Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (31): 5077-5084.doi: 10.3969/j.issn.2095-4344.0549
Meta-analysis of clinical outcomes of computer-navigated versus conventional opening wedge high tibial osteotomy
Shi Jun-heng1, Zhong De-gui1, Hong Wei-wu1, Huang Yong-quan2
- 1Guangzhou University of Chinese Medicine, Guangzhou 510006, Guangdong Province, China; 2Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou 510120, Guangdong Province, China
-
Online:2018-11-08Published:2018-11-08 -
Contact:Huang Yong-quan, Master, Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou 510120, Guangdong Province, China -
About author:Shi Jun-heng, MD, Guangzhou University of Chinese Medicine, Guangzhou 510006, Guangdong Province, China -
Supported by:the Scientific Research Project of Traditional Chinese Medicine Bureau of Guangdong Province, No. 20182043
CLC Number:
Cite this article
Shi Jun-heng, Zhong De-gui, Hong Wei-wu, Huang Yong-quan. Meta-analysis of clinical outcomes of computer-navigated versus conventional opening wedge high tibial osteotomy[J]. Chinese Journal of Tissue Engineering Research, 2018, 22(31): 5077-5084.
share this article
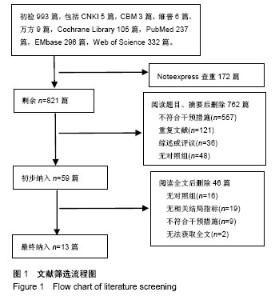
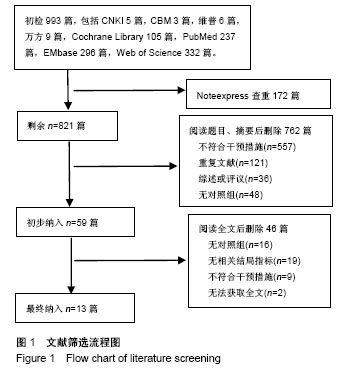
2.1 文献筛选结果 检索各数据库共计检索到993篇文献,应用Noteexpress软件查重排除172篇文献。根据既定纳入排标准,阅读文献题目和摘要排除762篇文献,初步纳入59篇文献。详细阅读全文后,排除46篇文献,最终共纳入13篇,都是已经公开发表的文献,文献筛选流程图见图1。"
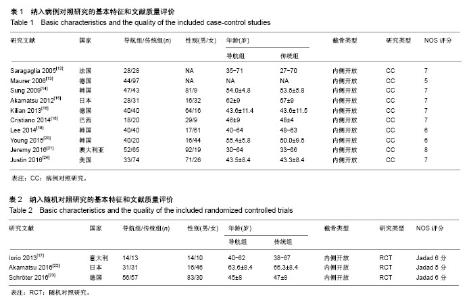
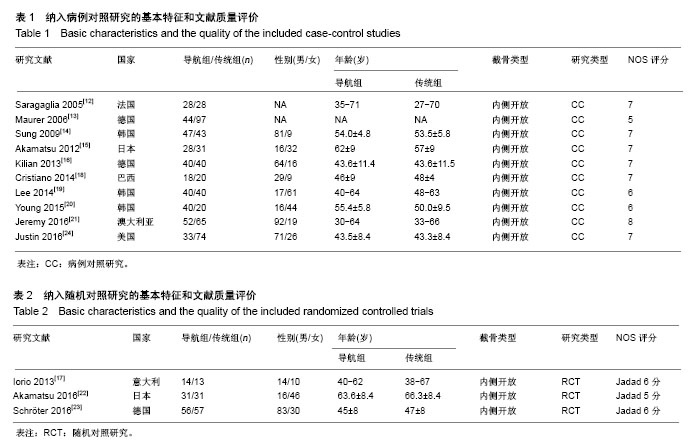
2.2 纳入文献的基本特征和文献质量评价 共纳入13个临床研究[6,9,12-22],包括1 030例内翻膝的患者,导航组为计算机导航辅助下行内侧开放HTO手术的患者,传统组为行传统内侧开放HTO手术的患者,其中导航组患者471例,传统组559例。3项随机对照研究都有明确的纳排标准,均有较高的方法学质量,且Jadad评分均在5分以上[20-22];10个病例对照研究也均有较高的方法学质量,其中NOS评分最低的为5分,最高达到8分[6,9,12-19]。纳入研究的基本特征见表1及表2。"

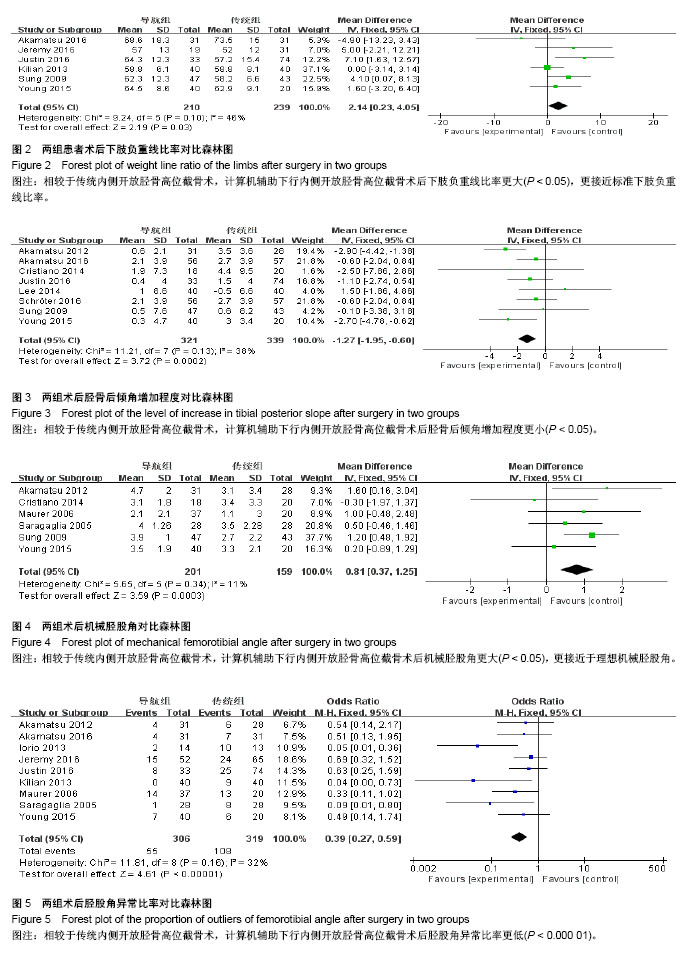
2.3 结局指标Meta分析 2.3.1 术后下肢负重线比率 纳入研究中有6篇文献采用术后下肢负重线比率为结局指标[13,15,18-20,22],其中导航组患者210例、传统组患者239例。经异质性检验, χ2=9.24,P=0.10≥ 0.1,I2=46%,提示纳入的6个研究间具有同质性,故选用固定效应模型进行合并[MD=2.14,95%CI(0.23,4.05)],合并效应量检验Z=2.19,P=0.03 < 0.05,提示相较于传统内侧开放HTO,计算机导航辅助下行内侧开放HTO术后下肢负重线比率更大,更接近Fujisawa[23]认为标准下肢负重线比率点的62%,差异有显著性意义,见图2。 2.3.2 术后胫骨后倾角增加程度 纳入研究中有8篇文献采用术后胫骨后倾角增加程度作为结局指标[13-14,16-18,20-22],其中导航组患者321例、传统组339例患者。