Chinese Journal of Tissue Engineering Research ›› 2013, Vol. 17 ›› Issue (5): 920-930.doi: 10.3969/j.issn.2095-4344.2013.05.024
Previous Articles Next Articles
Off-pump coronary artery bypass grafting treats high-risk coronary heart disease
Wang Shi-xiong1, 2, Li Ning-yin1, 2, Zhao Qi-ming1, Gao Bing-ren1
- 1 Second Hospital of Lanzhou University, Lanzhou 73000, Gansu Province, China
2 Second Clinical Medical College of Lanzhou University, Lanzhou 73000, Gansu Province, Chi
-
Received:2012-07-16Revised:2012-09-05Online:2013-01-29Published:2013-01-29 -
Contact:Wang Shi-xiong★, Studying for master’s degree, Second Hospital of Lanzhou University, Lanzhou 73000, Gansu Province, China; Second Clinical Medical College of Lanzhou University, Lanzhou 73000, Gansu Province, China wangshi0815@163.com -
About author:Wang Shi-xiong★, Studying for master’s degree, Second Hospital of Lanzhou University, Lanzhou 73000, Gansu Province, China; Second Clinical Medical College of Lanzhou University, Lanzhou 73000, Gansu Province, China wangshi0815@163.com
CLC Number:
Cite this article
Wang Shi-xiong, Li Ning-yin, Zhao Qi-ming, Gao Bing-ren. Off-pump coronary artery bypass grafting treats high-risk coronary heart disease[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(5): 920-930.
share this article
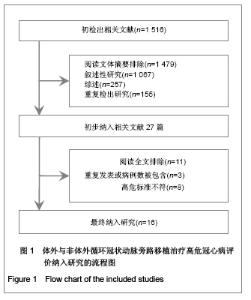
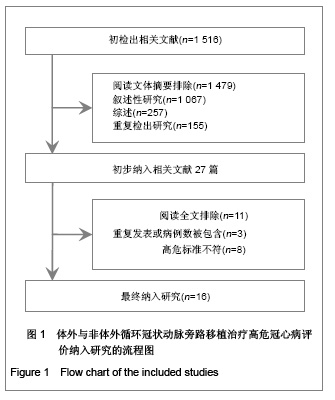
2.1 检索结果分析 根据检索策略和资料收集方法,初检出文献1516篇,去除重复文献155篇,初筛通过阅读题目和摘要,排除主题与本研究不符的文献1324篇,对初筛后的27篇文献仔细阅读全文,进一步排除受试对象与重复发表的文献11篇,最终纳入16个研究[17-32],共6441例患者,流程图见图1)。"
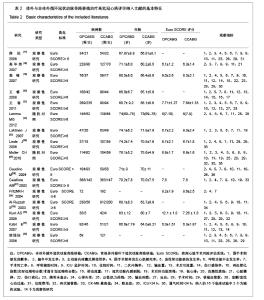
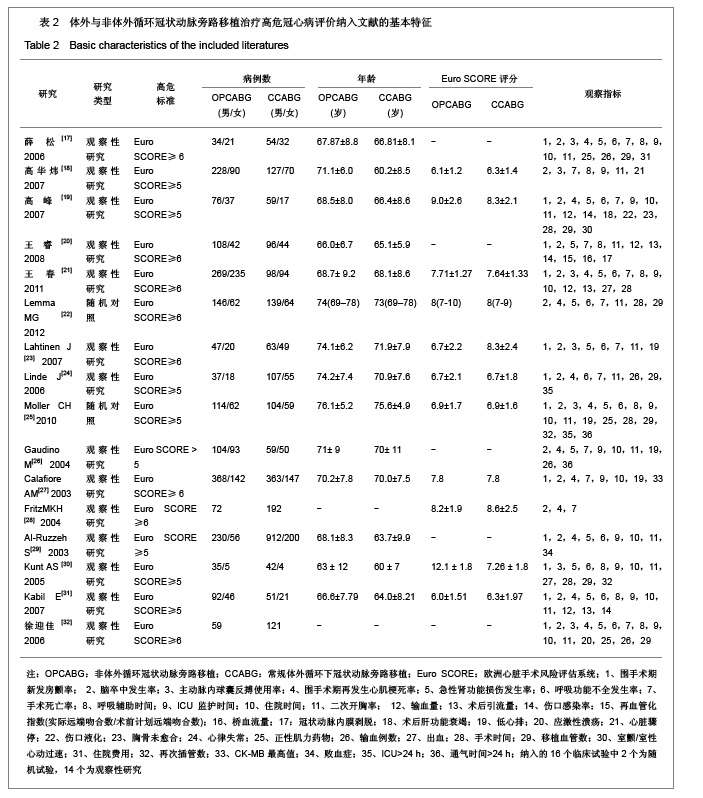
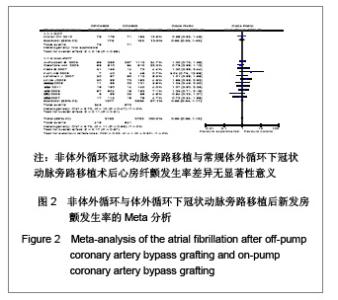
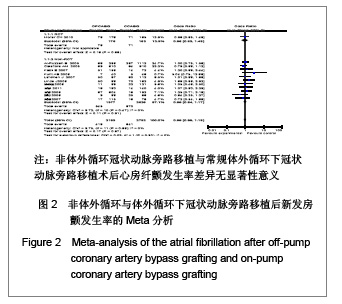
2.2 纳入研究的基本特征 本研究共纳入16个临床试验[17-32],其中2个为随机试验[22, 25],14个为观察性研究[17-21,23-24,26-32],观察性研究均为高质量的(得分≥6)。见表2。 2.3 Meta分析结果 2.3.1 安全性评价结果比较 术后新发房颤率,脑卒中率,主动脉内球囊反搏使用率,围手术期心肌梗死发生率,术后急性肾功能损伤率,术后呼吸功能不全,伤口感染率。 术后新发房颤发生率:共12个研究报道了术后新发房颤率[17,19-21,23-25,27,29-32],其中有1个随机对照试验[25],11个非随机对照试验[17,19-21,23-24,27,29-32],OPCABG组共纳入2153例患者,心房纤颤总发生率为19.4%;CCABG组共2792例,AF总发生率为23.0%。各研究间无统计学异质性(I2=0%,P=0.55),故采用固定效应模型合并效应量。研究数据设计亚组Meta分析结果显示:随机对照试验亚组两组差异无显著性意义[OR=0.96, 95%CI (0.63,1.48),P=0.86]; 非随机对照试验亚组两组差异无显著性意义[OR=0.99,95%CI (0.84,1.77),P=0.91]。合并分析显示两组差异亦无显著性意义[OR=0.99,95%CI(0.85,1.15),P=0.87],见图2,故认为OPCABG与CCABG术后心房纤颤发生率差异无显著性意义。"
