中国组织工程研究 ›› 2026, Vol. 30 ›› Issue (24): 6354-6364.doi: 10.12307/2026.234
• 组织构建循证医学 evidence-based medicine in tissue construction • 上一篇 下一篇
中国传统运动干预老年肌少症及其合并症:改善肌肉力量、质量及身体功能的Meta分析
褚 瑞1,李明明1,谢叶寿1,倪 涛2,杜依诺1
- 1安徽工程大学体育学院,安徽省芜湖市 241000;2常州大学体育学院,江苏省常州市 213000
-
收稿日期:2025-09-04修回日期:2025-10-19出版日期:2026-08-28发布日期:2026-02-04 -
通讯作者:谢叶寿,博士,教授,硕士生导师,安徽工程大学体育学院,安徽省芜湖市 241000 -
作者简介:褚瑞,男,2000年生,山东省枣庄市人,汉族,硕士,主要从事运动促进健康方面的研究。 -
基金资助:安徽省哲学社会科学规划项目(AHSKY2023D076),课题名称:县区级政府推动全民健身与全民健康深度融合研究,项目负责人:谢叶寿
Traditional Chinese sports intervene in sarcopenia and its complications in the elderly: a meta-analysis on improving muscle strength, mass, and physical function
Chu Rui1, Li Mingming1, Xie Yeshou1, Ni Tao2, Du Yinuo1
- 1School of Physical Education, Anhui Polytechnic University, Wuhu 241000, Anhui Province, China; 2Physical Education College of Changzhou University, Changzhou 213000, Jiangsu Province, China
-
Received:2025-09-04Revised:2025-10-19Online:2026-08-28Published:2026-02-04 -
Contact:Xie Yeshou, PhD, Professor, Master’s supervisor, School of Physical Education, Anhui Polytechnic University, Wuhu 241000, Anhui Province, China -
About author:Chu Rui, MS, School of Physical Education, Anhui Polytechnic University, Wuhu 241000, Anhui Province, China -
Supported by:Anhui Philosophy and Social Sciences Planning Project, No. AHSKY2023D076 (to XYS)
摘要:

文题释义:
肌少症及其合并症:为肌少症、肌少症性肥胖、肌少骨质疏松症、肌少骨量减少以及骨肌少症性肥胖的统称,以肌肉功能减退、骨密度降低及脂肪异常蓄积为主要特征,并且存在共同的病理机制与治疗靶点。
中国传统运动:指植根于中国传统哲学与医学理论(如经络学说、阴阳五行、导引养生学说等)的身体练习体系,主要涵盖太极拳、八段锦、易筋经、五禽戏等具体形式。中国传统运动的核心特征体现为身心协同,动作柔和舒缓,注重意念与呼吸的协调配合,属于中低强度的有氧运动范畴。
目的:肌少症及其合并症引发的肌肉功能减退、身体功能衰退等问题增加了老年人不良健康结局的风险,而目前针对中国传统运动干预该类疾病的系统证据尚显不足。因此,此次研究采用Meta分析方法系统评价中国传统运动对肌少症及其合并症的干预效果。
方法:遵循PRISMA指南,系统检索PubMed、Web of Science、Cochrane Library、CNKI、万方数据库,选择中国传统运动干预肌少症及其合并症的随机对照试验,试验组采用易筋经、太极拳、八段锦等中国传统运动中的一项或多项进行干预,对照组进行健康教育、常规护理或远程太极拳指导,结局指标包括握力、膝关节肌肉力量、四肢骨骼肌质量指数、坐立测试、步速、站立-行走计时测试与简易体能状况表。采用Revman 5.4和Stata 15.1软件进行Meta分析,通过亚组分析明确中国传统运动干预老年肌少症及其合并症效果的最佳方案参数。
结果:共纳入21项研究(n=1 313)。Meta分析结果显示,中国传统运动可有效改善患者的握力(MD=1.83,95%CI:1.65,2.01,P < 0.000 01)、
膝关节肌肉力量(MD=5.98,95%CI:3.85,8.11,P < 0.000 01)、四肢骨骼肌质量指数(MD=0.22,95%CI:0.10,0.34,P=0.000 4)、步速(MD=0.12,95%CI:0.09,0.16,P < 0.000 01)、坐立测试成绩(MD=1.92,95%CI:1.41,2.43,P < 0.000 01)、站立-行走计时测试成绩(SMD=
-1.00,95%CI:-1.25,-0.74,P < 0.000 01)以及简易体能状况成绩(MD=1.12,95%CI:0.77,1.46,P < 0.000 01)。亚组分析结果显示,在提升此类患者握力方面,易筋经(干预> 12周、每周干预> 3次、单次运动≤30 min)的效果最佳;在改善患者四肢骨骼肌质量指数方面,八段锦(干预12周、每周干预≤3次、单次运动> 30 min)的效果最优;太极拳(干预> 12周、每周干预> 3次、单次运动≤30 min)或八段锦(干预周期12周、每周干预3次、单次运动> 30 min)均能显著提升患者步速;在改善患者坐立测试成绩方面,易筋经(干预8周、每周干预5次、单次运动≤40 min)的效果最佳;八段锦(干预> 12周、每周干预≤3次、单次运动> 30 min且≤40 min)对站立-行走测试成绩的改善最显著。
结论:中国传统运动可有效改善老年肌少症及其合并症患者的握力、膝关节肌肉力量、四肢骨骼肌质量及身体功能,并且不同干预参数条件下具有特异性效应,建议临床根据目标结局制定个性化运动处方。
https://orcid.org/0009-0000-0770-4447 (褚瑞)
中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
中图分类号:
引用本文
褚 瑞, 李明明, 谢叶寿, 倪 涛, 杜依诺. 中国传统运动干预老年肌少症及其合并症:改善肌肉力量、质量及身体功能的Meta分析[J]. 中国组织工程研究, 2026, 30(24): 6354-6364.
Chu Rui, Li Mingming, Xie Yeshou, Ni Tao, Du Yinuo. Traditional Chinese sports intervene in sarcopenia and its complications in the elderly: a meta-analysis on improving muscle strength, mass, and physical function[J]. Chinese Journal of Tissue Engineering Research, 2026, 30(24): 6354-6364.
