Chinese Journal of Tissue Engineering Research ›› 2013, Vol. 17 ›› Issue (4): 688-695.doi: 10.3969/j.issn.2095-4344.2013.04.020
Previous Articles Next Articles
Locking plate for the treatment of 3-part and 4-part fracture of proximal humerus
He Xiao-jian, Zhuang Jian, Zhou Kai-hua, Chen Ming-ji, Gao Ru-feng, Zheng Fen, Pan Fu-gen
- Department of Orthopedics, Qingpu Branch of Zhongshan Hospital, Fudan University, Shanghai 201700, China
-
Received:2012-09-18Revised:2012-11-27Online:2013-01-22Published:2013-01-22 -
Contact:Pan Fu-gen, Chief physician, Department of Orthopedics, Qingpu Branch of Zhongshan Hospital, Fudan University, Shanghai 201700, China fugenpan@yahoo.cn -
About author:He Xiao-jian★, Master, Attending physician, Department of Orthopedics, Qingpu Branch of Zhongshan Hospital, Fudan University, Shanghai 201700, China hexiaojian1@126.com
CLC Number:
Cite this article
He Xiao-jian, Zhuang Jian, Zhou Kai-hua, Chen Ming-ji, Gao Ru-feng, Zheng Fen, Pan Fu-gen. Locking plate for the treatment of 3-part and 4-part fracture of proximal humerus[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(4): 688-695.
share this article

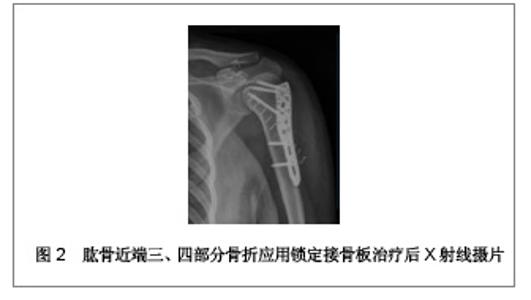
2.1 锁定接骨板治疗肱骨近端三、四部分骨折的临床病例 复旦大学附属中山医院青浦分院骨科2008年1月至2009年12月行锁定接骨板内固定治疗31例肱骨近端骨折患者,男13例,女18例;年龄28-81岁,平均56.4岁。致伤原因:摔伤19例,交通伤7例,坠落伤5例。损伤侧别:左侧14例,右侧17例。3例合并肩关节脱位。6例合并其他部位骨折。术前均行CT及三维重建检查,骨折类型采用Neer分类:三部分骨折19例,四部分骨折12例。受伤至手术时间2-9 d,平均5 d。 2.2 治疗方法 患者取沙滩椅位,全身麻醉后,取胸大肌三角肌间隙入路,注意保护头静脉,充分显露肱骨近端,一般不切开关节囊,少剥离骨折块的骨膜,以肱二头肌长头腱及结节间沟为标志,采用间接复位法将肱骨大小结节骨折块复位。以1.5 mm克氏针临时固定,C臂机监视骨折复位后将解剖锁定接骨板近端置于大结节顶点下方5 mm,结节间沟后方约5 mm处,远端置于三角肌止点。先于远折端以1枚普通皮质骨将钢板固定于肱骨,C臂机下再次确认骨折复位情况及钢板位置,满意后将远近端锁定钢板螺钉固定,近端锁钉长度距软骨下5 mm为宜。结节部骨折块可用可吸收缝线缝合固定于钢板近端的小孔上。拔除克氏针,透视机下再次检查骨折复位情况以及钢板位置,逐层关闭伤口。 术后常规放置引流以及应用抗生素,老年患者予以抗骨质疏松治疗。术后3 d开始肩肘关节被动外展和上举功能锻炼。术后6周、3,6,12个月X射线摄片随访。观察骨折愈合情况,按照Constant评分记录肩关节功能。典型病例X射线摄片见图1,2。"

"

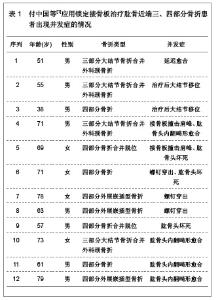
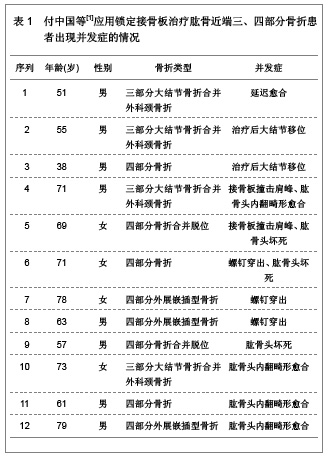
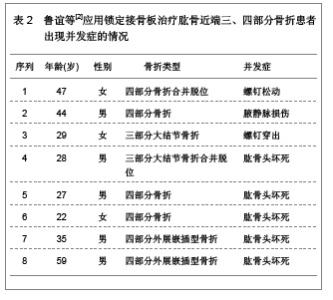
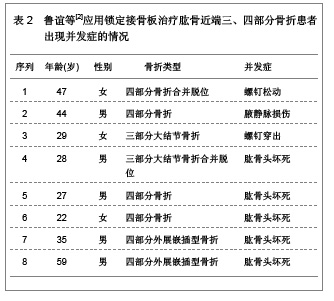
2.3 治疗结果 31例患者均得到13-49个月随访,平均随访19.8个月。骨折均愈合,无内固定失效,临床愈合时间为8-16周。根据Constant评分标准评定肩关节功能:优11例,良16例,可3例,差1例。所有患者均未见螺钉松脱、穿出、断裂等情况,也未见肱骨头坏死、骨不连等相关并发症发生。 2.4 临床应用体会 肱骨近端骨折发生率约占全身骨折的5%[14],好发于骨质疏松的老年患者。在所有老年人骨折发病率中位列第3。其治疗目标和其它关节内骨折一致:尽可能解剖复位恢复关节面的平整、固定牢靠利于肩关节早期进行功能锻炼。但由于肱骨近端三、四部分骨折较难复位,软组织剥离过多容易缺血坏死或骨不连,加上老年患者骨量丢失内固定失效的发生概率较高,预后较差,是创伤骨科的难点[15]。以往对于此类骨折一般采用肩关节假体置换。