Chinese Journal of Tissue Engineering Research ›› 2014, Vol. 18 ›› Issue (21): 3406-3411.doi: 10.3969/j.issn.2095-4344.2014.21.022
Previous Articles Next Articles
Relationship between implant design and marginal bone loss around oral implants: current situation and controversy
Li Ping 1, 2, Dai Jing-tao 1, 2, Li An2, Tang You-chao1
- 1 Huizhou Stomatological Hospital of Jinan University, Huizhou 516000, Guangdong Province, China; 2 Jinan University Medical School, Guangzhou 510000, Guangdong Province, China
-
Online:2014-05-21Published:2014-05-21 -
Contact:Tang You-chao, Chief physician, Huizhou Stomatological Hospital of Jinan University, Huizhou 516000, Guangdong Province, China -
About author:Li Ping, Studying for master’s degree, Physician, Huizhou Stomatological Hospital of Jinan University, Huizhou 516000, Guangdong Province, China -
Supported by:the Science and Technology Plan Project of Huizhou City, No. 2013Y115
CLC Number:
Cite this article
Li Ping, Dai Jing-tao, Li An, Tang You-chao. Relationship between implant design and marginal bone loss around oral implants: current situation and controversy [J]. Chinese Journal of Tissue Engineering Research, 2014, 18(21): 3406-3411.
share this article
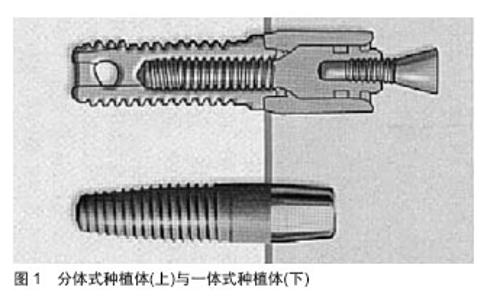
2.1 一体式种植体 种植体穿黏膜颈部与种植体位于骨内的体部合为一体,为一体式种植体(图1)。种植体颈部位于软组织之内,平台可以位于牙槽嵴表面的软组织之内或软组织之外,故也称为软组织水平种植体。 临床发现,一体式种植体不存在微间隙及二期手术引起的上皮连接顶端的微动,故更有利于保存种植体颈部骨组织。Finne等[4]通过对82个一体式种植体周围边缘骨重建及软组织健康进行3年临床观察,种植体3年存留率为98.8%。一体式种植体具有保持边缘骨水平稳定、软组织健康及高生存率等优点,故认为一体式种植体第1年骨重建后能较好地维持种植体周围软硬组织。Huang等[5]在36例患者的36 个5.0-6.0 mm缺牙间隙处植入直径2.5 mm或3.0 mm的一体式小直径种植体36颗,种植义齿龈缘与邻牙龈缘曲线协调,龈乳头充盈,美学效果理想,因此对间隙小于6 mm的缺牙间隙采用一体式小直径种植体可以取得满意的临床效果。 2.2 种植体颈部 种植体颈部是指种植体的冠方部分,骨水平和软组织水平两种种植体的颈部设计是两种不同理念。"
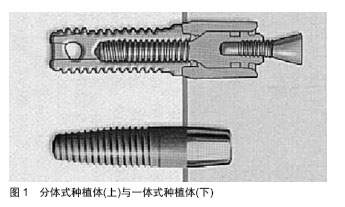
2.2.1 骨水平种植体颈部设计 骨水平种植体的设计理念是种植体平台与牙槽嵴顶齐平或位于根方(图2)。种植体颈部设计采用光滑表面,其主要基于菌斑易于附着在粗糙表面的假说。事实上,有学者对于光滑颈部设计与微螺纹颈部设计的骨水平种植体的临床研究发现,二者在探诊深度上存在显著性差异,粗糙表面更加有利于结缔组织和上皮组织附着,能有效减少边缘骨吸收[6]。 种植体颈部采用微螺纹设计与传统光滑颈部设计相比较,更有利于种植体颈部骨量的长期维持。Meriç等[7]利用三维有限元应力分析,研究表明微螺纹种植体颈部设计能有效改变种植体颈部的应力分布,将种植体传递给骨-种植体界面的剪切力转变为压应力或拉应力,从而减少了基台连接部和种植体周围骨密质的应力。Abrahamsson等[8]通过动物实验研究还发现微螺纹颈部结构能为骨结合提供更好的条件,减少种植体颈部骨吸收。同样,Lee等[9]临床前瞻性研究证实了在种植负载后,微螺纹颈部设计有利于种植体边缘骨水平维持。 2.2.2 软组织水平种植体颈部设计 软组织水平种植体是指种植体颈部位于软组织之内,平台可以位于牙槽嵴表面的软组织之内或软组织之外。软组织水平种植体存在光滑颈部,其部分植入牙槽嵴,或完全位于软组织内,则光滑颈部发生软组织愈合(即软组织封闭)。与骨组织种植体相比,软组织水平种植体平台的垂直向位置向冠方转移,使种植体平台与基台的微间隙向冠方移位,避免连接处的微动和微间隙处的病原微生物对种植体周围骨组织的刺激,将有利于保持种植体周围软组织结合与骨结合的长期稳定[10]。但是,刘健等[11]研究发现,在排除了负重条件和表面处理技术等影响因素下,就种植体边缘骨吸收而言,骨水平种植体肯定会明显优于软组织水平种植体。 2.3 种植体-基台连接 基台与种植体的连接方式称为基台连接,种植体平台中心存在向冠方凸起或凹陷到种植体内部的结构设计,分别称为外基台连接和内基台连接。基台与种植体的接触边界称为种植体-基台界面,其所形成的间隙称为微间隙。该处有处有明显的炎症细胞聚集,并且在微间隙上下0.5-0.75 mm 范围构成炎性结缔组织渗漏带[12]。故种植体-基台连接处微间隙内的微生物聚集及渗透,引起种植体周围炎症,并最终导致炎症细胞趋化聚集、促进破骨细胞形成和生长,引起种植体周围骨吸收。若种植体-基台连接处远离牙槽嵴骨,则能减少种植体周围边缘骨吸收[13]。 "