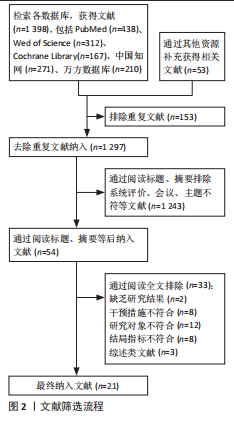
文献筛选流程详见图2。
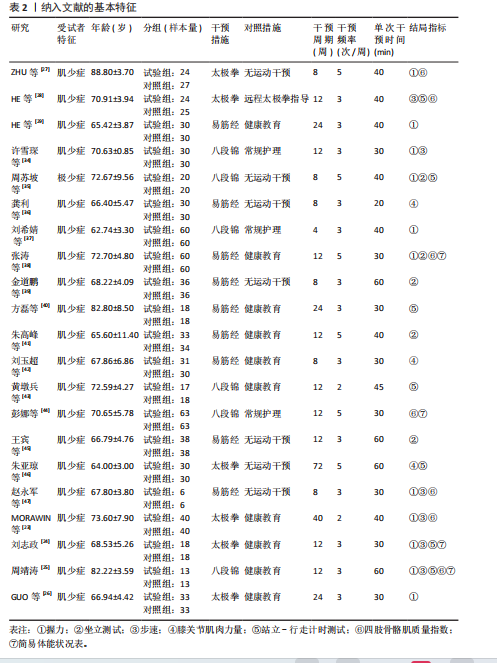
2.2 纳入文献的特征 表2系统归纳了纳入文献的受试者特征、试验分组设计、运动干预方案以及用于评估老年肌少症及其合并症干预效果的结局指标。21项研究均为随机对照试验,试验受试者均为患有肌少症或合并骨质疏松的肌少骨质疏松症、合并肥胖的肌少症性肥胖与同时出现肥胖并伴有骨量减少的骨肌少症性肥胖的老年人,平均年龄70.3岁,符合老年肌少症研究对象的典型年龄特征;其中有19项研究所纳入的受试者年龄在65-75岁之间,表明该年龄段肌少症及其合并症患者是当前中国传统运动干预研究的主要人群。
纳入文献的运动干预方案主要包含运动方式、干预周期、运动频率和运动时间4个方面,
仅有少量研究对运动干预所采用的强度进行了说明。6项研究采用太极拳[23-24,26-28,46]、9项研究采用易筋经[29,36,38-42,45,47]、6项研究采用八段锦作为运动干预手段[25,34-35,37,43-44];干预周期介于4-72周,其中12周的运动周期占比最高,达45.5%(10项);每周运动频率为2-5次,每周3次的运动频率占比达63.6%(14项);单次运动干预时长为20-60 min,每次30 min的运动时长占比为40.9%(9项)。
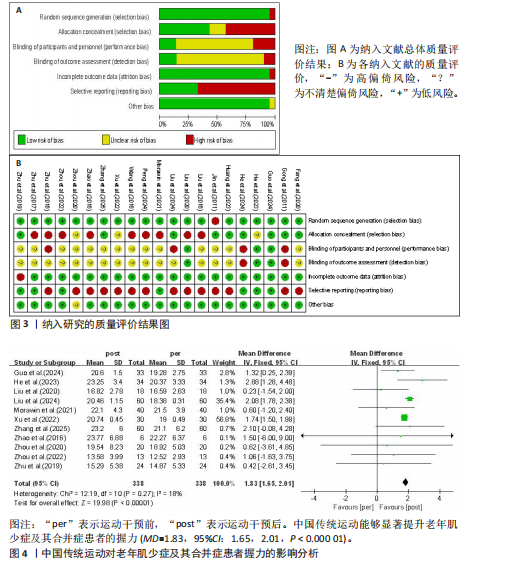
2.3 纳入研究的偏倚风险 纳入文献的偏倚风险评估结果见图3,其中1篇文献判定为A级,21篇文献判定为B级,文献总体质量良好。
2.4 Meta分析结果
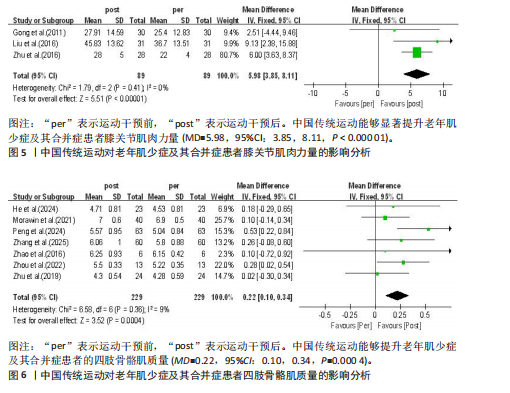
2.4.1 中国传统运动对老年肌少症及其合并症患者握力的影响 有11项随机对照试验报告了中国传统运动对老年肌少症及其合并症患者握力的干预效果,共纳入研究对象338例[23-27,29,34-35,37-38,47]。异质性检验结果显示各研究间的异质性较低(I2=18%,P=0.27),采用固定效应模型;采用Egger’s检验评估所纳入研究的发表偏倚,结果显示P=0.203,表明此次纳入的研究不存在发表偏倚,结果具有可靠性。Meta分析结果显示,中国传统运动能够显著提升老年肌少症及其合并症患者的握力(MD=1.83,95%CI:1.65,2.01,P < 0.000 01),见图4。
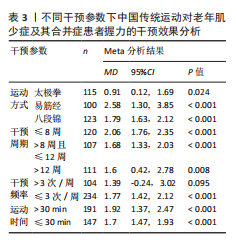
针对中国传统运动在不同干预参数条件下对患者握力的干预效应,亚组分析结果显示:根据效应值与P值比较,在不同的中国传统运动中,易筋经的改善效果最佳(MD=2.58,95%CI:1.30,3.85,P < 0.001);在运动周期方面,≤8周的干预效果最佳(MD=2.06,95%CI:1.76,2.35,P < 0.001),每周干预≤3次的改善
效果最佳(MD=1.77,95%CI:1.42,2.12,P < 0.001),单次运动> 30 min的改善效果最佳(MD=1.92,95%CI:1.37,2.47,P < 0.001),见表3。
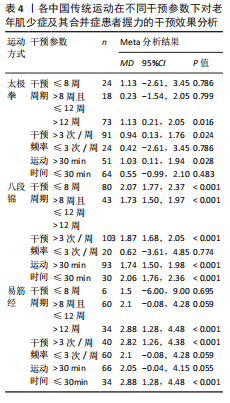
为进一步提高运动处方制定的针对性,此次研究对各类中国传统运动在不同干预参数条件下对患者握力改善的效应量进行了亚组分析,结果显示:对于太极拳,干预> 12周、每周干预> 3次且单次运动> 30 min的改善效果最佳;对于八段锦,干预≤8周、每周干预> 3次且单次运动≤30 min的改善效果最佳;对于易筋经,干预> 12周、每周干预> 3次且单次运动≤30 min的改善效果最佳,见表4。
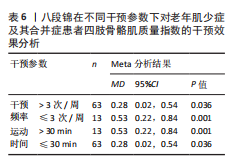
2.4.2 中国传统运动对老年肌少症及其合并症患者膝关节肌肉力量的影响 有3项随机对照试验报告了中国传统运动对老年肌少症及其合并症患者膝关节肌肉力量的干预效果,共纳入研究对象89例[36,42,46]。 异质性检验结果显示各研究间不存在异质性(I2=0%,P=0.41),采用固定效应模型;采用Egger’s检验评估所纳入研究的发表偏倚,结果显示P=0.970,表明此次纳入的
研究不存在发表偏倚,结果具有可靠性。Meta分析结果显示,中国传统运动能够显著提升老年肌少症及其合并症患者膝关节肌肉力量(MD=5.98,95%CI:3.85,8.11,P < 0.000 01),见图5。鉴于纳入研究在干预参数方面具有较高的同质性,故未对该指标进行亚组分析。
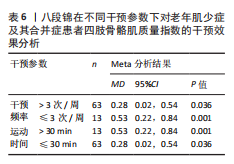
2.4.3 中国传统运动对老年肌少症及其合并症患者四肢骨骼肌质量指数的影响 7项随机对照试验报告了中国传统运动对老年肌少症及其合并症患者四肢骨骼肌质量指数的影响,共纳入研究对象229例[23,25,27-28,38,44,47]。异质性检验结果显示各研究间异质性较低(I2=9%,P=0.36),采用固定效应模型;采用Egger’s检验评估所纳入研究的发表偏倚,结果显示P=0.961,表明此次纳入的研究不存在发表偏倚,结果具有可靠性。Meta分析结果显示,中国传统运动能够提升老年肌少症及其合并症患者的四肢骨骼肌质量(MD=0.22,95%CI:0.10,0.34,P=0.000 4),见图6。
初步对中国传统运动整体在不同干预参数下对老年肌少症及其合并症患者四肢骨骼肌质量指数的干预效果进行比对,亚组分析结果显示:根据效应值与P值比较结果,在各类中国传统运动中八段锦的改善效果最佳(MD=0.38,95%CI:0.18,0.58,P < 0.001);运动> 8周且≤12周(MD=0.33,95%CI:0.17,0.49,P < 0.001)、每周干预≤3次(MD=0.27,95%CI:0.09,0.46,P=0.004)、单次运动> 30 min (MD=0.38,95%CI:0.16-0.60,P < 0.001)提升患者四肢骨骼肌质量的效果最佳,见表5。
由于太极拳与易筋经在初步亚组分析中显示对患者四肢骨骼肌质量指数的改善并不显著,因此,亚组分析仅针对八段锦在不同干预
参数下产生的效应量进行分析,结果显示:运动干预12周、每周干预≤3次及单次运动> 30 min对患者四肢骨骼肌质量指数的改善效果最佳,见表6。需注意的是,由于相关研究数量较少,此次研究纳入的八段锦干预周期均为12周,因此无法比较不同运动干预周期下的效果差异。
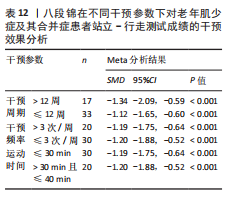
2.4.4 中国传统运动对老年肌少症及其合并症患者步速的影响 有6项随机对照试验报告了中国传统运动对老年肌少症及其合并症患者步速的干预效果,共纳入研究对象130例[23-25,28,34,47]。异质性检验结果显示各研究间存在中等异质性(I2=0%,P=0.60),采用固定效应模型;采用Egger’s检验评估所纳入研究的发表偏倚,结果显示P=0.504,表明此次纳入的研究不存在发表偏倚,结果具有可靠性。Meta分析结果显示,中国传统运动能够显著提升老年肌少症及其合并症患者的步速(MD=0.12,95%CI:0.09,0.16,P < 0.000 01),见图7。
