Chinese Journal of Tissue Engineering Research ›› 2013, Vol. 17 ›› Issue (4): 696-703.doi: 10.3969/j.issn.2095-4344.2013.04.021
Previous Articles Next Articles
Intramedullary nail internal fixation for the treatment of humeral fracture
Wang Yi-min1, Xu Kai-ming2, Huang Xing-zhong1, Huang Ai-jun1, Li Zhong-tan1, Ma Shu-qiang1
- 1 Shenzhen Futian Hospital of Guangdong Medical College, Shenzhen 518033, Guangdong Province, China
2 Peking University Shenzhen Hospital, Shenzhen 518036, Guangdong Province, China
-
Received:2012-06-18Revised:2012-08-27Online:2013-01-22Published:2013-03-05 -
About author:Wang Yi-min☆, M.D., Chief physician, Shenzhen Futian Hospital of Guangdong Medical College, Shenzhen 518033, Guangdong Province, China wymsz.good@163.com
CLC Number:
Cite this article
Wang Yi-min, Xu Kai-ming, Huang Xing-zhong, Huang Ai-jun, Li Zhong-tan, Ma Shu-qiang. Intramedullary nail internal fixation for the treatment of humeral fracture[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(4): 696-703.
share this article

1 肱骨髓内钉的种类 肱骨骨折多数可通过手法复位,夹板固定治疗,但对一些不稳定性骨折常需要切开复位置入固定。髓内钉固定为切开复位提供了基础。其对骨折块骨膜和骨折端软组织血运干扰小、应力遮挡小、去除固定后再骨折少、固定力度大、避免了不必要的植骨、手术时间短、出血少、不需要外固定、感染概率相对小等优点,越来越多的运用于临床。 1.1 Gross-Kempf钉 20世纪70年代后期,Gross和Kempf[8]对内锁钉作了改进,以远近端的两枚横向锁钉为特征,近端1/3不开槽,而且较远端粗,配有打入器和近、远端锁钉瞄准器,远端锁钉的穿针必须在影像增强装置的引导小金星,成为Gross-Kempf钉。 1.2 鱼口交锁髓内钉[9] 鱼口状交锁髓内钉整体采用不锈钢无缝管制成,外表面两侧具有纵形凹槽,下部开有槽口呈鱼口状,前端为喇叭形,上部加工有一横孔,上端具有内螺纹,顶开有定位口。置入必须在X射线辅助下进行,可牢靠固定骨折,缩短手术时间,胫骨和肱骨都可以使用。 1.3 全锁髓内钉 1997年,吴岳嵩等[10]报道对Huckstep钉修改而成的金属髓内钉。可在直视下打入髓内钉和锁钉,不需要X射线辅助,并且达到解剖对位的可能性较大。 1.4 非扩髓型肱骨内锁髓内钉[11] 该钉是由髓内针、内锁螺钉和尾部钉3部分构成。当内锁髓内钉安装完毕后,尾部钉通过髓内钉顶端的内螺纹拧入,防止软组织长入,便于取钉。 1.5 Seidel钉[12] Seidel钉为自带锁肱骨髓内钉,可通过定位器拧入。用该钉治疗AO角钢板固定失败的肱骨骨折也取得了成功。 1.6 髓内扩张自锁钉 1998年李健民等[13]在组合式防旋髓内钉的基础上改良而成。具有不扩髓、不需要X射线定位、抗疲劳极限高、无明显应力集中等优点。 1.7 可降解生物髓内钉 1998年Vander Elst等[14]采用多聚乳酸及多聚羟基乙酸混合物制成髓内钉应用山羊的股骨骨折,经过2.5年的随访,骨折愈合良好,而肱骨较股骨在抗重力和抗旋转等方面的要求更小一些,此类髓内钉很快会用于临床。"