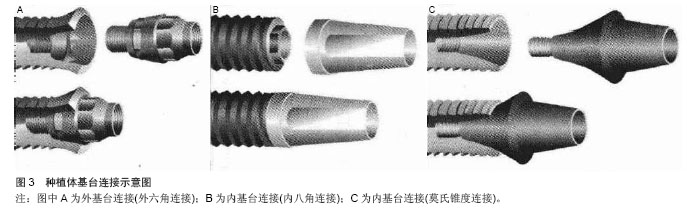
2.3.1 外基台连接 外基台连接是指基台与种植体顶部表面接触,根据几何形状分类为:外六角连接,外八角连接,花键连接等等(图3A)。与内基台连接相比,外连接存在抗侧向能力不足和螺丝易松动的缺陷,但目前仍然在临床上应用,尤其在小直径种植体设计内连接结构受到种植体颈部直径限制时。Weng等[14]研究显示不同的基台连接将引起不同的种植体周围骨组织缺损,其中外基台连接的种植体引起骨缺损量尤为显著。高奎英[15]通过动物研究发现在相同负荷且种植体直径相同情况下,外六角形连接种植体周围骨组织所受应力大于内六角形种植体周围骨组织所受应力。 2.3.2 内基台连接 内基台连接是指种植体平台冠方没有凸起的固位结构,为深入种植体的内凹设计。基台深入种植体内依靠相应的设计实现抗自身旋转,达到基台固位,抗剪切,定位等作用(图3B)。莫氏锥度连接是基台内连接的一种方式,种植体-基台连接只有锥度结构,没有螺丝,完全依靠锥度壁产生的机械摩擦固位力(图3C)。其主要特点在于:第一,莫氏锥度连接微生物封闭性良好,能够消除种植体-基台界面存在的微间隙,因此避免了微生物在种植体-基台界面处聚集。第二,莫氏锥度连接具有较强的机械稳定性,降低基台的微动,从而避免螺丝、基台松动等[16]。种植体-基台连接采用莫氏锥度设计,能够有效减少微间隙和微动,从而减少种植体周围边缘骨吸收。"

2.3.3 平台转移 近年来,Baumgarten[17]和Porter 等[18]相继提出平台转移概念:在骨水平种植体平台上,基台直径小于平台直径,使基台连接位置向种植体平台中心内移(图4)。 大部分临床试验及动物实验表明,平台转移技术可以有效降少种植体周围的垂直向骨吸收。Calvo-Guirado等[19]进行前瞻性临床研究,评估64颗前牙美学区的平台转移种植体的骨吸收情况,观察5年后发现种植体边缘骨水平稳定且美学效果良好,平均骨吸收为(0.97±0.39) mm,同时发现仅少数患者唇侧牙龈退缩。同样,有研究表明平台转移种植体在功能负重 12个月后,平台转移设计可以有效减少种植体颈部骨吸收,维持种植体周围骨组织的稳定性[20]。Farronato 等[21]通过动物实验证实,在种植体平台与牙槽嵴顶齐平下,平台转移种植体结合上皮宽度较窄,而其对结缔组织影响不大。此外,平台转移导致牙槽嵴顶吸收平均为0.58 mm。Çimen等[22]利用三维有限元分析发现,平台转移能够将骨-种植体界面应力有效转移,降低种植体颈部周围骨组织应力,从而维持种植体周围边缘骨稳定,但也存在基台和基台螺丝折断的风险。 2.4 种植体的尺寸 种植体的尺寸包括种植体的直径与长度。 2.4.1 种植体直径 种植体体部直径:对螺纹种植体而言,种植体体部直径分为不包含螺纹的内径和包含螺纹的外径,习惯上将种植体外径称为种植体体部直径,临床上简称为“种植体直径”。早期种植体设计,常规使用直径3.75 mm的螺纹状种植体,壁厚度为0.4 mm,通常被称为标准直径种植体。大直径种植体(粗种植体)直径大于4.5 mm,而小直径种植体(细种植体)直径小于3.5 mm[23]。 种植体直径增加,表面积显著增加,直径每增加 1 mm表面积约增加25%。根据三维有限元分析,增加种植体表面积可以减少骨结合界面应力集中[24]。Jang等[25]进行影响种植体存留率的回顾性研究发现,粗种植体可以增加骨-种植体接触界面的面积,相应减少单位面积内应力分布,从而更有利于减少种植体周围蝶形骨吸收。有学者认为,在长期负载情况下,种植体周围骨皮质会出现应力峰值,而骨界面应力值与种植体直径与长度均呈负相关。在保证种植体周围足够骨量的前提下,大直径种植体明显增加了骨-种植体接触面积,以最大限度地减小单位面积内的应力,从而能减少种植体周围骨的丧失,发挥种植体的支持和固位作用[26]。 种植体平台直径:种植体颈部为种植体的冠方部分,最冠方称为种植体平台。种植体平台直径小于体部直径。种植体平台直径小于体部直径,为一种新的种植体颈部形态设计(如Bicon,NobelActive)。其设计理念为尽可能地增加种植体平台周围的骨量,并改善软组织附着质量。"


斜肩式平台设计种植体(如Bicon种植系统)将种植体平台种植体与体部螺纹设计成一个冠方小根方大的圆台状(图5)。连接修复基台后,与种植体平台外径形成平台转换的效果,增加种植体平台周围骨量附着,从而减小种植体颈部周围骨组织应力[27]。程亚楠等[28]利用影像学方法评估平齐对接种植体、小平台转换种植体及斜肩式平台种植体的边缘骨吸收的差别,修复负载3个月后,平台转换种植体近、远中边缘骨吸收量明显优于平齐对接种植体;其中斜肩式平台种植体在种植体周围边缘骨吸收量最少,部分种植体周围边缘骨骨量略有增加。 2.4.2 种植体长度 种植体长度是指种植体植入骨内部分的长度。目前骨水平种植体是指整个种植体长度,软组织水平种植体是指种植体粗糙表面的体部长度,不包括光滑颈部高度。多数种植体系统中,种植体长度在6-16 mm之间。 增加种植体长度的优点在于增加骨-种植体界面的表面积,增强抗侧向负荷的能力。de Carvalho[29]通过三维有限元应力分析表明,种植体越长其周围骨组织的应力值越小,尤其是平台转移设计的种植体。Himmlová等[30]认为增加种植体直径对与分散骨组织应力影响最显著。在其他相关因素相同的情况下,为了分散骨组织的应力,增加种植体长度并不如改变种植体直径的效果显著[31-42]。但尚未有研究证明种植体成功率与种植体长度之间存在线性关系。"

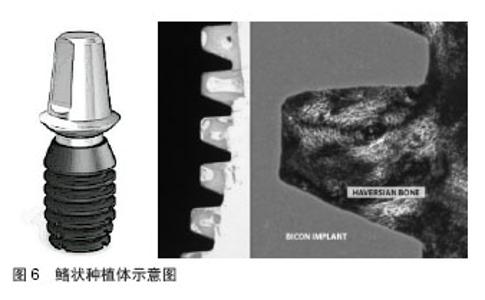
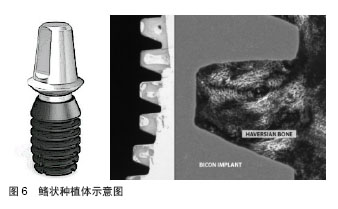
在特殊解剖部位,条件受限时,可以使用较短种植体,但应该考虑增加种植体的数量或直径。某些特殊几何形状设计的超短种植体,例如Bicon鳍状种植体最短者只有4.8 mm,以适应上颌与下颌磨牙区的可用骨高度不足,其临床效果得到肯定[43](图6)。"