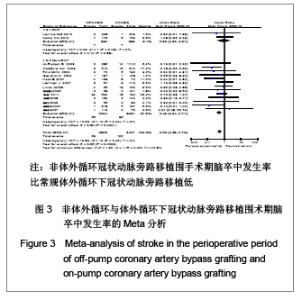
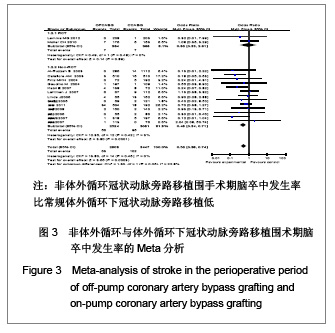
脑卒中发生率:共15个研究报道了围手术期脑卒中发生率[17-29, 31-32],其中有2个随机对照试验[22, 25],13个非随机对照试验[17-21,23-24,26-29,31-32]。OPCABG组共纳入2908例患者,脑卒中总发生率2.2%;CCABG组共纳入3 447例患者,脑卒中总发生率3.0%。各研究间无统计学异质性(I2=0%,P=0.48),故采用固定效应模型合并效应量。研究数据设计亚组分析结果显示:随机对照试验两组差异无显著性意义[OR=0.93,95%CI(0.33,2.61),P=0.89];非随机对照试验亚组两组比较差异有显著性意义[OR=0.49,95%CI (0.34,0.71), P=0.000 1]。合并分析显示两组比较差异有显著性意义[OR=0.53,95%CI(0.38,0.74),P=0.000 3],见图3,故认为OPCABG围手术期脑卒中发生率比CCABG低。"
"
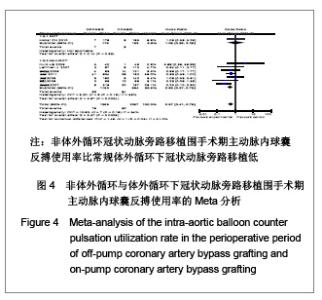
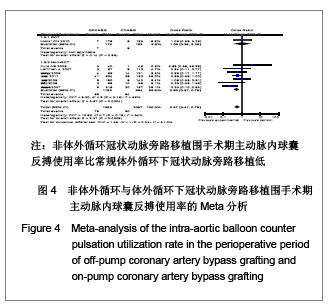
主动脉内球囊反搏使用率:共8个研究报道了主动脉内球囊反搏使用率[17-18,20-21,23,25,30,32],其中有1个随机对照试验[25],7个非随机对照试验[17-18, 20-21,23 ,30,32],OPCAB组共纳入1369例患者,主动脉内球囊反搏总使用率为5.6%;CCABG组共1 057例,主动脉内球囊反搏总使用率8.5%。各研究间无统计学异质性(I2=34%,P=0.16),故采用固定效应模型合并效应量。研究数据设计亚组分析结果显示:随机对照试验两组差异无显著性意义[OR=1.08,95%CI(0.36,3.29),P=0.89];非随机对照试验亚组两组差异有显著性意义[OR=0.53,95%CI(0.37,0.75),P=0.000 4]。合并分析显示两组差异有显著性意义[OR=0.57,95%CI(0.41,0.79),P=0.000 8],见图4,故认为OPCAB围手术期主动脉内球囊反搏使用率比CCABG低。"
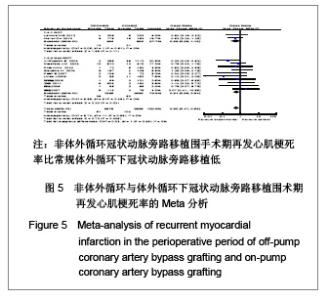
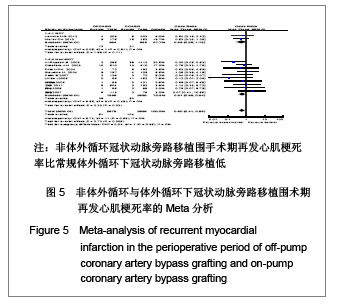
再发心肌梗死率:共12个研究报道了围手术期再发心肌梗死率[17,19,21,22,25-29,31-32],其中有2个随机对照试验[22,25],10个非随机对照试验[17,19,21 ,26-29,31-32]。OPCAB组共纳入2373例患者,总发生率2.1%;CCABG组纳入2 998例患者,总发生率3.5%。各研究间无统计学异质性(I2=0%,P=0.65),故采用固定效应模型合并效应量。研究数据设计亚组分析结果显示:随机对照试验两组差异无显著性意义[OR=0.56,95%CI(0.28,1.15),P=0.11];非随机对照试验亚组两组差异有显著性意义[OR=0.61,95%CI(0.39,0.94),P=0.03]。合并分析显示两组差异有显著性意义[OR=0.58,95%CI (0.41,0.86),P=0.006],见图5,故认为OPCABG围手术期再发心肌梗死率比CCABG低。"
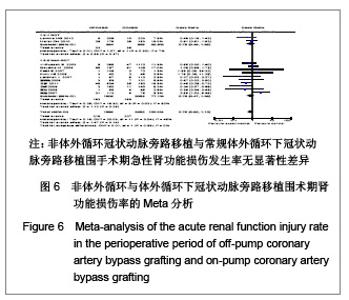
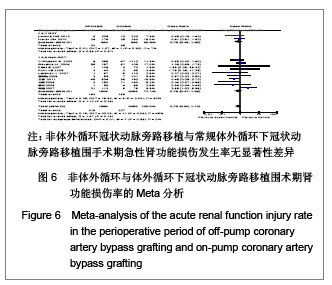
术后急性肾功能损伤率:共12个研究报道了急性肾功能损伤[17,19-23,25,26,29-32],其中有2个随机对照试验[22,25],10个非随机对照试验[17,19-21,23, 26,29-32],OPCABG组共纳入1993例患者,总发生率10.8%;CCABG组共2 432例,总发生率8.5%。各研究间有统计学异质性(I2=45%,P=0.04),分析异质性的来源,进行亚组分析。随机对照试验亚组的各研究间无统计学异质性(I2=7%,P=0.30),故采用固定效应模型合并效应量,Meta分析两组间差异无显著性意义[OR=0.78,95%CI(0.45,1.35),P=0.37]。非随机对照试验亚组的各研究间有统计学异质性(I2=52%,P=0.03),故采用随机效应模型合并效应量。Meta分析两组间差异无显著性意义[OR=0.76,95%CI (0.47,1.23),P=0.26],见图6。故认为OPCABG与CCABG围手术期急性肾功能损伤发生率差异无显著性意义。"
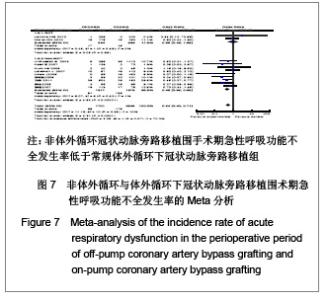