2 结果 2.1 肱骨髓内钉的类型 髓内钉的应用与发展为骨折患者的肢体功能康复起到了很大的作用,早期重建了患肢的力学稳定,后期保证了骨折在复位后的最佳对位上完全愈合,能够最大限度保留骨的血供。需要注意的是,因为不同类型的髓内钉的原理不同,所以要掌握不同类型髓内钉的适应证,才能最大限度发挥不同类型髓内钉的优势。"

3 常用肱骨髓内钉的材料组成 肱骨髓内钉材料是一种用作生物医用材料的金属或合金。目前临床应用的材料主要包括医用贵金属、医用钛、铌等单质金属,以及不锈钢、钛合金等。 3.1 医用不锈钢 用作生物医用材料的不锈钢,具有良好的耐腐蚀性能和综合力学性能,且加工工艺简便,是生物医用金属材料中应用最广最多的一类材料。作为骨折内固定材料,各种规格的皮质骨和松质骨加压螺钉、脊椎钉、哈氏棒、卢士棒等应用应用于骨折修复。 3.2 医用钴基合金 以其优良的力学性能和较好的生物相容性,尤其是优良的耐蚀、耐磨和铸造性能广泛得到应用。医用钴基合金也是常用的医用金属材料,相对不锈钢而言,医用钴基合金更适合于制造承载苛刻、耐磨性要求较高的长期植入体。 3.3 钛和钛合金 钛具有无毒、质轻、强度高、生物相容性好等优点,而且纯钛不会生锈,耐高温、低温、耐腐蚀,可与骨组织直接连接形成物理性结合。其生物相容性、耐腐蚀性和抗疲劳性能都优于不锈钢和钴基合金。在骨科领域应用广泛,用于制作各种骨折内固定器械等。 3.4 医用贵金属和钽、铌、锆等金属 最先广泛用于临床治疗的金属是金、银。铂等贵重金属。具有良好的稳定性和加工性能。铌、锆、钽及钛都具有极相似的组织结构和化学性能,但都应为其价格较贵,广泛应用受到限制。 3.5 形状记忆合金 是一种新型医用材料,中国医用形状记忆合金始于20世纪70年代,并很快得到了广泛应用。临床上已采用的形状记忆合金主要有镍钛形状记忆合金和铜基形状记忆合金,前者应用广泛。"

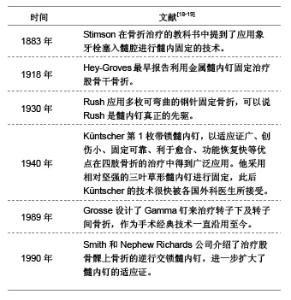
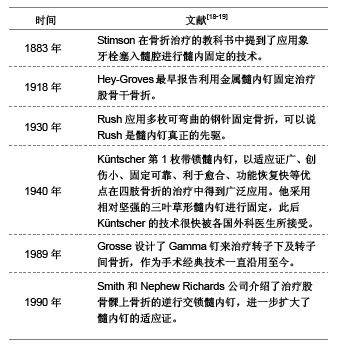
4 髓内钉的临床应用过程 应用髓内钉治疗骨折已经有120余年的历史,早在100多年前,就有人用不同的材料的棒状物进行过动物实验和临床观察。近年来随着骨折生物学固定观点的提出,髓内钉置入固定已经成为包括肱骨骨折在内的四肢骨干骨折治疗的首选。"
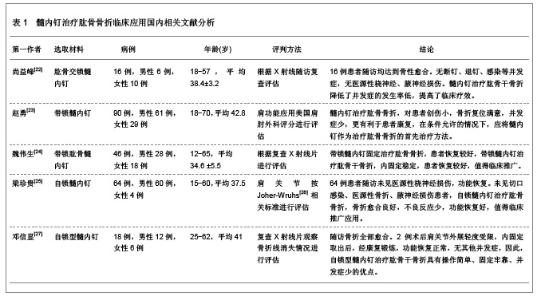
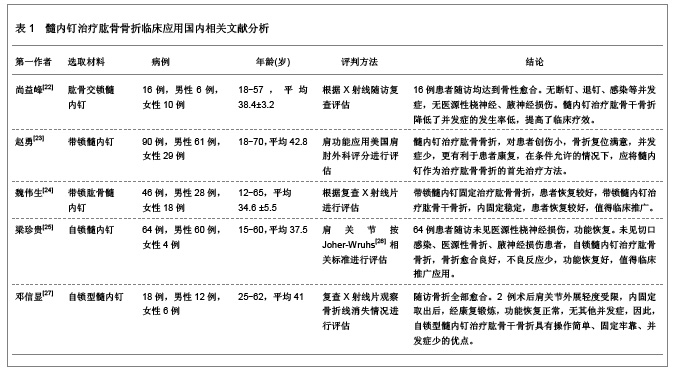
5 髓内钉置入内固定治疗肱骨骨折的相关文献分析 5.1 资料来源 与肱骨骨折的几种治疗方法相关研究文献[20-21],检索数据库时间范围1999至2011年,以“肱骨近端(Proximal humerus);骨折(Fracture);髓内钉(Intramedullary nail) ;人工假体置换(Prosthesis replacement) ;骨折固定(Fracture fixation)”为检索词,选取文献35篇[19,22-54]。 5.2 纳入标准 ①髓内钉治疗肱骨骨折的临床应用。②肱骨髓内钉置入后并发症分析。③髓内钉治疗肱骨骨折后并发症的防治。④肱骨折钢板固定与髓内钉固定治疗的分析。⑤肱骨髓内钉影响肩关节功能的研究。 5.3 排除标准 ①老年性肩关节骨性关节炎的诊治。②肿瘤核素诊断现状与进展。③上肢神经损伤的康复。④重复研究的文章。 5.4 分析指标 ①肱骨髓内钉种类。②肱骨髓内钉并发症。③肱骨髓内钉影响肩关节功能的机制。④肱骨髓内钉对骨折愈合的影响。 5.5 髓内钉置入固定治疗肱骨骨折相关国内外文献 5.5.1 肱骨骨折髓内钉固定治疗相关国内文献 髓内钉的设计理念为尽量保护骨的外周血运,包括复位和固定时减少骨膜下剥离、软组织暴露等。从生物力学上分析,髓内钉固定肱骨后,生理负荷下的生物力学表现强度偏高一些,有利于上肢早期功能锻炼。髓内钉治疗肱骨骨折临床应用国内相关文献分析,见表1。"
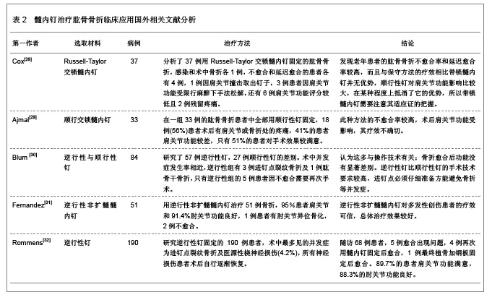
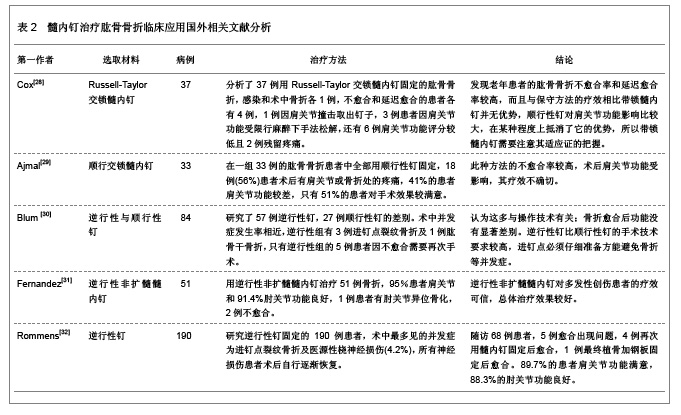
5.5.2 肱骨骨折髓内钉固定治疗相关国外文献 肱骨属于非负重骨,轴向引力与扭矩及弯矩为其所受力。而保证骨折愈合的抗旋转,抗弯曲的关键参数取决于内固定物的材料力学性能以及内固定物与骨相嵌的密切程度。部分肱骨骨折可因髓内钉而得到稳定,这是因为髓内钉是通过间接复位保护血供,因此,髓内钉置入治疗肱骨骨折正成为越来越多骨科医生首选的内固定方法。 肱骨骨折髓内钉固定治疗相关国外文献分析见表2。"
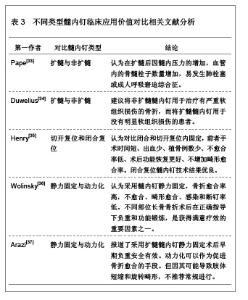