| [1]Albrektsson T,Zarb G,Worthington P,et al.The long-term efficacy of currently used dental implants: A review and proposed criteria of success.Int J Oral Maxillofac Implants. 1986;1(1):11-25. [2]郁雪松,赵黎,潘世源.种植体周围骨吸收的时间因素[J].中国组织工程研究与临床康复, 2012,15(48):9093-9095. [3]Qian J,Wennerberg A,Albrektsson T.Reasons for marginal bone loss around oral implants.Clin Implant Dent Relat Res. 2012;14(6):792-807. [4]Finne K,Rompen E,Toljanic J.Three-year prospective multicenter study evaluating marginal bone levels and soft tissue health around a one-piece implant system.Int J Oral Maxillofac Implants.2012;27(2):458. [5]Huang J,Zhao J,Liu Q,et al.Clinical research of immediate restoration implant with mini-implants in edentulous space. Hua Xi Kou Qiang Yi Xue Za Zhi.2010;28(4):412. [6]Eraslan O,?nan Ö.The effect of thread design on stress distribution in a solid screw implant: A 3d finite element analysis.Clin Oral Investig.2010; 14(4):411-416. [7]Meriç G,Erkmen E,Kurt A,et al.Biomechanical comparison of two different collar structured implants supporting 3-unit fixed partial denture: A 3-d fem study.Acta Odontol Scand. 2012; 70(1):61-71. [8]Abrahamsson I,Berglundh T.Tissue characteristics at microthreaded implants: an experimental study in dogs.Clin Impl Dent Rel Res.2006;8(3):107-113. [9]Lee DW,Choi YS,Park KH,et al.Effect of microthread on the maintenance of marginal bone level: A 3‐year prospective study.Clin Oral Impl Res.2007;18(4):465-470. [10]Prasad DK,Shetty M,Bansal N,et al.Crestal bone preservation: A review of different approaches for successful implant therapy. Indian J Dent Res.2011;22(2):317. [11]刘健,葛自力,惠建华,等.骨水平种植体与软组织水平种植体的临床疗效比较[J]. 苏州大学学报:医学版,2012,32(3):414-416. [12]Harder S,Dimaczek B,Açil Y,et al.Molecular leakage at implant-abutment connection—in vitro investigation of tightness of internal conical implant-abutment connections against endotoxin penetration.Clin Oral Invest. 2010;14(4): 427-432. [13]Rack A,Rack T,Stiller M,et al.In vitro synchrotron-based radiography of micro-gap formation at the implant-abutment interface of two-piece dental implants.J Synchrotron Radiat. 2010;17(2):289-294. [14]Weng D,Nagata MJH,Bell M,et al.Influence of microgap location and configuration on the periimplant bone morphology in submerged implants. An experimental study in dogs.ClinOral Impl Res.2008;19(11):1141-1147. [15]高奎英.内外连接对不同直径种植体周围骨组织的应力影响[D].