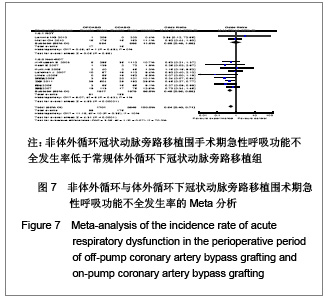
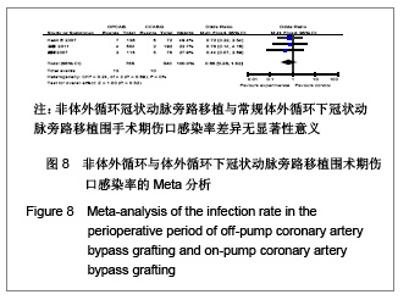
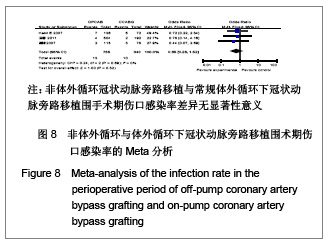
呼吸功能不全发生率:共11个研究报道了呼吸功能不全发生率[17,19,21-25, 29-32],其中有2个随机对照试验[22,25],9个非随机对照试验[17,19,21,23-24,29-32]。OPCAB组共纳入1701例患者,总发生率5.8%;CCABG组共2345例,总发生率7.5%。各研究间无统计学异质性(I2=2%,P=0.42),故采用固定效应模型合并效应量。研究数据设计亚组分析结果显示:随机对照试验两组差异无显著性意义[OR=0.98,95%CI(0.49,1.99),P=0.98];非随机对照试验亚组两组差异有显著性意义[OR=0.48,95%CI(0.35,0.65),P < 0.000 01]。合并分析显示两组差异有显著性意义[OR=0.54,95%CI(0.40,0.71),P < 0.000 1],见图7,故认为OPCABG围手术期急性呼吸功能不全发生率低于CCABG组。 伤口感染率:共3个研究报道了伤口感染率[19,20,31],都为非随机对照试验。OPCABG组共纳入755例患者,CCABG组共340例。各研究间无统计学异质性(I2=0%,P=0.89),故采用固定效应模型合并效应量。Meta分析结果显示两组差异有显著性意义[OR=0.65,95%CI(0.28,1.52),P=0.32],见图8,故认为OPCABG与CCABG围手术期伤口感染率差异无显著性意义。"
"
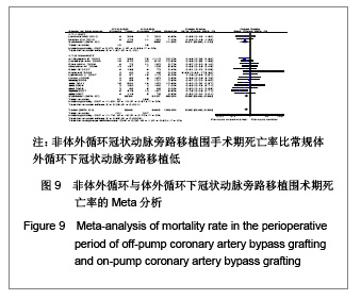
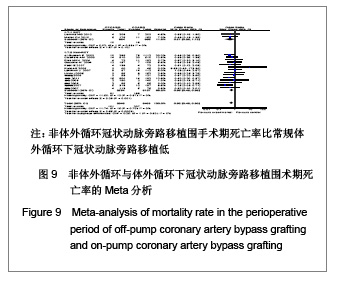
2.3.2 有效性评价结果比较 围手术期死亡率,呼吸机辅助呼吸时间,ICU时间,住院时间,二次开胸率,术后引流量,输血量。 死亡率:共16个研究报道了死亡率[17-32]。其中有2个随机对照试验[22, 25],14个非随机对照试验[17-21,23-24,26-32],OPCAB组共纳入2 948例患者,总发生率3.4%;CCABG组共纳入3493例患者,总发生率5.4%。各研究间无统计学异质性(I2=0%,P=0.79),故采用固定效应模型合并效应量。研究数据设计亚组分析结果显示:随机对照试验两组差异无显著性意义 [OR=0.51,95%CI(0.23,1.12),P=0.10];非随机对照试验亚组两组差异有显著性意义[OR=0.62,95%CI (0.48,0.83),P=0.001]。合并分析显示两组差异有显著性意义[OR=0.62,95%CI(0.48,0.80),P=0.000 3],见图9,故认为OPCABG围手术期死亡率比CCABG低。"
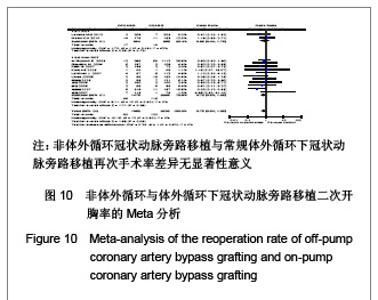
二次开胸率:共13个研究报道了二次开胸率[17-20,22-26,29-32]。其中有2个随机对照试验[22,25],11个非随机对照试验[17-20,23-24,26,29-32]。OPCAB组共纳入1862例患者,CCABG组共纳入2599例患者。各研究间无统计学异质性(I2=0%,P=0.80),故采用固定效应模型合并效应量。研究数据设计亚组分析结果显示:随机对照试验两组差异无显著性意义[OR=0.88,95%CI (0.44,1.75),P=0.72];非随机对照试验亚组两组差异无显著性意义[OR=0.72,95%CI(0.50,1.05),P=0.09]。合并分析显示两组差异无显著性意义[OR=0.75,95%CI (0.50,1.05),P=0.09],见图10,故认为OPCAB与CCABG再次手术率差异无显著性意义。"

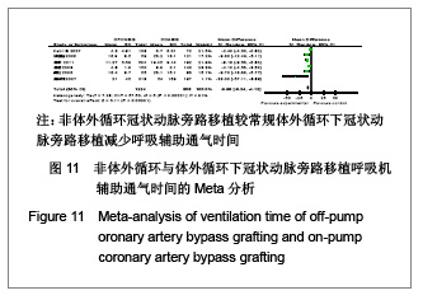
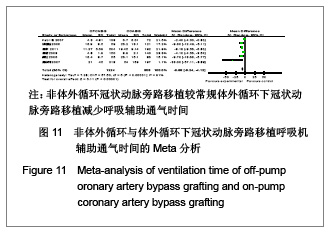
呼吸机辅助时间:共8个研究报道了呼吸机辅助时间(h)[17-18,20-21,25,30-32],其中1个采用了中位数计算[25], 1个采用min计算[30],最后纳入6个研究进行Meta分析[17-18, 20-21 ,31, 32],均为非随机对照试验。OPCABG组共纳入1224例患者,CABG组共808例。各研究间有统计学异质性(I2=91%,P < 0.000 01),分析异质性的来源,可能与各研究者之间拔除呼吸机时限没有统一标准及监护室条件不一。故采用随机效应模型合并效应量。Meta分析结果显示两组差异有显著性意义[WMD=-6.65,95%CI(-9.24,-4.12),P < 0.000 01],见图11。因此认为OPCABG较CCABG减少呼吸辅助通气时间。"
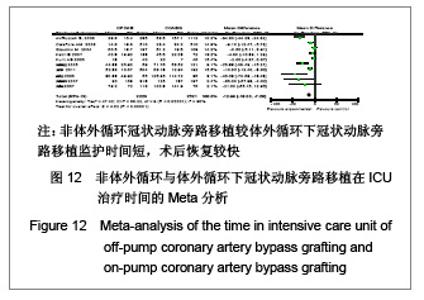
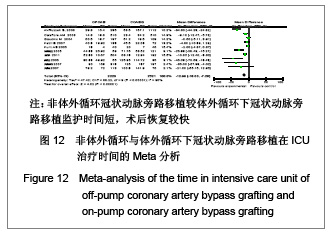