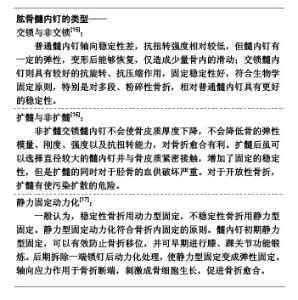
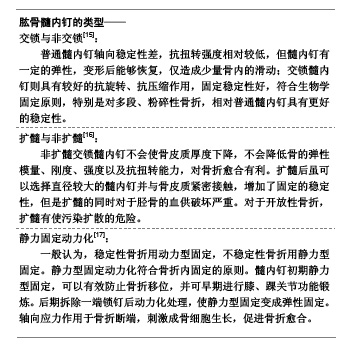
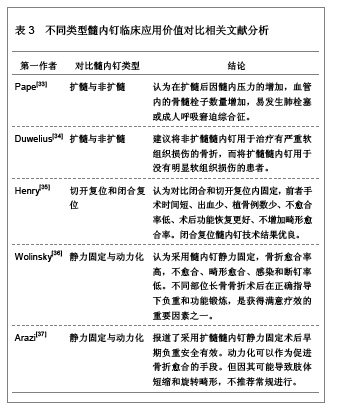
6 不同类型髓内钉临床应用价值的比较 由于肱骨是非负重长骨,在内固定的选用上不强调坚强内固定和解剖复位,但应考虑恢复正常的对位对线关系,以防止外观上畸形明显。在骨折的治疗中,保证骨折块的血液供应是最重要的,在保证骨折部位的长度和轴线恢复正常、旋转移位纠正和保持骨折区段的稳定性的基础上,尽可能保留骨折区段的血液供应,能有效地防止骨折不连的发生。不同类型的髓内钉在临床应用中有各自的优势和不足,只有清楚的认识到各类型髓内钉的临床应用价值,才能够尽可能少的破坏骨折块的血运,有利于骨折的尽早愈合及降低骨折不连接的发生率。随着肱骨髓内钉的发展,还将髓内钉分为扩髓肱骨钉和不扩髓肱骨钉、静力型肱骨钉和动力型肱骨钉以及外带锁肱骨钉和自带锁肱骨钉等多种钉型,应用于各种类型的骨折,特别适合于严重粉碎性骨折和阶段性骨折。不同类型髓内钉临床应用价值对比相关文献分析,见表3。"
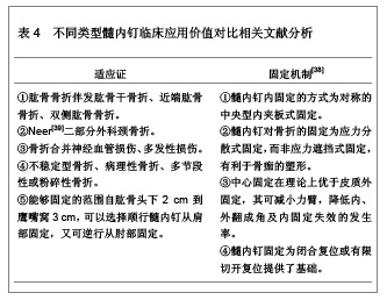
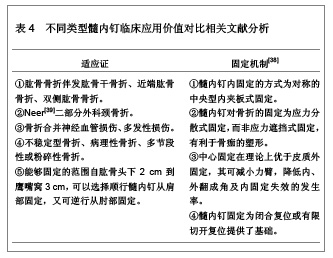
7 髓内钉置入内固定治疗肱骨骨折的适应证与内固定机制及方法 肱骨髓内钉内固定技术已经广泛应用于临床。与其他骨科骨折固定物一样,髓内钉也有其适应证、固定机制和并发症。已报道的肱骨髓内钉并发症有感染、骨折愈合畸形、神经血管损伤、髓内钉断裂等。 7.1 髓内钉置入内固定治疗肱骨骨折的适应证与内固定机制 髓内钉由主钉、锁钉和盖帽3部分组成,其材料为不锈钢。髓内钉使用的金属材料属于比较特殊的质地,对身体的影响很小,和人体有相容性。严格掌握髓内钉治疗肱骨骨折的适应证与固定机制,不但能在治疗中有效支撑和固定骨折,而且能降低发生骨折不连、桡神经损伤的概率。髓内钉置入固定治疗肱骨骨折的适应证与内固定机制,见表4。"
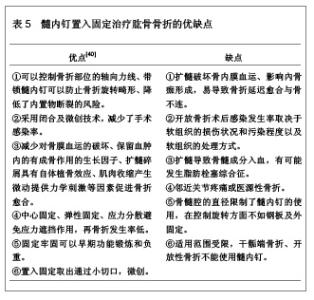
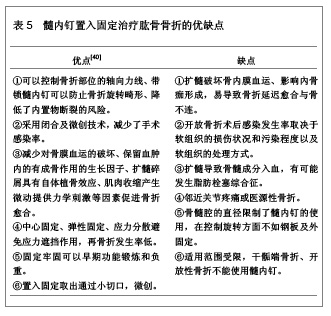
7.2 髓内钉置入内固定治疗肱骨骨折的优缺点 肱骨独特的解剖结构、血运、应力类型及方向以及邻近关节都与股骨和胫骨的大相径庭。早期的肱骨髓内钉主要有Küntscher钉,Hackethal钉和Ender钉、Russ钉等,这几种髓内钉均没有内锁作用,不能有效的控制骨折端的分离和旋转,需要外固定,而且早期出现退钉显像,影响肩关节功能。目前使用较多的髓内钉有改良的Küntscher钉、Gross-Kempf钉、Seidel钉以及全锁髓内钉等。在生物力学上,髓内钉除了拉伸刚度与加压钢板接近外,其抗轴向压缩、抗弯曲、抗扭转等性能均优于加压钢板。对骨折部软组织损伤小,骨膜剥离少,血供破坏少,中心性固定,无力矩存在,应力遮挡作用较小等优点。但是过细的髓内钉可能导致固定不稳定而使骨折不愈合。粉碎性骨折用髓内钉固定时不能有分离移位以免延迟愈合。髓内钉置入固定治疗肱骨骨折的优缺点,见表5。"
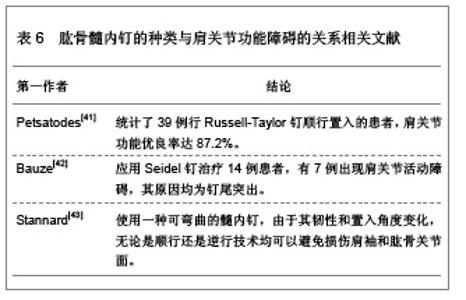
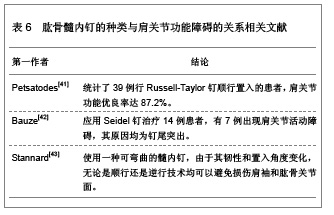
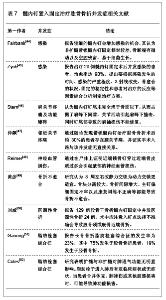
8 髓内钉置入内固定治疗肱骨骨折的并发症 8.1 不同种类的肱骨髓内钉对肩关节功能的影响 肩关节功能障碍是肱骨髓内钉固定后常见的并发症,髓内钉的种类也是造成腋神经损伤的原因,不同的肱骨髓内钉引起的肩关节功能障碍的发生率不同。肱骨髓内钉的种类与肩关节功能障碍的关系相关文献,见表6。"
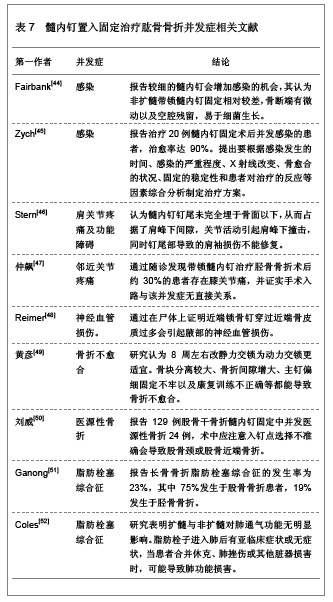
8.2 髓内钉置入内固定治疗肱骨骨折并发症相关文献 尽管髓内钉置入固定治疗肱骨骨折在临床上应用广泛,但因为肩关节活动范围大、患者对生活质量的要求高,而关节重建后的功能恢复水平很大程度取决于周围软组织的条件。为避免并发症及改善预后,仔细选择适应证、熟悉肩关节解剖和力学机制外,掌握髓内钉置入固定治疗肱骨骨折并发症的原因也是非常重要的。目前对髓内钉置入固定治疗肱骨骨折的文献报告较多,但对其术后并发症的研究较少。应合理选择肱骨髓内钉的类型,提高手术操作技巧。一般情况下,顺行法适用于肱骨中段以上部位骨折,逆行法适用于肱骨中远段骨折,但是,逆行髓内钉内固定有较高的医源性骨折的可能性。髓内钉置入固定治疗肱骨骨折并发症相关文献,见表7。"