吉林大学,2006.http://www.docin.com/p-333357579.html [16]Mangano C,Mangano F,Piattelli A,et al.Prospective clinical evaluation of 1920 morse taper connection implants: Results after 4 years of functional loading. Clin Oral Impl Res. 2009; 20(3):254-261. [17]Baumgarten H,Cocchetto R,Testori T,et al.A new implant design for crestal bone preservation: Initial observations and case report.Pract Proced Aesthet Dent.2005;17(10):735. [18]Porter SS.Platform switching: A new concept in implant dentistry for controlling postrestorative crestal bone levels. Dent.2006;26:9-17. [19]Calvo‐Guirado JL,Gómez‐Moreno G,López‐Marí L,et al.Crestal bone loss evaluation in osseotite expanded platform implants: A 5‐year study.Clin Oral Impl Res. 2011; 22(12):1409-1414. [20]冯爱菊,王维英,肖菲,等.平台转移设计种植体植入1年后下颌后牙区的骨丧失[J]. 中国组织工程研究,2011,15(22): 4160-4164. [21]Farronato D,Santoro G,Canullo L,et al.Establishment of the epithelial attachment and connective tissue adaptation to implants installed under the concept of “platform switching”: A histologic study in minipigs.Clin Oral ImplRes.2012;23(1):90-94. [22]Çimen H,Yengin E.Analyzing the effects of the platform-switching procedure on stresses in the bone and implant-abutment complex by 3-dimensional fem analysis. J Oral Implantol.2012;38(1):21-26. [23]Renouard F, Nisand D.Impact of implant length and diameter on survival rates. Clinical Oral Implants Research,2006; 17(S2):35-51. [24]Baggi L,Cappelloni I,Di Girolamo M,et al.The influence of implant diameter and length on stress distribution of osseointegrated implants related to crestal bone geometry: A three-dimensional finite element analysis.J Prosthet Dent. 2008;100(6):422-431. [25]Jang HW,Kang JK,Lee K,et al.A retrospective study on related factors affecting the survival rate of dental implants.J Adv Prosthodont.2011;3(4):204-215. [26]Hsu JT,Fuh LJ,Lin DJ,et al.Bone strain and interfacial sliding analyses of platform switching and implant diameter on an immediately loaded implant: Experimental and three-dimensional finite element analyses.JPeriodontol. 2009;80(7):1125-1132. [27]Marincola M,Coelho P,Morgan V,et al.The importance of crestal bone preservation in the use of short implants. J Adv Dent Res VolI: Issue I: October,2010:15. [28]程亚楠,徐普,朱亚丽,等.三种种植系统周边骨质吸收的对比研究[J].临床口腔医学杂志,2011,27(12):742-745. [29]de Carvalho NA,de Almeida EO,Rocha EP,et al.Short implant to support maxillary restorations: Bone stress analysis using regular and switching platform.J Craniofac Surg.2012; 23(3): 678-681. [30]Himmlová L,Dostálová T,Kácovský A,et al.Influence of implant length and diameter on stress distribution: A finite element analysis.J Prosthet Dent.2004;91(1):20-25. [31]Noharet R,Pettersson A,Bourgeois D.Accuracy of implant placement in the posterior maxilla as related to 2 types of surgical guides: A pilot study in the human cadaver.J Prosthet Dent.2014 Apr 7.pii: S0022-3913(14)00087-0. doi: 10.1016/j.prosdent.2013.12.013. [Epub ahead of print] [32]Liang R,Guo W,Qiao X,et al.Biomechanical analysis and comparison of 12 dental implant systems using 3D finite element study.Comput Methods Biomech Biomed Engin. 