经异质性检验,χ2=11.21,P=0.13 > 0.1,I2=38%,提示纳入的8个研究间具有同质性,选用固定效应模型进行合并[MD=-1.27,95%CI(-1.95,-0.60)],合并效应量检验Z=3.72,P= 0.000 2 ≤ 0.05,提示相较于传统内侧开放HTO,计算机导航辅助下行内侧开放HTO术后胫骨后倾角增加程度更小,其差异有显著性意义。见图3。 2.3.3 术后机械胫股角 纳入研究中有6篇文献采用术后机械胫股角作为结局指标[9,12-14,16,18],其中导航组患者201例、传统组159例患者。经异质性检验,χ2=5.65,P=0.34 > 0.1,I2=11%,提示纳入的6个研究间具有同质性,选用固定效应模型进行合并[MD=0.81,95%CI(0.37,1.25)],合并效应量检验Z=3.59,P=0.000 3 < 0.05,提示相较于传统内侧开放HTO,计算机导航辅助下行内侧开放HTO术后机械胫股角更大,更接近于理想机械胫股角[24],差异有显著性意义。见图4。 2.3.4 术后胫股角异常比率 纳入研究中有9篇文献采用术后胫股角异常比率作为结局指标[6,9,12,14-15,18-20,22],其中导航组患者306例、传统组319例患者。经异质性检验,χ2=11.81,P=0.16 > 0.1,I2=32%,提示纳入的9个研究间具有同质性,选用固定效应模型进行合并[OR=0.39,95%CI(0.27,0.59)],合并效应量检验Z=4.61,P < 0.000 01,提示相较于传统内侧开放HTO,计算机导航辅助下行内侧开放HTO术后出现胫股角异常的患者更少、比率更低,差异有显著性意义。见图5。"

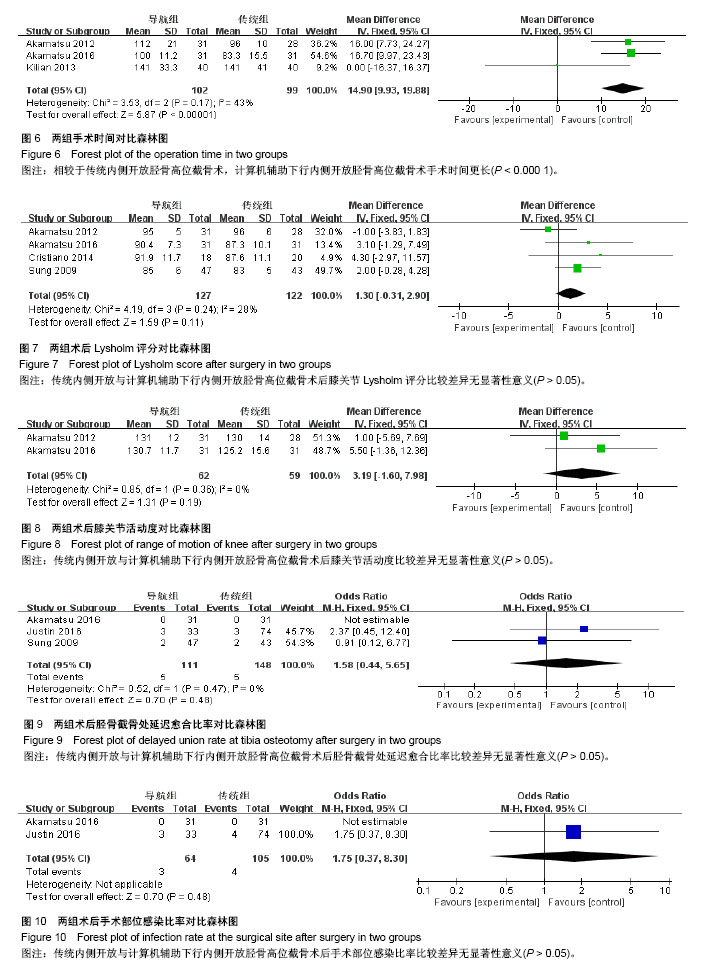
2.3.5 手术时间 纳入研究中有2篇文献采用收拾时间作为结局指标[14,20],其中导航组患者102例、传统组99例患者。经异质性检验,χ2=3.53,P=0.17 > 0.1,I2=43%,提示纳入的2个研究间具有同质性,选用固定效应模型进行合并[MD=14.90,95%CI(9.93,19.88)],合并效应量检验Z=5.87,P < 0.0000 1,提示相较于传统内侧开放HTO,计算机导航辅助下行内侧开放HTO术手术时间更长,差异有显著性意义。见图6。 2.3.6 术后Lysholm评分 纳入研究中有4篇文献采用术后膝关节Lysholm评分作为结局指标[13-14,16,20],其中导航组患者127例、传统组122例患者。经异质性检验, χ2=4.19,P=0.24 > 0.1,I2=28%,提示纳入的4个研究间具有同质性,选用固定效应模型进行合并[MD=1.30,95%CI(-0.31,2.90)],合并效应量检验Z=1.59,P=0.11 > 0.05,提示计算机导航辅助下与传统内侧开放HTO术后膝关节Lysholm评分的差异无显著性意义。见图7。 2.3.7 术后膝关节活动度 纳入研究中有2篇文献采用术后膝关节活动度作为结局指标[14,20],其中导航组患者62例、传统组59例患者。经异质性检验,χ2=0.85,P=0.36 > 0.1,I2=0%,提示纳入的2个研究间具有同质性,选用固定效应模型进行合并[MD=3.19,95%CI(-1.60,7.98)],合并效应量检验Z=1.31,P=0.19 > 0.05,提示计算机导航辅助下与传统内侧开放HTO术后膝关节活动度的差异无显著性意义。见图8。 2.3.8 胫骨截骨处延迟愈合比率 纳入研究中有3篇文献采用术后胫骨截骨处延迟愈合比率作为结局指标[13,19-20],其中导航组111例、传统组148例患者,计算机导航组5例出现胫骨截骨处延迟,传统组5例出现胫骨截骨处延迟。经异质性检验,χ2=0.52,P=0.47 > 0.1,I2=0%,提示纳入的3个研究间具有同质性,选用固定效应模型进行合并[OR=1.58,95%CI(0.44,5.65)],合并效应量检验Z=0.70,P=0.48 > 0.05,提示计算机导航辅助下与传统内侧开放HTO术后胫骨截骨处延迟愈合比率的差异无显著性意义。见图9。 2.3.9 手术部位感染比率 纳入研究中有2篇文献采用术后手术部位感染比率作为结局指标[19-20],其中导航组患者64例、传统组105例患者,导航组3例出现术后手术部位感染,传统组4例出现术后手术部位感染。由于1项研究报道导航组和传统组均未出现手术部位感染[20],异质性检验无法运用,合并效应量[OR=1.75,95%CI(0.37,8.30)],合并效应量检验Z=0.70,P=0.48,提示计算机导航辅助下与传统内侧开放HTO后手术部位感染比率的差异无显著性意义。见图10。"