| [1] 张鹏翼,黄煌渊,陈文钧.肱骨骨折的手术治疗进展[J].上海医学, 2004,27(12):946-948.[2] Court-Brown CM, Caesar B.Epidemiology of adult fractures: A review.Injury.2006;37(8):691-697.[3] 杨吉青.肱骨骨折手术与非手术治疗的疗效比较[J].中国临床保健杂志,2008,11(4):392.[4] 侯辉歌.肱骨近端锁定钢板治疗复杂的肱骨骨折[J].中国骨与关节损伤杂志,2008,23(2):120.[5] 张作君.肱骨近端骨折国内外治疗现状[J].中国矫形外科杂志, 2000,7(5):478-481.[6] Christensen NO.Küntscher intramedullary reaming and nail fixation for nonunion of the humerus.Clin Orthop Relat Res. 1976;(116):222-225.[7] Jensen CH,Hansen D,Jørgensen U.Humeral shaft fractures treated by interlocking nailing: a preliminary report on 16 patients.Injury.1992;23(4):234-236.[8] Kempf I,Grosse A,Abalo C.Locked intramedullary nailing. Its application to femoral and tibial axial, rotational, lengthening, and shortening osteotomies.Clin Orthop Relat Res.1986; (212):165-173.[9] 吴乃庆,宋李军,王道新,等.鱼口交锁髓内钉和其它三种交锁髓内钉的生物力学性能比较[J].中华骨科杂志,1997,17(4):233-236.[10] 吴岳嵩,徐伯诚.矩形随内钉的设计及临床应用.中华骨科杂志, 1991,11(6):405.[11] 韩一生,赵广跃,刘建,等.非扩髓型肱骨内锁髓内钉的研制和临床应用.中华骨科杂志,1997,14(4):229-232.[12] Evans PD,Conboy V.Locked nailing of humeral fractures.J Bone Joint Surg Br.1993;75(1):165.[13] 李健民,胥少汀,邹德威,等.髓内扩张自锁钉的结构特点及力学行为[J].中华骨科杂志,1998,15(18):728-732.[14] van der Elst M, Bramer JA, Klein CP,et al.Biodegradable interlocking nails for fracture fixation.Clin Orthop Relat Res. 1998;(357):192-204.[15] 周炼.交锁钉和非交锁钉髓内固定对不稳定胫骨骨折的疗效比较[J].海南医学,2009,20(11):65-68.[16] 林研,印心奇,董天华,等.扩髓与非扩髓交锁髓内钉治疗胫骨骨折的疗效比较[J].中华创伤杂志,2001,17(12):709-712.[17] 叶蜀新,王攀,德荣.带锁髓内钉静力型固定动力化在治疗股骨干骨折中的应用[J].泸州医学院学报,2007,30(1):40-41.[18] 陈勤,周政,关龙,等.Gamma钉治疗股骨转子间骨折两种手术方法的临床比较[J].中国修复重建外科杂志,2007,21(10): 1027-1030.[19] Kotela I,Bo?tu? W,Bednarenko M,et al.The use of the gamma nail in fractures of the nearer end of femur.Przegl Lek.2006; 63(7):42-44.[20] 中国知网.中国学术期刊总库[DB/OL].2012-08-10. https://www.cnki.net[21] SCI数据库.Web of Sciencevia ISI Web of Knowledge[DB/OL]. 2012-08-10. http://ip-science.thomsonreuters.com/mjl[22] 尚益峰.髓内钉治疗肱骨骨折16例临床分析[J].中国实用医药, 2012,7(21):100-101.[23] 赵勇.髓内钉在肱骨干骨折内固定治疗中的应用分析[J].