2014 Apr 8.[Epub ahead of print] [33]Han HJ,Kim S,Han DH.Multifactorial Evaluation of Implant Failure: A 19-year Retrospective Study.Int J Oral Maxillofac Implants.2014;29(2):303-310. [34]Petropoulos VC,Balshi TJ,Wolfinger GJ,et al.Treatment of a Patient with Implant Failure and Jaw Osteonecrosis: Successful Retreatment Using Implants.J Oral Implantol.2014 Mar 25.[Epub ahead of print] [35]Lu Y,Chang S,Wu H,et al.Selection of optimal length and diameter of mini implant in two different forces: a three-dimensional finite element analysis.Hua Xi Kou Qiang Yi Xue Za Zhi.2014;32(1):85-90. [36]Schrott A,Riggi-Heiniger M,Maruo K,et al.Implant loading protocols for partially edentulous patients with extended edentulous sites-a systematic review and meta-analysis.Int J Oral Maxillofac Implants.2014;29 Suppl:239-255. [37]Cundy TP,Cundy WJ,Antoniou G,et al.Serum titanium, niobium and aluminium levels two years following instrumented spinal fusion in children: does implant surface area predict serum metal ion levels?Eur Spine J.2014 Mar 23.[Epub ahead of print] [38]Baba NZ,Goodacre CJ,Kattadiyil MT.Tooth retention through root canal treatment or tooth extraction and implant placement: A prosthodontic perspective.Quintessence Int. 2014;45(5):405-416. [39]González-García R,Monje A,Fernández-Calderón MC,et al.Three-dimensional and chemical changes on the surface of a 3-year clinically retrieved oxidized titanium dental implant.J Mech Behav Biomed Mater.2014;34C:273-282. [40]Al-Hashedi AA,Ali TB,Yunus N.Short dental implants: An emerging concept in implant treatment.uintessence Int. 2014; 45(6):499-514. [41]Nejatidanesh F,Savabi O,Ebrahimi M,et al.Retentive strength of implant-supported base metal copings over short metal abutments using different luting agents and surface treatments. Implant Dent.2014;23(2):162-167. [42]Caruso R,Botta L,Verde A,et al.Relationship between pre-implant interleukin-6 levels, inflammatory response, and early outcome in patients supported by left ventricular assist device: a prospective study.PLoS One.2014;9(3):e90802. [43]王春先,周磊,徐世同,等.Bicon短种植体在上颌后牙区骨量不足病例中的临床应用[J]. 中国口腔种植学杂志,2011,16(1):056. |
| [1] | Huo Hua, Cheng Yuting, Zhou Qian, Qi Yuhan, Wu Chao, Shi Qianhui, Yang Tongjing, Liao Jian, Hong Wei. Effects of drug coating on implant surface on the osseointegration [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3558-3564. |
| [2] |
Zhang Xuan, Li Yunpeng, Zhang Xuejian, Yin Chuanrong, Deng Yue.