| [1] Sherman MF, Warren RF, Marshall JL, et al. A clinical and radiographical analysis of 127 anterior cruciate insufficient knees. Clin Orthop Relat Res.1988;227:229-237.[2] Johnson DL, Urban WJ, Caborn DN, et al. Articular cartilage changes seen with magnetic resonance imaging-detected bone bruises associated with acute anterior cruciate ligament rupture. Am J Sports Med. 1998;26(3):409-414.[3] Nielsen AB, Yde J. Epidemiology of acute knee injuries: a prospective hospital investigation. J Trauma. 1991;31(12): 1644-1648.[4] 张英泽,李存祥,李冀东,等.不均匀沉降在膝关节退变及内翻过程中机制的研究[J]. 河北医科大学学报,2014,35(2):218-219.[5] Rossi R, Bonasia DE, Amendola A. The role of high tibial osteotomy in the varus knee. J Am Acad Orthop Surg. 2011; 19(10):590-599.[6] Iorio R, Pagnottelli M, Vadala A, et al. Open-wedge high tibial osteotomy: comparison between manual and computer-assisted techniques. Knee Surg Sports Traumatol Arthrosc.2013;21(1):113-119.[7] Yan J, Musahl V, Kay J, et al. Outcome reporting following navigated high tibial osteotomy of the knee: a systematic review. Knee Surg Sports Traumatol Arthrosc.2016;24(11): 3529-3555.[8] Hankemeier S, Hufner T, Wang G, et al. Navigated open-wedge high tibial osteotomy: advantages and disadvantages compared to the conventional technique in a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2006; 14(10):917-921.[9] Maurer F, Wassmer G. High tibial osteotomy: does navigation improve results?. Orthopedics.2006;29(10 Suppl): S130-S132.[10] Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Control Clin Trials. 1996;17(1):1-12.[11] Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603-605. [12] Saragaglia D, Roberts J. Navigated osteotomies around the knee in 170 patients with osteoarthritis secondary to genu varum. Orthopedics.2005;28(10 Suppl):s1269-s1274.[13] Kim SJ, Koh YG, Chun YM, et al. Medial opening wedge high-tibial osteotomy using a kinematic navigation system versus a conventional method: a 1-year retrospective, comparative study. Knee Surg Sports Traumatol Arthrosc. 2009;17(2):128-134.[14] Akamatsu Y, Mitsugi N, Mochida Y, et al. Navigated opening wedge high tibial osteotomy improves intraoperative correction angle compared with conventional method. Knee Surg Sports Traumatol Arthrosc. 2012;20(3):586-593.[15] Reising K, Strohm PC, Hauschild O, et al. Computer-assisted navigation for the intraoperative assessment of lower limb alignment in high tibial osteotomy can avoid outliers compared with the conventional technique. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):181-188.[16] Ribeiro CH, Severino NR, Moraes de Barros Fucs PM. Opening wedge high tibial osteotomy: navigation system compared to the conventional technique in a controlled clinical study. Int Ortho.2014;38(8):1627-1631.[17] Lee DH, Han SB, Oh KJ, et al. The weight-bearing scanogram technique provides better coronal limb alignment than the navigation technique in open high tibial osteotomy. Knee.2014;21(2):451-455. [18] Na YG, Eom SH, Kim SJ, et al. The use of navigation in medial opening wedge high tibial osteotomy can improve tibial slope maintenance and reduce radiation exposure. Int Orthop. 2016;40(3):499-507. [19] Stanley JC, Robinson KG, Devitt BM, et al. Computer assisted alignment of opening wedge high tibial osteotomy provides limited improvement of radiographic outcomes compared to flouroscopic alignment. Knee. 2016;23(2):289-294. [20] Akamatsu Y, Kobayashi H, Kusayama Y, et al. Comparative study of opening-wedge high tibial osteotomy with and without a combined computed tomography-based and image-free navigation system. Arthroscopy. 2016;32(10): 2072-2081. [21] Schroter S, Ihle C, Elson DW, et al. Surgical accuracy in high tibial osteotomy: coronal equivalence of computer navigation and gap measurement. Knee Surg Sports Traumatol Arthrosc. 2016;24(11):3410-3417. [22] Chang J, Scallon G, Beckert M, et al. Comparing the accuracy of high tibial osteotomies between computer navigation and conventional methods. Comput Assist Surg (Abingdon). 2017; 22(1):1-8. [23] Fujisawa Y, Masuhara K, Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am. 1979;10(3):585-608.[24] 汪锡龙,尚希福,李国远,等. 个体化股骨远端外翻角度截骨技术在初次人工全膝关节置换术中的应用[J]. 中国修复重建外科杂志, 2015,29(1):27-30.[25] 王兴山,柳剑,顾建明,等. 改良闭合楔形胫骨高位截骨术治疗膝内翻畸形的疗效观察[J]. 中华关节外科杂志(电子版), 2016, 10(5):474-480.[26] Wang G,Zheng G, Keppler P, et al. Implementation, accuracy evaluation, and preliminary clinical trial of a CT-free navigation system for high tibial opening wedge osteotomy. Comput Aided Surg. 2005;10(2):73-85.