydrogel in tissue engineering based on patent information [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3527-3533. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||