医药前沿,2012,2(18):176-177.[24] 魏伟生.带锁髓内钉治疗肱骨骨折的疗效46例观察[J].中外健康文摘,2011,8(05):221-222.[25] 梁珍贵.自锁髓内钉治疗肱骨骨折64例疗效分析[J].健康必读, 2011,8(11):46.[26] Johner R,Wruhs O.Classification of tibial shaft fractures and correlation with results after rigid internal fixation.Clin Orthop Relat Res.1983;Sep(178):7-25.[27] 邓信显.自锁型髓内钉治疗肱骨骨折18例报告[J].华夏医学,2011, 24(3):317-318.[28] Cox MA,Dolan M,Synnott K,et al.Closed interlocking nailing of humeral shaft fractures with the Russell-Taylor nail.J Orthop Trauma.2000;14(5):349-353.[29] Ajmal M,O'Sullivan M,McCabe J,et al.Antegrade locked intramedullary nailing in humeral shaft fractures.Injury.2001; 32(9):692-694.[30] Blum J,Janzing H,Gahr R,etal.Clinical performance of a new medullary humeral nail: antegrade versus retrograde insertion. J Orthop Trauma.2001;15(5):342-349.[31] Fernandez FF,Matschke S,Hülsenbeck A,et al.Five years' clinical experience with the unreamed humeral nail in the treatment of humeral shaft fractures.Injury.2004;35(3): 264-271.[32] Rommens PM,Blum J,Runkel M.Retrograde nailing of humeral shaft fractures.Clin Orthop Relat Res.1998; (350): 26-39.[33] Pape HC,Regel G,Dwenger A,et alInfluence of thoracic trauma and primary femoral intramedullary nailing on the incidence of ARDS in multiple trauma patients.Injury. 1993; 24(3):82-103.[34] Duwelius PJ,Schmidt AH,Rubinstein RA,et al.Nonreamed interlocked intramedullary tibial nailing. One community's experience.Clin Orthop Relat Res.1995; Jun(315):104-113.[35] Henry SL.Supracondylar femur fractures treated percutaneously.Clin Orthop Relat Res.2000;Jun(375):51-59.[36] Wolinsky PR,McCarty E,Shyr Y,et al.Reamed intramedullary nailing of the femur: 551 cases.J Trauma.1999;46(3): 392-399.[37] Arazi M,O?ün TC,Oktar MN,et al.Early weight-bearing after statically locked reamed intramedullary nailing of comminuted femoral fractures: is it a safe procedure?2000;50(4):711-716.[38] 张麒云,范存义,曾炳芳.肱骨髓内钉影响肩关节功能的研究进展[J].上海医学,2008,31(2):144-146.