[27] Kyung BS, Kim JG, Jang KM, et al. Are navigation systems accurate enough to predict the correction angle during high tibial osteotomy? Comparison of navigation systems with 3-dimensional computed tomography and standing radiographs. Am J Sports Med. 2013;41(10):2368-2374. [28] El-Azab H, Halawa A, Anetzberger H, et al. The effect of closed- and open-wedge high tibial osteotomy on tibial slope: a retrospective radiological review of 120 cases. J Bone Joint Surg Br. 2008;90(9):1193-1197. [29] Marti CB, Gautier E, Wachtl SW, et al. Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy. 2004;20(4):366-372. [30] Song EK, Seon JK, Park SJ, et al. Navigated open wedge high tibial osteotomy. Sports Med Arthrosc Rev. 2008;16(2): 84-90.[31] 韩旭东. 胫骨内侧平台后倾角放射学测量评价及其与膝骨关节炎的关系[D]. 广州:广州中医药大学, 2011.[32] Giffin JR, Vogrin T M, Zantop T, et al. Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med.2004;32(2):376-382. [33] Picardo NE, Khan W, Johnstone D. Computer-assisted navigation in high tibial osteotomy: a systematic review of the literature. Open Orthop J. 2012;6:305-312. |
| [1] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [2] | Chen Jinping, Li Kui, Chen Qian, Guo Haoran, Zhang Yingbo, Wei Peng. Meta-analysis of the efficacy and safety of tranexamic acid in open spinal surgery [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1458-1464. |
| [3] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [4] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Comparison of the short-term efficacy of extracorporeal shock wave therapy for middle-aged and elderly knee osteoarthritis: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1471-1476. |
| [5] | Wang Yongsheng, Wu Yang, Li Yanchun. Effect of acute high-intensity exercise on appetite hormones in adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1305-1312. |
| [6] | Kong Desheng, He Jingjing, Feng Baofeng, Guo Ruiyun, Asiamah Ernest Amponsah, Lü Fei, Zhang Shuhan, Zhang Xiaolin, Ma Jun, Cui Huixian. Efficacy of mesenchymal stem cells in the spinal cord injury of large animal models: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1142-1148. |
| [7] | Kong Lingbao, Lü Xin. Effect of implant selection and approach on support in the operation of posterolateral tibial plateau fractures [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 942-947. |