ICU治疗时间:共10个研究报道了在ICU治疗时间 (h)[17-19,21,26-27,29-32],均为非随机对照试验。OPCABG组共纳入2220例患者,CCABG组共2521例。各研究间有统计学异质性(I2=90%,P < 0.000 01),分析异质性的来源,可能与各研究者的监护室条件不一致有关。故采用随机效应模型合并效应量。Meta分析结果显示两组差异有显著性意义[WMD=-12.66,95%CI(-18.03, -7.92),P < 0.000 01],见图12,故认为OPCABG较CCABG监护时间短,术后恢复较快。"

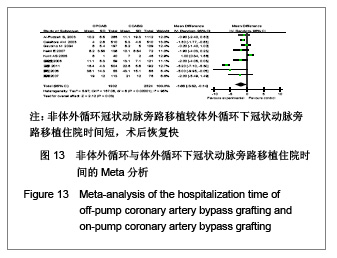
住院时间:共10个研究报道了住院时间[17,19,21,25-27,29-32],其中1个研究采用中位数计算[25],故纳入9个研究进行Meta分析[17,19,21,26-27,29-32],均为非随机对照试验。OPCABG组共纳入1 902例患者,CCABG组共2 324例。各研究间有统计学异质性(I2=90%,P <0.000 01)。故采用随机效应模型合并效应量。Meta分析结果显示两组差异有显著性意义[WMD=-1.88,95%CI(-3.62,-0. 14),P < 0.000 01],见图13,说明OPCABG较CCABG住院时间短,术后恢复快。"
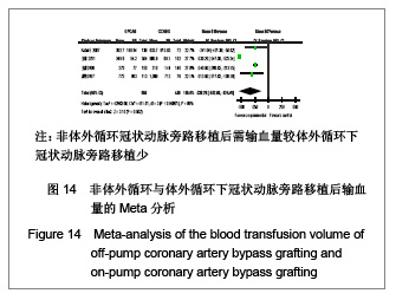
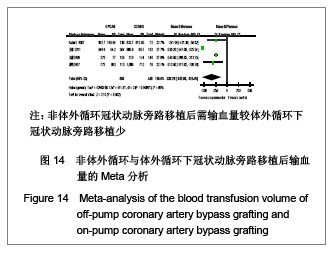
输血量:共4个研究报道了平均输血量[19-21,31],均为非随机对照试验。OPCABG组共纳入905例患者,CCABG组共480例。各研究间有统计学异质性(I2=99%,P < 0.000 01)。故采用随机效应模型合并效应量。Meta分析结果显示两组差异有显著性意义[WMD=-338.28,95%CI(-552.08,-124. 48),P=0.002],见图14,说明OPCABG术后需输血量较CCABG少。"
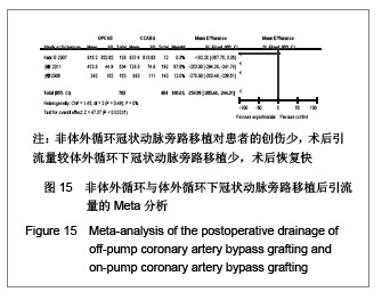
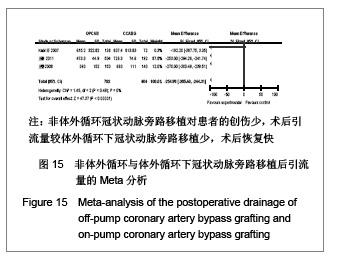
引流量:共3个研究报道了术后应流量[20-21,31],均为非随机对照试验。OPCAB组共纳入792例患者,CCABG组共404例。各研究间无统计学异质性(I2=0%,P=0.49)。故采用固定效应模型合并效应量。Meta分析结果显示两组差异有显著性意义[WMD=-254.86,95%CI(-265.40, -224. 31),P < 0.000 01],因为说明OPCABG对患者的创伤少,术后引流量较CCABG少,术后恢复快。见图15。"
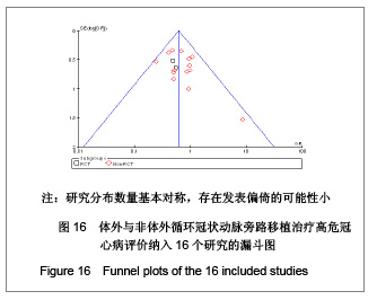
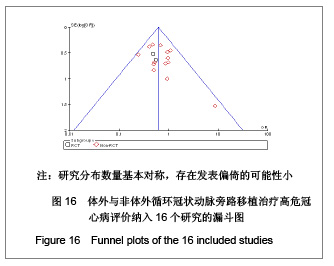
2.4 发表偏倚 文章纳入16个研究,漏斗图显示16个研究分布数量基本对称,发表偏倚的可能性小,见图16"
| [1] Edmunds LH Jr. Inflammatory response to cardiopulmonary bypass.Ann Thorac Surg. 1998/12/30 ed; 1998:S12-6; discussion S25-8.[2] Taylor KM. Brain damage during cardiopulmonary bypass. Ann Thorac Surg.1998;65(4 Suppl):S20-6; discussion S7-8.[3] Royster RL. Myocardial dysfunction following cardiopulmonary bypass: recovery patterns, predictors of inotropic need, theoretical concepts of inotropic administration. J Cardiothorac Vasc Anesth. 1993;(4 Suppl 2):19-25.[4] Cislaghi F,Condemi AM,Corona A.Predictors of prolonged mechanical ventilation in a cohort of 5123 cardiac surgical patients. Eur J Anaesthesiol. 2009;26(5):396-403.[5] Chen YB, Shu J, Yang WT,et al. Meta-analysis of randomized trials comparing the effectiveness of on-pump and off-pump coronary artery bypass. Chin Med J (Engl). 2012;125(2): 338-344.