但上肢对灵活性的要求较高,使假体置换并不像在下肢中那样成功[16]。 解剖型肱骨近端锁定钢板在临床中应用的特点,使手术治疗肱骨近端骨折的并发症有所下降。文献报道,所有三部分骨折及不伴有肩关节脱位的四部分骨折患者均可采用内固定治疗,而无需置换关节[17]。文章研究结果也表明,应用锁定钢板治疗肱骨近端三、四部分骨折,疗效满意,术后并发症低,未见螺钉松脱、穿出、断裂等情况,也未见肱骨头坏死、骨不连等并发症发生。与早期钢板相比,PHOLOS钢板具有成角稳定性,抗拔出能力强,螺钉锁定不会退出,不易松动。但是随着锁定钢板的广泛的应用,内固定失效的报告也引起人们的关注。研究认为提高疗效、减少内固定失效主要应该注意以下几方面。 骨折复位:在肱骨近端骨折内固定失效的患者中,肱骨头内翻移位、螺钉切出较为常见。与骨折复位不良、肱骨外科颈内侧皮质粉碎失去支撑有关,肱骨头颈内下方力学特性与股骨距相似,发生骨折时此处由于肱二头肌长头腱阻挡,能量得以部分吸收,骨折片相对外侧完整。内侧能否重建稳定的支撑直接影响内固定的稳定,故复位时应遵循由内而外的原则,首先复位内侧骨块,当内侧有良好的骨质接触后,再复位外侧骨块,肱骨大结节骨块可留待最后复位。 钢板螺钉的放置:据文献报道,钢板放置过高会引起肩峰撞击,放置偏前则易压迫或磨损肱二头肌长头腱。螺钉太短,不能完全固定骨折块,容易松动脱钉,螺钉太长则穿破肱骨头关节面,减少此类并发症的发生是治疗成功的关键。钢板应放置在肱骨大结节顶点下5 mm,结节间沟后缘5-10 mm处较为稳妥。螺钉则以达到关节软骨下骨下5 mm为佳。术中应多角度透视确认螺钉没有穿出。此外,由于肱骨颈内侧结构的重要性,应至少有2枚螺钉固定此处骨质,起到加强和支撑作用。 软组织保护:对于肱骨近端三、四部分骨折,肱骨头缺血坏死仍是影响疗效的重要因素[18],文献报道,四部分骨折肱骨头坏死率可达37%。文章复旦大学附属中山医院青浦分院骨科锁定接骨板内固定治疗31例患者中,四部分骨折12例,无1例坏死。临床经验是在显露并复位骨折时,尽可能少剥离附着在骨折块的软组织,以免损伤骨折块血供。以结节间沟为标志,依靠间接复位技术进行复位,注意软组织保护,尤其是内侧软组织对于肱骨头的血供有重要作用,更应该注意保护,上述操作对于预防肱骨头坏死具有重要意义。 2.5 锁定接骨板治疗肱骨近端三、四部分骨折的并发症 北京大学人民医院创伤骨科付中国等[11]对锁定接骨板治疗肱骨近端三、四部分骨折的52例患者进行跟踪随访,40例患者为三部分大结节骨折合并外科颈骨折,其中有9例患者还同时合并盂肱关节前脱位;12例患者为四部分骨折,其中9例为外展嵌插型,3例合并脱位。对52例患者进行锁定接骨板内固定治疗,结果12例患者出现相关并发症,并发症发生率为23.07%,其中延迟愈合1例,治疗后出现大结节移位2例,接骨板撞击肩峰2例,螺钉穿出3例,肱骨头坏死3例,肱骨头内翻畸形愈合4例,其中3例患者同时合并2种以上并发症,详细结果见表1。 北京大学积水潭医院运动损伤科鲁谊等[12]对33例肱骨近端三、四部分骨折应用锁定接骨板内固定治疗的患者进行跟踪随访,17例为三部分大结节骨折,其中5例合并肱骨头前脱位,1例合并肱骨头后脱位;15例为四部分骨折,其中9例为外展嵌插型,2例合并肱骨头脱位。对33例患者进行锁定接骨板内固定治疗,结果8例患者出现相关并发症,并发症发生率为24.24%,其中肱骨头缺血坏死5例,螺钉穿出1例,螺钉松动1例,腋静脉损伤1例,8例患者均为单一并发症,详细结果见表2。"
"

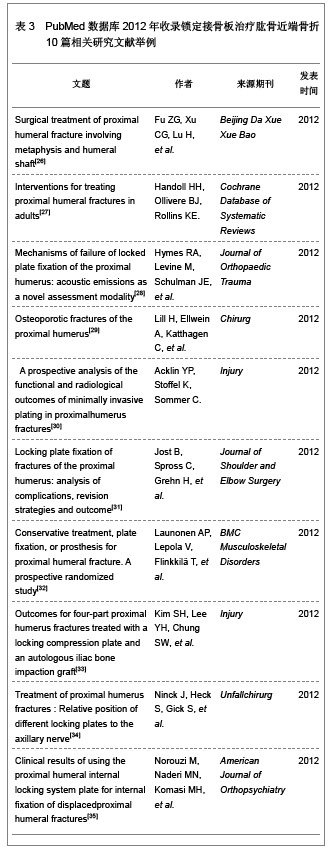
从上述2组应用锁定接骨板治疗肱骨近端三、四部分骨折后的并发症统计结果可以看出患者年龄、性别、骨折类型、骨折的严重程度以及内固定钢板的类型均是并发症发生的风险因素。其中螺钉穿出、螺钉松动、接骨板撞击肩峰、大结节移位为内固定相关并发症,延迟愈合、腋静脉损伤、肱骨头坏死以及肱骨内翻畸形愈合为非内固定相关并发症[19]。锁定接骨板内固定治疗肱骨近端三、四部分骨折虽然可以获得较好的治疗效果,但是同时也存在很多的不足,因此,在应用时要综合考虑患者全身状态、上肢功能、肱骨头血运及软组织完整性等多方面因素严格合理选择合适的治疗方法,严格规范操作,良好的复位以及对周围血运良好保护,同时辅助影像学检查,尽量避免任何并发症的发 生[20-22]。 2.6 锁定接骨板治疗肱骨近端三、四部分骨折的优缺点 锁定接骨板是根据生物接骨术理念和肱骨近端局部解剖特点及生物力学特性研究设计的新一代接骨板[23],锁定接骨板的出现改善了传统钢板的内固定效果,其应用于治疗肱骨近端三、四部分骨折的优点可以总结为以下几点[13]:①作为解剖型接骨板,适合肱骨近端特殊的解剖形态,术中无需预弯。②作为一种内固定支架,改变了接骨板与骨骼间以摩擦力为基础的传统固定模式,使接骨板与骨面间的压力降至最低,最大程度保护了骨膜和骨的血运从而使骨折愈合有更好的生物学环境。③螺钉与接骨板的角度固定,对骨折端产生了良好的稳定作用。④肱骨头固定螺钉向不同方向交叉设计,提高了内固定物的抗拔出力,特别适合于骨质疏松患者。⑤钉板间锁定固定有较好的锚合力和较高的抗拉力,可防止螺钉退出和内固定松动,对肱骨头的支持固定较其它钢板得到明显加强,尤其是应用于骨质疏松性骨折或粉碎性骨折。⑥锁定接骨板近端边缘有多个缝合孔,有利于关节囊及肩袖损伤的修复,也可以作为克氏针临时固定骨块的针孔。⑦体积小,操作简单,减少对软组织的剥离和刺激,降低肩峰撞击症的发生率。锁定接骨板治疗肱骨近端三、四部分骨折有很多的优点,但是文章研究显示其应用也可以发生大结节移位、肩峰撞击、螺钉松动及穿出、肱骨头坏死、肱骨头内翻畸形愈合、感染、延迟愈合以及神经血管损伤等相关并发症,并且锁定接骨板价格昂贵,因此应用时综合考虑患者的整体状态以及经济能力等多种因素进行选择,以达到最佳的临床治疗效果,减少并发症的发生[24-25]。 2.7 PubMed数据库2012年收录锁定接骨板治疗肱骨近端骨折10篇相关研究文献举例 见表3。"