| [8] | Huang Dengcheng, Wang Zhike, Cao Xuewei. Intravenous, topical tranexamic acid alone or their combination in total knee arthroplasty: a meta-analysis of randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 948-956. |
| [9] | Li Yan, Wang Pei, Deng Donghuan, Yan Wei, Li Lei, Jiang Hongjiang. Electroacupuncture for pain control after total knee arthroplasty: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 957-963. |
| [10] | He Xiangzhong, Chen Haiyun, Liu Jun, Lü Yang, Pan Jianke, Yang Wenbin, He Jingwen, Huang Junhan. Platelet-rich plasma combined with microfracture versus microfracture in the treatment of knee cartilage lesions: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 964-969. |
| [11] | Hua Haotian, Zhao Wenyu, Zhang Lei, Bai Wenbo, Wang Xinwei. Meta-analysis of clinical efficacy and safety of antibiotic artificial bone in the treatment of chronic osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 970-976. |
| [12] | Zhan Fangbiao, Cheng Jun, Zou Xinsen, Long Jie, Xie Lizhong, Deng Qianrong. Intraoperative intravenous application of tranexamic acid reduces perioperative bleeding in multilevel posterior spinal surgery: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 977-984. |
| [13] | Zhong Yuanming, Wan Tong, Zhong Xifeng, Wu Zhuotan, He Bingkun, Wu Sixian. Meta-analysis of the efficacy and safety of percutaneous curved vertebroplasty and unilateral pedicle approach percutaneous vertebroplasty in the treatment of osteoporotic vertebral compression fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 456-462. |
| [14] | Li Yang, Zhang Mingyong. Meta-analysis of the effect of double Endobutton and clavicular hook plate on the treatment of acromioclavicular dislocation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 463-470. |
| [15] | Li Yanle, Yue Xiaohua, Wang Pei, Nie Weizhi, Zhang Junwei, Tan Yonghai, Jiang Hongjiang. Intramedullary nail fixation versus plate fixation in the treatment of displaced midshaft clavicular fractures in adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 471-476. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||