初步对中国传统运动整体在不同干预参数下对老年肌少症及其合并症患者步速的干预效果进行比对,亚组分析结果显示,根据效应值与P值,在不同的中国传统运动中,太极拳(MD=0.11,95%CI:0.06,0.16,P < 0.001)与八段锦(MD=0.13,95%CI:0.09,0.18,P < 0.001)均可显著提升患者步速;运动> 12周(MD=0.13,95%CI:0.09,0.16,P < 0.001)、每周> 3次(MD=0.13,95%CI:0.09,0.16,P < 0.001)、单次运动> 30 min(MD=0.12,95%CI:0.07,0.18,P < 0.001)与≤30 min(MD=0.12,95%CI:0.08,0.16,P < 0.001)的干预效果最佳,见表7。
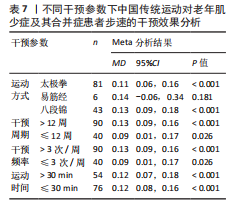
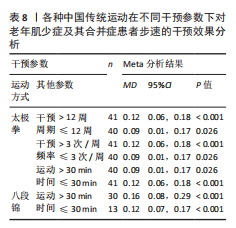
由于易筋经在初步亚组分析中显示对患者步速的改善并不显著,因此亚组分析仅针对八段锦与太极拳在不同干预参数下产生的效应量进行分析,结果显示:八段锦运动干预12周、每周干预3次及单次运动> 30 min对患者步速的改善效果最佳;太极拳干预> 12周、每周干预> 3次、单次运动≤30 min对患者步速的改善效果最佳,见表8。需注意的是,由于相关研究数量较少,此次研究纳入的八段锦干预周期均为12周,干预频率均为每周3次,因此无法比较不同运动干预周期与频率下的效果差异。
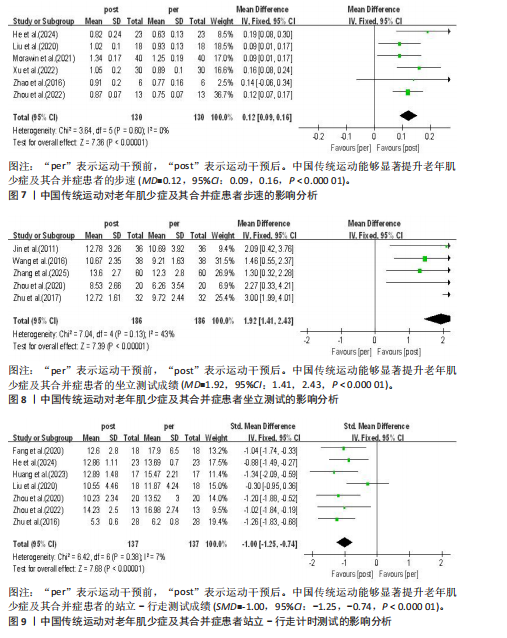
2.4.5 中国传统运动对老年肌少症及其合并症患者坐立测试的影响 有5项随机对照试验报告了中国传统运动对老年肌少症及其合并症患者坐立测试的干预效果,共纳入研究对象186例[35,38-39,41,45]。异质性检验结果显示各研究间存在中等异质性(I2=43%,P=0.13),采用固定效应模型;采用Egger’s检验评估所纳入研究的发表偏倚,结果显示P=0.691,表明此次纳入的研究不存在发表偏倚,结果具有可靠性。Meta分析结果显示,中国传统运动能够显著提升老年肌少症及其合并症患者的坐立测试成绩(MD=1.92,95%CI:1.41,2.43,P < 0.000 01),见图8。
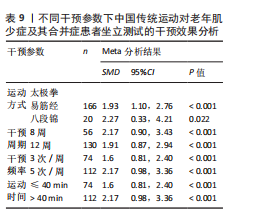
初步对中国传统运动整体在不同干预参数下对老年肌少症及其合并症患者坐立测试的干预效果进行比对,亚组分析结果显示,根据效应值与P值,在不同的中国传统运动中,易筋经(MD=1.93,95%CI:1.10,2.76,P < 0.001)八段锦(MD=2.27,95%CI:0.33,4.21,P=0.022)均可显著提升老年肌少症及其合并症患者的坐立测试成绩;8周干预周期(MD=2.17,95%CI:0.90,3.43,P < 0.001)、每周干预5次(MD=2.17,95%CI:0.98,3.36,P < 0.001)与单次运动> 40 min(MD=2.17,95%CI:0.98,3.36,P < 0.001)对老年肌少症及其合并症坐立测试成绩效果的改善效果最佳,见表9。
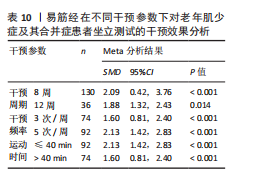
由于相关研究数量受限,在分析中国传统运动对老年肌少症及其合并症患者坐立测试成绩的效应量时,仅成功纳入1项采用八段锦进行干预的研究,未纳入采用太极拳进行干预的研究,因此亚组分析仅针对易筋经在不同干预参数下产生的效应量进行分析,结果显示:易筋经干预8周、每周干预5次及单次运动≤40 min对老年肌少症及其合并症患者坐立测试成绩的改善效果最佳,见表10。
2.4.6 中国传统运动对老年肌少症及其合并症患者站立-行走计时测试的影响 有7项随机对照试验报告了中国传统运动对老年肌少症及其合并症患者站立-行走测试的干预效果,共纳入研究对象137例[24-25,28,35,40,43,46]。由于所纳入的研究测试中对站立-行走测试所采用的计量单位不同,因此该项分析采用SMD计算效应量。异质性检验结果显示各研究间的异质性较低(I2=7%,P=0.38),采用固定效应模型;采用Egger’s检验评估纳入研究的发表偏倚,结果显示P=0.874,表明此次纳入研究不存在发表偏倚,结果具有可靠性。Meta分析结果显示,中国传统运动能够显著提升老年肌少症及其合并症患者的站立-行走测试成绩(SMD=-1.00,95%CI:-1.25,-0.74,P < 0.000 01),见图9。
初步对中国传统运动整体在不同干预参数下对老年肌少症及其合并症患者站立-行走测试成绩的干预效果进行比对,亚组分析结果显示,根据效应值与P值,在不同的中国传统运动中,八段锦(SMD=-1.19,95%CI:-1.62,-0.76,P < 0.001)可显著提升老年肌少症及其合并症患者的站立-行走测试成绩;干预≤12周(SMD=-1.08,95%CI:-1.38,-0.79,P < 0.001)、每周干预≤3次(SMD=-1.12,95%CI:-1.45,-0.78,P < 0.001)与单次运动时间≤30 min(SMD=-1.19,95%CI:-1.79,-0.64, P < 0.001)改善老年肌少症及其合并症患者站立-行走测试成绩的效果最佳,见表11。
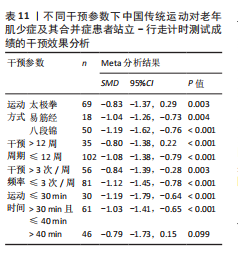
由于太极拳在初步亚组分析中对老年肌少症及其合并症患者站立-行走测试成绩的改善并不显著,并且仅纳入了一项采用易筋经作为干预手段的相关研究,因此亚组分析仅针对八段锦在不同干预参数下产生的效应量进行分析,结果显示:八段锦干预> 12周、每周干
预≤3次及单次运动> 30 min且≤40 min对老年肌少症及其合并症患者站立-行走测试成绩的改善效果最佳,见表12。
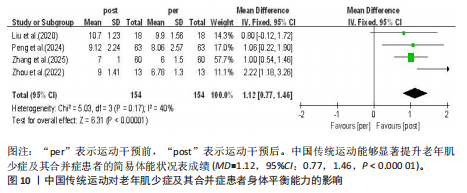
2.4.7 中国传统运动对老年肌少症及其合并症患者简易体能状况表成绩的影响 4项随机对照试验系统探讨了中国传统运动对老年肌少症及其合并症患者简易机体功能评估成绩的干预效果,涉及研究对象154例[24-25,38,44]。
异质性检验结果显示各研究间存在中等异质性(I2=40%,P=0.17),采用固定效应模型;采用
Egger’s检验评估所纳入研究的发表偏倚,结果显示P=0.496,表明各研究不存在发表偏倚,结果具有可靠性。Meta分析结果显示,中国传统运动能够显著提升老年肌少症及其合并症患者的简易体能状况表成绩(MD=1.12,95%CI:0.77,1.46,P < 0.000 01),见图10。
鉴于纳入研究在干预参数方面具有较高的同质性,故未对该指标进行亚组分析。
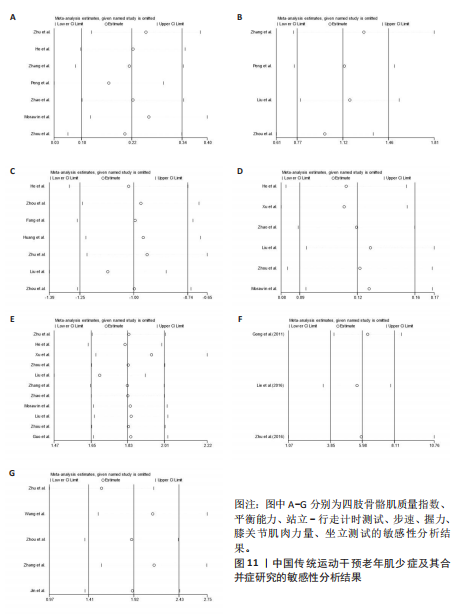
2.5 敏感性分析 采用逐一剔除法对各项结局指标进行敏感性分析,结果显示各研究的合并效应量未发生显著变化(图11),表明此次Meta分析的结果具有较高的稳健性。