[6] Biancari F, Mahar MA. Meta-analysis of randomized trials on the efficacy of posterior pericardiotomy in preventing atrial fibrillation after coronary artery bypass surgery. J Thorac Cardiovasc Surg. 2010;139(5):1158-1161.[7] Bainbridge D, Martin J, Cheng D. Off pump coronary artery bypass graft surgery versus conventional coronary artery bypass graft surgery: a systematic review of the literature. Semin Cardiothorac Vasc Anesth. 2005;9(1): 105-111.[8] Nigwekar SU, Kandula P, Hix JK,et al. Off-pump coronary artery bypass surgery and acute kidney injury: a meta-analysis of randomized and observational studies. Am J Kidney Dis. 2009;54(3):413-423.[9] Edelman JJ, Yan TD, Padang R,et al. Off-pump coronary artery bypass surgery versus percutaneous coronary intervention: a meta-analysis of randomized and nonrandomized studies. Ann Thorac Surg. 2010;90(4):1384-1390.[10] Afilalo J, Rasti M, Ohayon SM,et al. Off-pump vs. on-pump coronary artery bypass surgery: an updated meta-analysis and meta-regression of randomized trials. Eur Heart J. 2011;33(10):1257-1267.[11] Nashef SA, Roques F, Michel P,et al. European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg. 1999;16(1):9-13.[12] Higgins J, Thompson SG, Deeks JJ,et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557.[13] Stroup DF, Berlin JA, Morton SC,et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012.[14] Panesar SS, Athanasiou T, Nair S,et al. Early outcomes in the elderly: a meta-analysis of 4921 patients undergoing coronary artery bypass grafting--comparison between off-pump and on-pump techniques. Heart.2006;92(12):1808-1816.[15] Athanasiou T, Al-Ruzzeh S,Kumar P,et al.Off-pump myocardial revascularization is associated with less incidence of stroke in elderly patients. Ann Thorac Surg. 2004;77(2):745-753.[16] Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. The Cochrane Collaboration. 2011.[17] 薛松, 黄日太, 申达浦,等. 心脏停跳与不停跳冠状动脉旁路移植术在高危病人中应用的比较[J]. 中华胸心血管外科杂志, 2006, 22(5):2.[18] 高华炜, 郑哲, 胡盛寿. 高危患者行非体外循环与体外循环冠状动脉旁路移植术早期临床结果的对比分析[J].中华心血管病杂志,2007,35(3):3.[19] 高峰, 杨碧波, 高文德,等. 高风险患者非体外循环冠状动脉旁路移植[J].中国微创外科杂志,2007,7(3):267-270.[20] 王睿, 陈鑫, 石开虎,等. 高风险冠心病患者接受体外或非体外循环冠状动脉旁路移植术的临床对比研究[J]. 中国微创外科杂志,2008,14(7):3.[21] 王春, 谷天祥, 于洋,等. 非体外循环不停跳冠状动脉旁路移植术在高危冠心病治疗中的作用[J]. 中国动脉硬化杂志,2011, (06):517-20.