[39] Neer CS 2nd.Four-segment classification of proximal humeral fractures: purpose and reliable use.J Shoulder Elbow Surg. 2002; 11(4):389-400.[40] 张建国,林枫松,张铁良,等.带锁髓内钉应用中的几个问题[J].中华骨科杂志,2005,25(3):181-184.[41] Petsatodes G,Karataglis D,Papadopoulos P,et al.Antegrade interlocking nailing of humeral shaft fractures.J Orthop Sci. 2004;9(3):247-252.[42] Bauze AJ,Clayer MT. Treatment of pathological fractures of the humerus with a locked intramedullary nail.J Orthop Surg (Hong Kong).2003;11(1):34-37.[43] Stannard JP,Harris HW,McGwin G Jr,et al.Intramedullary nailing of humeral shaft fractures with a locking flexible nail.J Bone Joint Surg Am.2003;85(11):2103-2110.[44] Fairbank AC,Thomas D,Cunningham B,et al.Sta-bility of reamed and unreamed intramedullary tibial nails:a biomechanical study.Injury,1995;26(7):483-485.[45] Zych GA,Hutson JJ Jr.Diagnosis and management of infection after tibial intramedullary nailing.Clin Orthop Relat Res.1995;Jun(315):153-162.[46] Stern PJ,Mattingly DA,Pomeroy DL,et al.Intramedullary fixation of humeral shaft fractures.J Bone Joint Surg Am. 1984;66(5):639-646.[47] 仲飙,潘垚,罗从风,等.胫骨干骨折髓内钉治疗后膝关节痛的临床研究[J].中华创伤骨科杂志,2004,6(10):1109-1111.[48] Catone GA,Reimer BL,McNeir D,et al.Tibial autogenous cancellous bone as an alternative donor site in maxillofacial surgery: a preliminary report.J Oral Maxillofac Surg.1992; 50(12):1258-1263.[49] 黄彦,王胜标.股骨干骨折交锁髓内钉固定所致并发症的原因分析及处理[J].中华创伤杂志,2001,17(5):290-292.[50] 刘威,成传德,闻亚非,等.带锁髓内钉治疗股骨干骨折的常见并发症分析[J].中华骨科杂志,2001,21(5):317-319.[51] Ganong RB.Fat emboli syndrome in isolated frac-tures of the tibia and femur.Clin Orthop.1993;Jun(291):208-214.[52] Coles RE,Clements FM,Lardenoye JW,et al. Trans-esophageal echocardiography in quantification of em-boli during femoral nailing:reamed versus unreamed techniques.J South Orthop Assoc.2000;9(2):98-104. |
| [1] | Xu Hao, Ding Lu, Li Xiao. Mechanical effect of mechanical wear of abutment screws on the Morse taper connection implant system: a three-dimensional finite element analysis [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(6): 1375-1383. |