| [1] CRUZ-JENTOFT AJ, BAEYENS JP, BAUER JM, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412-423. [2] CAO L, MORLEY JE. Sarcopenia Is Recognized as an Independent Condition by an International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) Code. J Am Med Dir Assoc. 2016;17(8):675-677. [3] GAO Y, LIU D, XIAO Q, et al. Exploration of Pathogenesis and Cutting-Edge Treatment Strategies of Sarcopenia: A Narrative Review. Clin Interv Aging. 2025;20:659-684. [4] LIU P, HAO Q, HAI S, et al. Sarcopenia as a predictor of all-cause mortality among community-dwelling older people: A systematic review and meta-analysis. Maturitas. 2017;103:16-22. [5] NIELSON CM, SRIKANTH P, ORWOLL ES. Obesity and fracture in men and women: an epidemiologic perspective. J Bone Miner Res. 2012;27(1):1-10. [6] ORMSBEE MJ, PRADO CM, ILICH JZ, et al. Osteosarcopenic obesity: the role of bone, muscle, and fat on health. J Cachexia Sarcopenia Muscle. 2014;5(3):183-192. [7] 孙嘉禾,史冀鹏,朱天瑞,等.运动对肌少症及其合并症老年人影响的Meta分析[J].中国组织工程研究,2026,30(4):997-1007. [8] KIM TN, PARK MS, YANG SJ, et al. Prevalence and determinant factors of sarcopenia in patients with type 2 diabetes: the Korean Sarcopenic Obesity Study. Diabetes Care. 2010;33(7):1497-1499. [9] ZHANG H, WANG J, XI J, et al. Functional fitness and risk factors of older patients with diabetes combined with sarcopenia and/or frailty: A cross-sectional study. Nursing open. 2024;11(1): e2042-e2042. [10] PÉREZ-ZEPEDA MU, SGARAVATTI A, DENT E. Sarcopenia and post-hospital outcomes in older adults: A longitudinal study. Arch Gerontol Geriatr. 2017;69:105-109. [11] GASKIN FS, FARR SA, BANKS WA, et al. Ghrelin-induced feeding is dependent on nitric oxide. Peptides. 2003;24(6):913-918. [12] WU PY, HUANG KS, CHEN KM, et al. Exercise, Nutrition, and Combined Exercise and Nutrition in Older Adults with Sarcopenia: A Systematic Review and Network Meta-analysis. Maturitas. 2021;145:38-48. [13] CHEN HT, CHUNG YC, CHEN YJ, et al. Effects of Different Types of Exercise on Body Composition, Muscle Strength, and IGF-1 in the Elderly with Sarcopenic Obesity. J Am Geriatr Soc. 2017;65(4): 827-832. [14] HASSAN BH, HEWITT J, KEOGH JW, et al. Impact of resistance training on sarcopenia in nursing care facilities: A pilot study. Geriatr Nurs. 2016;37(2):116-121. [15] DE SÁ SOUZA H, DE MELO CM, PIOVEZAN RD, et al. Resistance Training Improves Sleep and Anti-Inflammatory Parameters in Sarcopenic Older Adults: A Randomized Controlled Trial. Int J Environ Res Public Health. 2022;19(23):16322. [16] ZHANG Y, HUANG L, SU Y, et al. The Effects of Traditional Chinese Exercise in Treating Knee Osteoarthritis: A Systematic Review and Meta-Analysis. PLoS One. 2017;12(1):e0170237. [17] 贾冕,王正珍,李博文.中医运动处方的起源与发展[J].体育科学,2017,37(10):65-71,89. [18] ZHOU Z, ZHOU R, LI K, et al. Effects of tai chi on physiology, balance and quality of life in patients with type 2 diabetes: A systematic review and meta-analysis. J Rehabil Med. 2019;51(6):405-417. [19] ZHANG Y, LIU H, ZHOU L, et al. Applying Tai Chi as a rehabilitation program for stroke patients in the recovery phase: study protocol for a randomized controlled trial. Trials. 2014;15:484. [20] WU S, LU Z, LI Z, et al. The efficacy of Tai Chi for intervention treatment of myocardial infarction: A protocol for systematic review and meta-analysis. Medicine (Baltimore). 2021;100(46):e27584. [21] ZHENG G, CHEN B, FANG Q, et al. Primary prevention for risk factors of ischemic stroke with Baduanjin exercise intervention in the community elder population: study protocol for a randomized controlled trial. Trials. 