| [1] Lind T, Krøner K, Jensen J. The epidemiology of fractures of the proximal humerus. Arch Orthop Trauma Surg. 1989;108 (5): 285-287. [2] Kannus P, Palvanen M, Niemi S, et al. Osteoporotic fractures of the proximal humerus in elderly Finnish persons: sharp increase in 1970-1998 and alarming projections for the new millennium. Acta Orthop Scand. 2000;71(5):465-470. [3] Neer CS 2nd. Displaced proximal humeral fractures. I. Classification and evaluation. J Bone Joint Surg Am. 1970; 52(6):1077-1089. [4] Resch H, Hübner C, Schwaiger R. Minimally invasive reduction and osteosynthesis of articular fractures of the humeral head. Injury. 2001;32 Suppl 1:SA25-32. [5] Park MC, Murthi AM, Roth NS, et al. Two-part and three-part fractures of the proximal humerus treated with suture fixation. J Orthop Trauma. 2003;17(5):319-325. [6] Ruchholtz S, Hauk C, Lewan U, et al. Minimally invasive polyaxial locking plate fixation of proximal humeral fractures: a prospective study. J Trauma. 2011;71(6):1737-1744. [7] 张殿英,杨明,徐海林,等.LCP治疗肱骨近端骨折[J].中国矫形外科杂志,2004,12(14):1055-1057.[8] Fankhauser F, Boldin C, Schippinger G, et al. A new locking plate for unstable fractures of the proximal humerus. Clin Orthop Relat Res. 2005;(430):176-181. [9] Plecko M, Kraus A. Internal fixation of proximal humerus fractures using the locking proximal humerus plate. Oper Orthop Traumatol. 2005;17(1):25-50. [10] 万方数据库.万方数据知识服务平台[DB/OL].2012-10-28.http://www.wanfangdata.com.cn/ [11] 付中国,邓磊,白露,等.肱骨近端骨折锁定接骨板治疗术后并发症分析[J].北京大学学报(医学版),2011,43(5):666-670.[12] 鲁谊,朱以明,姜春岩,等.锁定钢板治疗肱骨近端骨折的并发症分析[J].中华创伤杂志,2008,24(10):808-813.[13] 张长青,苏琰,曾炳芳.肱骨近端锁定接骨板治疗肱骨近端骨折的临床分析及手术技巧[J].中华手外科杂志,2005,21(5):262- 264.[14] Neviaser AS, Hettrich CM, Dines JS, et al. Rate of avascular necrosis following proximal humerus fractures treated with a lateral locking plate and endostealimplant. Arch Orthop Trauma Surg. 2011;131(12):1617-1622. [15] El-Sayed MM. Surgical management of complex humerus head fractures. Orthop Rev (Pavia). 2010;2(2):e14. [16] Foroohar A, Tosti R, Richmond JM, et al. Classification and treatment of proximal humerus fractures: inter-observer reliability and agreement across imaging modalities and experience. J Orthop Surg Res. 2011;6:38. [17] Baumgartner D, Nolan BM, Mathys R, et al. Review of fixation techniques for the four-part fractured proximal humerus in hemiarthroplasty. J Orthop Surg Res. 2011;6:36. [18] Altman GT, Gallo RA, Molinero KG, et al. Minimally invasive plate osteosynthesis for proximal humerus fractures: functional results of treatment. Am J Orthop (Belle Mead NJ). 