| [2] | Guo Jiachen, Gao Jun, Dai Wenhao, Liao Huayuan, Jiang You, Zhang Xi . Effect of compressive stress microenvironment on cytokines during fracture healing [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(4): 908-916. |
| [3] | Yu Xinlin, Chen Huiyu, Wang Yingying, Guo Weizhong, Feng Bin Lin Chengshou, Lin Wang. Finite element analysis of internal fixation with new retrograde intramedullary nail on lateral femur condyle for distal type A2 femur fractures [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(3): 546-552. |
| [4] | Zhang Junwei, Chen Lingling, Ma Zhenyuan, Nie Weizhi, Li Chaohui, Wang Haitao, Duan Laibao, Hou Jinyong, Bi Hongzheng. Three-dimensional displacement and risk factors of midshaft clavicle fractures treated with titanium elastic intramedullary nailing [J]. Chinese Journal of Tissue Engineering Research, 2026, 30(2): 269-277. |
| [5] | Xu Hao, Ding Lu, Li Xiao. Investigating the effect of the mechanical wear on abutment screw in Morse taper connection implant implant system by using finite element analysis [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(在线): 1-9. |
| [6] | Ao Xiaojing, Li Kun, Liu Yuhang, Yang Xiaoxuan, Wang Xing, Li Zhijun, Ren Xiaoyan, Zhang Shaojie. Development and application of a three-dimensional digital visualization system for children’s neck acupoints [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(9): 1834-1840. |
| [7] | Ma Chi, Wang Ning, Chen Yong, Wei Zhihan, Liu Fengji, Piao Chengzhe. Application of 3D-printing patient-specific instruments combined with customized locking plate in opening wedge high tibial osteotomy [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(9): 1863-1869. |
| [8] | Zhao Jiyu, Wang Shaowei. Forkhead box transcription factor O1 signaling pathway in bone metabolism [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(9): 1923-1930. |