2014;15:113. [22] BARRADO-MARTÍN Y, HEWARD M, POLMAN R, et al. People living with dementia and their family carers’ adherence to home-based Tai Chi practice. Dementia (London). 2021;20(5):1586-1603. [23] MORAWIN B, TYLUTKA A, CHMIELOWIEC J, et al. Circulating Mediators of Apoptosis and Inflammation in Aging; Physical Exercise Intervention. Int J Environ Res Public Health. 2021; 18(6):3165. [24] 刘志政.太极拳对增龄性肌肉减少症的干预效果研究[D].济宁:曲阜师范大学,2020. [25] 周靖涛.八段锦对老年肌少症的干预效果研究[D].湘潭:湖南科技大学,2022. [26] GUO H, CAO J, HE S, et al. Quantifying the Enhancement of Sarcopenic Skeletal Muscle Preservation Through a Hybrid Exercise Program: Randomized Controlled Trial. JMIR Aging. 2024;7: e58175. [27] ZHU YQ, PENG N, ZHOU M, et al. Tai Chi and whole-body vibrating therapy in sarcopenic men in advanced old age: a clinical randomized controlled trial. Eur J Ageing. 2019;16(3):273-282. [28] HE S, MENG D, WEI M, et al. Proposal and validation of a new approach in tele-rehabilitation with 3D human posture estimation: a randomized controlled trial in older individuals with sarcopenia. BMC Geriatr. 2024;24(1):586. [29] HE S, WEI M, MENG D, et al. Self-determined sequence exercise program for elderly with sarcopenia: A Randomized controlled trial with clinical assistance from explainable artificial intelligence. Arch Gerontol Geriatr. 2024;119: 105317. [30] HUANG CY, MAYER PK, WU MY, et al. The effect of Tai Chi in elderly individuals with sarcopenia and frailty: A systematic review and meta-analysis of randomized controlled trials. Ageing Res Rev. 2022;82:101747. [31] NIU K, LIU YL, YANG F, et al. Efficacy of traditional Chinese exercise for sarcopenia: A systematic review and meta-analysis of randomized controlled trials. Front Neurosci. 2022;16:1094054. [32] LIBERATI A, ALTMAN DG, TETZLAFF J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ. 2009;339:b2700. [33] HIGGINS JP, ALTMAN DG, GØTZSCHE PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. [34] 许雪琛,郭恒群,林健.八段锦联合抗阻运动干预老年肌少症30例[J].福建中医药,2022, 53(11):60-62. [35] 周苏坡,邹颖,孙小斐,等.八段锦预防老年肌少症人群跌倒的研究[J].体育科技,2020,41(6): 27-28+30. [36] 龚利,严隽陶,刘玉超,等.推拿功法易筋经对老年骨骼肌减少症患者等速肌力的影响[J].上海中医药大学学报,2011,25(3):55-58. [37] 刘希婧,华馨,严莉,等.以护理为导向的八段锦联合杵针八阵穴疗法对肝硬化肌少症病人的干预效果[J].循证护理,2024,10(12):2177-2180. [38] 张涛,马天翼,骆丽,等.易筋经对老年肌少症患者肌肉力量及慢性炎症的影响[J].南京中医药大学学报,2025,41(3):399-404. [39] 金道鹏,徐俊,赵吉忠,等.推拿功法易筋经对骨骼肌减少症患者日常活动能力及体质的影响[J].中国中医药信息杂志,2011,18(1):14-16. [40] 方磊,李振瑞,陶旭辰,等.易筋经对老年骨骼肌减少症平衡障碍患者跌倒风险影响的临床研究[J].中国康复医学杂志,2020,35(3):319-323. [41] 朱高峰,沈志方,沈清河,等.易筋经对老年人骨骼肌肌力的影响(英文)[J].Journal of Acupuncture and Tuina Science. 2017,15(6):434-439. [42] 刘玉超,严隽陶,王振裕,等.易筋经对老年骨骼肌减少症骨骼肌收缩功能的影响[J].上海中医药大学学报,2016,30(5):42-45. [43] 黄墩兵,林忠华,姜财,等.全身振动训练联合八段锦运动对老年肌少症患者姿势稳定性的影响[J].中国康复,2023,38(7):430-433. [44] 彭娜,苗笛,王红,等.八段锦联合血流限制训练对老年肌少症的应用效果研究[J].中华保健医学杂志,2024,26(3):332-335. [45] 王宾,马士荣,胡莺.健身气功易筋经锻炼对骨骼肌减少症患者康复效果的影响[J].中国老年学杂志,2016,36(4):898-899. [46] 朱亚琼,彭楠,周明.太极拳对老年人下肢肌力及功能的影响[J].中国中西医结合杂志,2016, 36(1):49-53. [47] 赵永军,张育民,郭艳花,等.推拿结合抗阻运动对骨骼肌衰减症患者日常生活活动能力的影响[J].中国康复医学杂志,2016,31(9):989-994. [48] PAPADOPOULOU SK. Sarcopenia: A Contemporary Health Problem among Older Adult Populations. Nutrients. 