2011;40(3):E40-47. [19] Südkamp N, Bayer J, Hepp P, et al. Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate. Results of a prospective, multicenter, observational study. J Bone Joint Surg Am. 2009; 91(6):1320-1328. [20] Zyto K, Kronberg M, Broström LA. Shoulder function after displaced fractures of the proximal humerus. J Shoulder Elbow Surg. 1995;4(5):331-336. [21] Misra A, Kapur R, Maffulli N. Complex proximal humeral fractures in adults--a systematic review of management. Injury. 2001;32(5):363-372. [22] 曾炳芳,罗从风.重视骨折并发症的处理[J].中华创伤骨科杂志, 2006,8(7):601-602.[23] Gavaskar AS, Muthukumar S, Chowdary N. Biological osteosynthesis of complex proximal humerus fractures: surgical technique and results from a prospective single center trial. Arch Orthop Trauma Surg. 2010;130(5):667- 672. [24] 张华,倪卫东,高仕长,等.锁定加压接骨板治疗肱骨近端骨折[J].中华创伤杂志,2008,24(7):527-530.[25] 黄磊,李广旭,李波,等.PHILOS锁定加压接骨板与肱骨近端锁定加压接骨板治疗肱骨近端骨折[J].中国组织工程研究与临床康复,2010,14(52):9861-9864.[26] Fu ZG, Xu CG, Lu H, et al. Surgical treatment of proximal humeral fracture involving metaphysis and humeral shaft. Beijing Da Xue Xue Bao. 2012;44(6):887-890. [27] Handoll HH, Ollivere BJ, Rollins KE. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev. 2012. [28] Hymes RA, Levine M, Schulman JE, et al. Mechanisms of Failure of Locked Plate Fixation of the Proximal Humerus: Acoustic Emissions as a Novel Assessment Modality. J Orthop Trauma. 2012. [29] Lill H, Ellwein A, Katthagen C, et al. Osteoporotic fractures of the proximal humerus. Chirurg. 2012;83(10):858-865. [30] Acklin YP, Stoffel K, Sommer C. A prospective analysis of the functional and radiological outcomes of minimally invasive plating in proximalhumerus fractures. Injury. 2012. [31] Jost B, Spross C, Grehn H, et al. Locking plate fixation of fractures of the proximal humerus: analysis of complications, revision strategies and outcome. J Shoulder Elbow Surg. 2012. [32] Launonen AP, Lepola V, Flinkkilä T, et al. Conservative treatment, plate fixation, or prosthesis for proximal humeral fracture. A prospective randomized study. BMC Musculoskelet Disord. 