[22] Lemma MG, Coscioni E, Tritto FP,et al. On-pump versus off-pump coronary artery bypass surgery in high-risk patients: operative results of a prospective randomized trial (on-off study). J Thorac Cardiovasc Surg. 2012;143(3):625-631.[23] Lahtinen J, Biancari F, Rimpilainen J,et al. Off-pump versus on-pump coronary artery bypass surgery in high-risk patients (EuroSCORE >/= 6). Thorac Cardiovasc Surg. 2007;55(1): 13-18.[24] Linde J, Moller C, Hughes P, Steinbruchel D. Off-pump versus on-pump CABG in high-risk patients: short- and mid-term outcome. Scand Cardiovasc J.2006;40(4):209-213.[25] Moller CH, Perko MJ, Lund JT,et al. No major differences in 30-day outcomes in high-risk patients randomized to off-pump versus on-pump coronary bypass surgery: the best bypass surgery trial. Circulation. 2010;121(4):498-504.[26] Gaudino M, Glieca F, Alessandrini F,et al. High risk coronary artery bypass patient: incidence, surgical strategies, and results. Ann Thorac Surg.2004;77(2):574-579; discussion 80.[27] Calafiore AM, Di Mauro M, Canosa C,et al. Early and late outcome of myocardial revascularization with and without cardiopulmonary bypass in high risk patients (EuroSCORE > or = 6). Eur J Cardiothorac Surg. 2003;23(3):360-367.[28] Fritz MKH, Wiebalck A, Khargi K,et al. Does off-pump coronary artery bypass surgery reduce morbidity and mortality in high-risk patients? European Surgery - Acta Chirurgica Austriaca. 2004;36(6):363-367.[29] Al-Ruzzeh S, Nakamura K, Athanasiou T,et al. Does off-pump coronary artery bypass (OPCAB) surgery improve the outcome in high-risk patients?: a comparative study of 1398 high-risk patients. Eur J Cardiothorac Surg. 2003;23(1):50-55.[30] Kunt AS, Darcin OT, Andac MH. Coronary artery bypass surgery in high-risk patients. Curr Control Trials Cardiovasc Med. 2005;6:13.[31] Kabil E, Mujanovic E, Bergsland J. A comparation of coronary artery bypass grafting with and without cardiopulmonary bypass in EuroSCORE high risk patients. Bosn J Basic Med Sci. 2007;7(1):48-51.[32] 徐迎佳, Yongseng T, Yeowleng C. 180例高危病例的冠状动脉搭桥术——停跳与不停跳手术的比较[J]. 国际心血管病杂志, 2006,33(4):3.