2020;12(5):1293. [49] YU X, CHAU JPC, HUO L. The effectiveness of traditional Chinese medicine-based lifestyle interventions on biomedical, psychosocial, and behavioral outcomes in individuals with type 2 diabetes: A systematic review with meta-analysis. Int J Nurs Stud. 2018;80:165-180. [50] CHEN J, ZHOU R, FENG Y, et al. Molecular mechanisms of exercise contributing to tissue regeneration. Signal Transduct Target Ther. 2022; 7(1):383. [51] JÄGER S, HANDSCHIN C, ST-PIERRE J, et al. AMP-activated protein kinase (AMPK) action in skeletal muscle via direct phosphorylation of PGC-1alpha. Proc Natl Acad Sci U S A. 2007;104(29):12017-12022. [52] JUNG S, KIM K. Exercise-induced PGC-1α transcriptional factors in skeletal muscle. Integr Med Res. 2014;3(4):155-160. [53] ZHOU M, LIAO H, SREEPADA LP, et al. Tai Chi Improves Brain Metabolism and Muscle Energetics in Older Adults. J Neuroimaging. 2018;28(4):359-364. [54] 史仍飞.骨骼肌生长与适应的机械信号与途径[J].中国组织工程研究与临床康复,2010,14(24): 4507-4511. [55] ZHU WG, THOMAS AC, WILSON GM, et al. Identification of a resistance-exercise-specific signalling pathway that drives skeletal muscle growth. Nat Metab. 2025;7(7):1404-1423. [56] FENG L, LI B, YONG SS, et al. Exercise and nutrition benefit skeletal muscle: From influence factor and intervention strategy to molecular mechanism. Sports Med Health Sci. 2024;6(4):302-314. [57] LAI CC, TU YK, WANG TG, et al. Effects of resistance training, endurance training and whole-body vibration on lean body mass, muscle strength and physical performance in older people: a systematic review and network meta-analysis. Age Ageing. 2018;47(3):367-373. [58] LU L, MAO L, FENG Y, et al. Effects of different exercise training modes on muscle strength and physical performance in older people with sarcopenia: a systematic review and meta-analysis. BMC Geriatr. 2021;21(1):708. [59] MALICDAN MC, NOGUCHI S, NONAKA I, et al. Lysosomal myopathies: an excessive build-up in autophagosomes is too much to handle. Neuromuscul Disord. 2008;18(7):521-529. [60] BAMMAN MM, SHIPP JR, JIANG J, et al. Mechanical load increases muscle IGF-I and androgen receptor mRNA concentrations in humans. Am J Physiol Endocrinol Metab. 2001;280(3):E383-390. [61] SOMMER A, KORDOWSKI F, BÜCH J, et al. Phosphatidylserine exposure is required for ADAM17 sheddase function. Nat Commun. 2016;7:11523. [62] ZADA FSM, NASERI K, ZALMAI MR. Effects of exercise training on blood circulation system. Sprin J Arts Humanit Soc Sci. 2024;3(5):87-90. [63] SCHOENFELD BJ. Science and development of muscle hypertrophy. Human Kinetics; 2020. [64] CUI H, WANG Z, WU J, et al. Chinese expert consensus on prevention and intervention for elderly with sarcopenia (2023). Aging Med (Milton). 2023;6(2):104-115. [65] HÄKKINEN K, ALEN M, KALLINEN M, et al. Neuromuscular adaptation during prolonged strength training, detraining and re-strength-training in middle-aged and elderly people. Eur J Appl Physiol. 2000;83(1):51-62. [66] LEMMER JT, HURLBUT DE, MARTEL GF, et al. Age and gender responses to strength training and detraining. Med Sci Sports Exerc. 2000;32(8): 1505-1512. [67] 周明,彭楠,黎春华,等.太极拳训练对老年人下肢骨骼肌肌力的影响趋势分析[J].中国康复医学杂志,2014,29(11):1050-1054. [68] MARX W, VERONESE N, KELLY JT, et al. The Dietary Inflammatory Index and Human Health: An Umbrella Review of Meta-Analyses of Observational Studies. Adv Nutr. 2021;12(5):1681-1690. [69] PAN L, XIE W, FU X, et al. Inflammation and sarcopenia: A focus on circulating inflammatory cytokines. Exp Gerontol. 