| [9] | Hu Chaoran, Cen Chaode, Yang Yang, Zhou Cheng, Huang Huaxian, Yuan Honghao, Luo Qin, Cao Yongfei. 3D printing assisted minimal invasive plate osteosynthesis versus intramedullary nail for treatment of AO12-C middle-proximal humeral fractures [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(33): 7116-7122. |
| [10] | Bu Xianmin, Liang Di, Zhang Bin, Xu Yingjie, Ding Hao, Wu Bin, Tian Ronghua. Exosomes derived from human umbilical cord mesenchymal stem cells in treatment of osteoporotic femoral fractures in SD rats [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(31): 6634-6641. |
| [11] | Liu Hanfei, Cai Zhencun, Zhou Xueting, Wen Hang, Chen Zhenjun. Mechanisms by which traumatic brain injury promotes bone callus formation and fracture healing [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(29): 6260-6268. |
| [12] | Chen Zhen, Chen Xi, Li Xiaoting, Chen Daxin, Hong Weiwu. Comparison of medial-lateral and lateral-only fixation for pediatric supracondylar humeral fractures: a systematic review and meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(27): 5924-5932. |
| [13] | Rao Xin, Jiang Daixiang, Lu Hui Luo Yangxing, Li Meng, Liu Dingxi, Wu Qimei, Liu Rong. Comparison of biomechanical characteristics of superior and inferior pubic ramus fractures fixed with different internal fixation methods [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(27): 5757-5764. |
| [14] | Zheng Li, Ding Yiheng, Li Xinhao, Wen Zekai, Jiang Bingzheng, Lin Xuexia. Role of neuropilin 1 in promoting angiogenesis-osteogenesis coupling during fracture healing [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(21): 4576-4583. |
| [15] | Cheng Chaoran, Zhang Junxia, Jia Jun. Finite element analysis of muscle loading effect on biomechanics of early healing of femoral stem fractures [J]. Chinese Journal of Tissue Engineering Research, 2025, 29(21): 4413-4420. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||