[33] Goetz R,Rohman M, Haller J,et al. Internal mammary-coronary artery anastomosis. A nonsuture method employing tantalum rings. J Thorac Cardiovasc Surg. 1961; 41:378-386[34] Serruys PW, Morice MC, Kappetein AP,et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360 (10): 961-972.[35] Wijeysundera DN, Beattie WS, Djaiani G,et al. Off-pump coronary artery surgery for reducing mortality and morbidity: meta-analysis of randomized and observational studies. J Am Coll Cardiol. 2005;46(5):872-882.[36] 宋铁牛, 赵启明, 戴玉雷,等. 体外与非体外循环冠状动脉旁路移植术再血管化率的系统评价[J].现代生物医学进展,2011, 11(1):105-107.[37] Takagi H, Matsui M, Umemoto T. Off-pump coronary artery bypass may increase late mortality: a meta-analysis of randomized trials. The Annals of thoracic surgery.2010;(6): 1881-1888.[38] 姜大庆, 谷天祥, 王海龙, 等. 老年患者非体外和体外循环冠状动脉旁路移植术围术期脑卒中发生率比较的系统评价和Meta分析[J]. 中国胸心血管外科临床杂志,2011,18(4):289-300.[39] Vasques F, Rainio A, Heikkinen J,et al. Off-pump versus on-pump coronary artery bypass surgery in patients aged 80 years and older: institutional results and meta-analysis. Heart Vessels. 2011 Nov 9.[40] Hart JC. A review of 140 Octopus off-pump bypass patients over the age of seventy: procedure of choice.Heart Surg Forum. 2001;4 Suppl 1:S24-29.[41] 崔虎军, 肖峰, 李岩,等.心脏手术风险评估欧洲系统(EuroSCORE)的初步临床应用[J]. 中国心血管病研究杂志, 2006,4(1):4.[42] Parolari A, Pesce LL, Trezzi M,et al. EuroSCORE performance in valve surgery: a meta-analysis. Ann Thorac Surg. 2010;89(3):787-93, 793.e1-2. |
| [1] | Zhang Yu, Tian Shaoqi, Zeng Guobo, Hu Chuan. Risk factors for myocardial infarction following primary total joint arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1340-1345. |
| [2] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [3] | Chen Jinping, Li Kui, Chen Qian, Guo Haoran, Zhang Yingbo, Wei Peng. Meta-analysis of the efficacy and safety of tranexamic acid in open spinal surgery [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1458-1464. |
| [4] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [5] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [6] | Wang Yongsheng, Wu Yang, Li Yanchun. Effect of acute high-intensity exercise on appetite hormones in adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1305-1312. |