2021;154:111544. [70] 周术锋,王芳,彭永,等.12周太极拳联合渐进抗阻运动对膝关节骨性关节炎患者微循环功能及炎性因子的影响[J].中国体育科技,2023, 59(3):44-49. [71] 陈辉,周亚娜.太极拳锻炼对老年高血压患者血清TNF-α和IL-6水平的影响[J].中国老年学杂志,2012,32(11):2361-2362. [72] LADAWAN S, KLAROD K, PHILIPPE M, et al. Effect of Qigong exercise on cognitive function, blood pressure and cardiorespiratory fitness in healthy middle-aged subjects. Complement Ther Med. 2017;33:39-45. [73] LAURENT MR, DUBOIS V, CLAESSENS F, et al. Muscle-bone interactions: From experimental models to the clinic? A critical update. Mol Cell Endocrinol. 2016;432:14-36. [74] 刘魏,童培建,肖鲁伟,等.益骨汤口服联合太极拳锻炼治疗老年性骨质疏松症肾阳虚证[J].中医正骨,2018,30(11):6-12. [75] CHO MR, LEE S, SONG SK. A Review of Sarcopenia Pathophysiology, Diagnosis, Treatment and Future Direction. J Korean Med Sci. 2022;37(18):e146. [76] 王素素,李丽凤,张一民.运动干预老年人肌少症近10年研究进展及国际热点可视化分析[J].中国组织工程研究,2022,26(14):2223-2230. [77] COCHET C, BELLONI G, BUONDONNO I, et al. The Role of Nutrition in the Treatment of Sarcopenia in Old Patients: From Restoration of Mitochondrial Activity to Improvement of Muscle Performance, a Systematic Review. Nutrients. 2023;15(17):3703. [78] CAVALLUCCI V, PANI G. The Leucine Catabolite and Dietary Supplement β-Hydroxy-β-Methyl Butyrate (HMB) as an Epigenetic Regulator in Muscle Progenitor Cells. Metabolites. 2021; 11(8):512. [79] ERICKSON KI, VOSS MW, PRAKASH RS, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A. 2011;108(7):3017-3022. [80] 欧春影,李传玲,安晓雷,等.急性脑梗死患者血清BDNF、IL-6和TNF-α含量与血管性认知障碍关系的临床分析[J].中华脑科疾病与康复杂志(电子版),2019,9(3):163-167. [81] DICKSTEIN R, DEUTSCH JE. Motor imagery in physical therapist practice. Phys Ther. 2007;87(7): 942-953. [82] TAO J, CHEN X, EGOROVA N, et al. Tai Chi Chuan and Baduanjin practice modulates functional connectivity of the cognitive control network in older adults. Sci Rep. 2017;7:41581. [83] GUO LY, YANG CP, YOU YL, et al. Underlying mechanisms of Tai-Chi-Chuan training for improving balance ability in the elders. Chin J Integr Med. 2014;20(6):409-415. [84] 刘玉超,王振裕,方磊,等.易筋经对老年骨骼肌减少症者动态平衡能力的影响[J].河北中医药学报,2014,29(4):9-11. [85] XIAO Y, LUO Q, YU Y, et al. Effect of baduanjin on the fall and balance function in middle-aged and elderly people: A protocol for systematic review and meta-analysis. Medicine (Baltimore). 2021;100(37):e27250. [86] 翟凤鸣,陈玉娟,黄志芳,等.八段锦运动对老年人生理功能的影响[J].中国老年学杂志, 2013,33(6):1402-1404. [87] 王利凯,萧禹,王立童.经皮耳迷走神经电刺激联合经颅直流电刺激对脑卒中患者上肢功能的影响[J].中国康复,2023,38(11):659-663. [88] NIU Y, BURANARUGSA R, KUHIRUNYARATN P. Comparing the Effects of Bafa Wubu Tai Chi and Traditional He-Style Tai Chi Exercises on Physical Health Risk Factors in Overweight Male College Students: A Randomized Controlled Trial. Int J Environ Res Public Health. 2023;20(14):6323. [89] AN B, DAI K, ZHU Z, et al. Baduanjin alleviates the symptoms of knee osteoarthritis. J Altern Complement Med. 2008;14(2):167-174. [90] WANG C, LIANG J, SI Y, et al. The effectiveness of traditional Chinese medicine-based exercise on physical performance, balance and muscle strength among older adults: a systematic review with meta-analysis. Aging Clin Exp Res. 2022;34(4):725-740. [91] DE ANGELIS C, DRAZEN JM, FRIZELLE FA, et al. Clinical trial registration: a statement from the International Committee of Medical Journal Editors. Lancet. 2004;364(9438):911-912. |