2012;13:167. [33] Kim SH, Lee YH, Chung SW, et al. Outcomes for four-part proximal humerus fractures treated with a locking compression plate and an autologous iliac bone impaction graft. Injury. 2012;43(10):1724-1731. [34] Ninck J, Heck S, Gick S, et al. Treatment of proximal humerus fractures : Relative position of different locking plates to the axillary nerve. Unfallchirurg. 2012. [35] Norouzi M, Naderi MN, Komasi MH, et al. Clinical results of using the proximal humeral internal locking system plate for internal fixation of displacedproximal humeral fractures. Am J Orthop (Belle Mead NJ). 2012;41(5):E64-8. [36] 周旭军.国人肱骨近端行肩关节置换与接骨板板固定的应用解剖研究[D].湖南:南华大学,2007:1-49.[37] Gardner MJ, Weil Y, Barker JU, et al. The importance of medial support in locked plating of proximal humerus fractures. J Orthop Trauma. 2007;21(3):185-191.[38] Egol KA, Ong CC, Walsh M, et al. Early complications in proximal humerus fractures (OTA Types 11) treated with locked plates. J Orthop Trauma. 2008;22(3):159-164. [39] Cornell CN, Levine D, Pagnani MJ. Internal fixation of proximal humerus fractures using the screw-tension band technique. J Orthop Trauma. 1994;8(1):23-27.[40] Koukakis A, Apostolou CD, Taneja T, et al. Fixation of proximal humerus fractures using the PHILOS plate: early experience. Clin Orthop Relat Res. 2006;442:115-120. [41] Lill H, Hepp P, Rose T, et al. The angle stable locking-proximal-humerus-plate (LPHP) for proximal humeral fractures using a small anterior-lateral-deltoid-splitting- approach-technique and first results. Zentralbl Chir. 2004; 129(1):43-48. [42] Hettrich CM, Neviaser A, Beamer BS, et al. Locked plating of the proximal humerus using an endosteal implant. J Orthop Trauma. 2012;26(4):212-215.[43] Itamura J, Dietrick T, Roidis N, et al. Analysis of the bicipital groove as a landmark for humeral head replacement. J Shoulder Elbow Surg. 2002;11(4):322-326. |
| [1] | Xu Feng, Kang Hui, Wei Tanjun, Xi Jintao. Biomechanical analysis of different fixation methods of pedicle screws for thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1313-1317. |
| [2] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [3] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [4] | Chen Xinmin, Li Wenbiao, Xiong Kaikai, Xiong Xiaoyan, Zheng Liqin, Li Musheng, Zheng Yongze, Lin Ziling. Type A3.3 femoral intertrochanteric fracture with augmented proximal femoral nail anti-rotation in the elderly: finite element analysis of the optimal amount of bone cement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1404-1409. |