| [7] | Kong Desheng, He Jingjing, Feng Baofeng, Guo Ruiyun, Asiamah Ernest Amponsah, Lü Fei, Zhang Shuhan, Zhang Xiaolin, Ma Jun, Cui Huixian. Efficacy of mesenchymal stem cells in the spinal cord injury of large animal models: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1142-1148. |
| [8] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Intravenous, topical tranexamic acid alone or their combination in total knee arthroplasty: a meta-analysis of randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 948-956. |
| [9] | Li Yan, Wang Pei, Deng Donghuan, Yan Wei, Li Lei, Jiang Hongjiang. Electroacupuncture for pain control after total knee arthroplasty: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 957-963. |
| [10] | He Xiangzhong, Chen Haiyun, Liu Jun, Lü Yang, Pan Jianke, Yang Wenbin, He Jingwen, Huang Junhan. Platelet-rich plasma combined with microfracture versus microfracture in the treatment of knee cartilage lesions: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 964-969. |
| [11] | Hua Haotian, Zhao Wenyu, Zhang Lei, Bai Wenbo, Wang Xinwei. Meta-analysis of clinical efficacy and safety of antibiotic artificial bone in the treatment of chronic osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 970-976. |
| [12] | Zhan Fangbiao, Cheng Jun, Zou Xinsen, Long Jie, Xie Lizhong, Deng Qianrong. Intraoperative intravenous application of tranexamic acid reduces perioperative bleeding in multilevel posterior spinal surgery: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 977-984. |
| [13] | Zhang Wenwen, Jin Songfeng, Zhao Guoliang, Gong Lihong. Mechanism by which Wenban Decoction reduces homocysteine-induced apoptosis of myocardial microvascular endothelial cells in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 723-728. |
| [14] | Nie Huijuan, Huang Zhichun. The role of Hedgehog signaling pathway in transforming growth factor beta1-induced myofibroblast transdifferentiation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 754-760. |
| [15] | Yang Xin, Jin Zhe, Feng Xu, Lu Bing. The current situation of knowledge and attitudes towards organ, eye tissue, body donation of residents in Shenyang [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 779-784. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||