Guided bone regeneration using preformed titanium mesh combined with bioabsorbable membranes in aesthetic area [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(26): 4112-4117. |
| [3] | Yuan Bo, Wang Zhiwei, Tang Yifan, Zhou Shengyuan, Chen Xiongsheng, Jia Lianshun. Construction of polycaprolactone-tricalcium phosphate with different mixture ratios using three-dimensional printing technology and its osteoinductivity in vitro [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(6): 821-826. |
| [4] | Liu Dan, Min Changqin, Lu Shuai, Chen Yue, Sun Yong. Osseointegration induced by beta-tricalcium phosphate loaded with advanced platelet-rich fibrin [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(6): 888-893. |
| [5] | Li Fang, Cheng Yuting, Huang Xiaolin, Zhou Qian, Wu Chao, Shi Qianhui, Wang Yong, Liao Jian. Maxillary sinus floor augmentation: with or without bone grafting [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(6): 971-977. |
| [6] | Wei Wei, Liu Yanfei, Zhang Ling, Xiong Na . Self-assembling peptide hydrogel: hemostatic effect and mechanism [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(2): 310-316. |
| [7] | Zou Yingnan, Wang Yibo, Ding Chao, Pan Xinyu, Shi Jiuhui . Three-dimensional finite element analysis of dental implant combined with residual tooth after hemisection under dynamic loads [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(2): 178-183. |
| [8] | Wang Liping, Chen Weihong, Zha Jun, Chen Xili, Su Yucheng, Fang Ying, Dong Yu, Guo Xueqi, Ge Linhu. Short-term efficacy evaluation of Mis Seven implant system repairing dentition loss [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(14): 2208-2214. |
| [9] | Li Ying, You Yapeng, Li Baoe, Song Yunjia, Ma Aobo, Chen Bo, Han Wen, Li Changyi. Type I collagen combined titanium dioxide nanotube composite coating modified titanium surface improves osteoblast adhesion and osseointegration [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(14): 2169-2176. |
| [10] | Zhang Minbo, Peng Qifeng, Ma Yaping, Kong Weijun, Liao Wenbo. Physical properties and biocompatibility of 3D printed bone microparticle/poly(lactic-co-glycolic acid) scaffold [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(14): 2215-2222. |
| [11] | Li Zhi, Tan Chunhua, Cai Xianhua, Wang Huasong, Ding Xiaoming, Zhao Yanhong. Fabrication and biocompatibility assessment of the scaffold with biomimetic interconnected macropore structure [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(14): 2223-2227. |
| [12] | Bai Yulong, Gao Yufeng, Zhong Hongbin, Zhao Yantao, Guo Ruizhou, Li Li. Allogeneic and xenogeneic tissue repair materials: how to choose a suitable virus inactivation process [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(14): 2261-2268. |
| [13] | Luo Kai, Yang Yafeng, Ma Teng, Xia Bing, Huang Liangliang, Huang Jinghui, Luo Zhuojing. Effects of perfluorotributylamine/alginate/bioglass biomaterials on viability and osteogenic differentiation of adipose-derived stem cells [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(13): 1995-2001. |
| [14] | Wang Yuanyuan, Song Wenshan, Yu Dejun, Dai Yuankun, Li Bafang. Preparation and evaluation of fish skin acellular dermal matrix for oral guided tissue regeneration [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(10): 1526-1532. |
| [15] | Liu Shaoyang, Zou Hanlin . Biocompatibility of anodic titanium oxide: an experimental research [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(10): 1575-1580. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||