| [5] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [6] | Zhang Shangpu, Ju Xiaodong, Song Hengyi, Dong Zhi, Wang Chen, Sun Guodong. Arthroscopic suture bridge technique with suture anchor in the treatment of acromioclavicular dislocation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1417-1422. |
| [7] | Zhang Chao, Lü Xin. Heterotopic ossification after acetabular fracture fixation: risk factors, prevention and treatment progress [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1434-1439. |
| [8] | Zhou Jihui, Li Xinzhi, Zhou You, Huang Wei, Chen Wenyao. Multiple problems in the selection of implants for patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1440-1445. |
| [9] | Wang Debin, Bi Zhenggang. Related problems in anatomy mechanics, injury characteristics, fixed repair and three-dimensional technology application for olecranon fracture-dislocations [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1446-1451. |
| [10] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [11] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [12] | Xu Yulin, Shen Shi, Zhuo Naiqiang, Yang Huilin, Yang Chao, Li Yang, Zhao Heng, Zhao Lu. Biomechanical comparison of three different plate fixation methods for acetabular posterior column fractures in standing and sitting positions [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 826-830. |
| [13] | Cai Qunbin, Zou Xia, Hu Jiantao, Chen Xinmin, Zheng Liqin, Huang Peizhen, Lin Ziling, Jiang Ziwei. Relationship between tip-apex distance and stability of intertrochanteric femoral fractures with proximal femoral anti-rotation nail: a finite element analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 831-836. |
| [14] | Hou Guangyuan, Zhang Jixue, Zhang Zhijun, Meng Xianghui, Duan Wen, Gao Weilu. Bone cement pedicle screw fixation and fusion in the treatment of degenerative spinal disease with osteoporosis: one-year follow-up [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 878-883. |
| [15] | He Li, Tian Wei, Xu Song, Zhao Xiaoyu, Miao Jun, Jia Jian. Factors influencing the efficacy of lumbopelvic internal fixation in the treatment of traumatic spinopelvic dissociation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 884-889. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||