| [1] | 张庆彤, 陈乐琴, 刘昶, 陈昱廷, 郭睿武. 内源性大麻素系统调控运动动机的神经机制[J]. 中国组织工程研究, 2026, 30(在线): 1-11. |
| [2] | 李智斐, 韩 斌, 柳秋丽, 张展鸣, 韦浩凯, 左匡时, 张翼升. 基于动作捕捉技术分析神经根型颈椎病患者的颈椎运动特征[J]. 中国组织工程研究, 2026, 30(9): 2286-2293. |
| [3] | 何易祥, 乔万佳, 王文己. 氨甲环酸与氨基己酸在全髋和全膝关节置换过程中有效性和安全性的Meta分析[J]. 中国组织工程研究, 2026, 30(9): 2361-2369. |
| [4] | 刘金龙, 阿卜杜吾普尔•海比尔, 白 臻, 苏丹阳, 苗 鑫, 李 菲, 杨晓鹏. 不同非手术方法治疗青少年特发性脊柱侧凸效果的系统综述与网状Meta分析[J]. 中国组织工程研究, 2026, 30(9): 2370-2379. |
| [5] | 高 峰, 张 俊, 余文君, 单于玉婧, 赵 乐, 胡雨婷, 王俊华, 刘永富. 佩戴腕手矫形器对脑卒中患者手功能障碍作用的Meta分析[J]. 中国组织工程研究, 2026, 30(8): 2124-2131. |
| [6] | 潘 冬, 杨加玲, 田 卫, 王东济, 朱 政, 马文超, 刘 娜, 付常喜. 抗阻运动激活衰老大鼠骨骼肌卫星细胞:脂联素受体1途径的作用[J]. 中国组织工程研究, 2026, 30(7): 1736-1746. |
| [7] | 曹 涌, 滕虹良, 邰鹏飞, 李骏达, 朱腾旗, 李兆进. 细胞因子和卫星细胞在肌肉再生中的相互作用[J]. 中国组织工程研究, 2026, 30(7): 1808-1817. |
| [8] | 王振泽, 刘奋德, 张 瑞, 李武军. 间充质干细胞治疗下肢动脉硬化闭塞症:系统评价和Meta分析[J]. 中国组织工程研究, 2026, 30(7): 1869-1876. |
| [9] | 张子华. 从坐到站动作老年下肢肌群仿真及用力特征分析[J]. 中国组织工程研究, 2026, 30(6): 1407-1416. |
| [10] | 钟彩红, 肖晓歌, 李 明, 林剑虹, 洪 靖. 运动相关髌腱炎发病的生物力学机制[J]. 中国组织工程研究, 2026, 30(6): 1417-1423. |
| [11] | 侯超文, 李兆进, 孔健达, 张树立. 骨骼肌衰老主要生理变化及运动的多机制调控作用[J]. 中国组织工程研究, 2026, 30(6): 1464-1475. |
| [12] | 孙尧天, 徐 凯, 王沛云. 运动影响铁代谢对免疫性炎症疾病调控的潜在机制[J]. 中国组织工程研究, 2026, 30(6): 1486-1498. |
| [13] | 曹新燕, 于子夫, 冷晓轩, 高世爱, 陈金慧, 刘西花. 重复经颅磁刺激和经颅直流电刺激对脑瘫患儿运动功能及步态影响的网状Meta分析[J]. 中国组织工程研究, 2026, 30(6): 1539-1548. |
| [14] | 周 坚, 张 涛, 周威力, 赵星丞, 王 军, 沈 杰, 钱 丽, 陆 明. 抗阻训练对骨质疏松并肌少症患者股四头肌质量及膝关节功能的影响[J]. 中国组织工程研究, 2026, 30(5): 1081-1088. |
| [15] | 李郝静, 王 新, 宋成林, 张胜男, 陈云昕. 上斜方肌处体外冲击波与运动控制训练治疗慢性非特异性颈痛[J]. 中国组织工程研究, 2026, 30(5): 1162-1170. |
中国传统运动是以中医理论为基础的运动干预手段,涵盖太极拳、八段锦、易筋经、五禽戏等运动形式,其历史可追溯至3 000多年前[16]。中国传统运动兼具治疗性与有氧运动特性,治疗性源于相关中医理论基础(涵盖了经络脏腑学原理、阴阳五行学说等),并融合了中国传统哲学思维与养生观念的精髓[17]。大量现代临床研究证实,中国传统运动作为运动干预措施,在老年人心血管疾病、糖尿病及高血压等慢性病的治疗与康复过程中发挥着积极作用[18-21]。同时,中国传统运动能够通过刚柔并济的动作设计实现身心协同调节,与现代医学中常用的抗阻训练、高强度间歇训练等运动干预手段相比,中国传统运动在安全性、普适性及身心同步干预方面具有独特优势[22]。目前,已有研究针对中国传统运动对老年肌少症及其合并症的干预效果展开分析,结果显示中国传统运动可有效改善该类患者的肌肉功能、骨密度及平衡、认知等身体功能,从而降低跌倒、虚弱等多种不良健康结果的发生风险,进而改善患者的生活质量[23-26]。但单一的随机对照试验仍存在局限性:现有随机对照试验样本量普遍较小,统计效能不足;多数研究聚焦于单一的中国传统运动类型(如仅太极拳),缺乏多种中国传统运动(太极拳、八段锦、易筋经等)对不同结局指标(肌肉质量、力量、功能)的横向效能比较;各项研究间所采用的干预参数(运动周期、频率与时间)差距较大,导致结果可比性降低[27-29]。此外,虽有研究采用Meta分析对相关结果进行了证据整合,但对中国传统运动用于老年肌少症及其合并症的预防与治疗仍存在一定的局限性,例如,孙嘉禾等[7]通过Meta分析检验了运动干预对老年肌少症及其合并症患者肌肉力量、质量与身体功能的干预效果,但并未针对于中国传统运动进行特异性分析;HUANG等[30]的研究运用Meta方法分析了太极拳对老年体弱与肌少症患者的影响,但所纳入的干预措施仅包含太极拳,缺乏对其他中国传统运动的考量;NIU等[31]分析了中国传统运动对老年肌少症患者肌肉力量与身体功能的影响,但该研究纳入的样本量较少且未对患者的肌肉质量改变进行评估。上述Meta分析均未进一步分析中国传统运动干预老年肌少症及其合并症的周期、频率、时长等干预参数以及不同类型中国传统运动之间在改善相关指标上效应的差异,这可能降低中国传统运动在指导运动处方制定中的可用性。
鉴于此,此次研究运用Meta分析方法,针对中国传统运动改善老年肌少症及其合并症患者肌肉力量、质量与身体功能的相关研究进行全面系统的定量回顾,并通过亚组分析探析可能促进中国传统运动改善效应更优的干预参数以及不同形式的中国传统运动对改善不同指标效应量的差异;同时,从生理、生化等层面深入探讨中国传统运动干预效能的潜在机制,旨在为相关临床试验的设计与运动处方的制定提供理论依据与实践参考。
中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
研究根据PRISMA(Preferred Reporting Items
for Systematic Reviews and Meta-Analyses)中关于系统性综述与Meta分析的标准声明进行实施的[32]。该方案已在约克大学评价和传播中心PROSPERO数据库注册:注册号CRD420251071083(https://www.crd.york.ac.uk/PROSPERO/view/CRD420251071083.)
1.1 检索策略 由2名研究者采用双盲法执行检索任务,检索时间跨度设定为各数据库建库至2025-07-30。检索范围涵盖中英文数据库:①英文数据库包括Web of Science、Cochrane Library、PubMed,检索词包括TaiJi、Exercises、elderly、Tai Chi Chuan、Baduanjin、Chinese Traditional Sports、Yijinjing、Sarcopenia、Sarcopenic Obesity、Osteosarcopenia、Aged、senior citizens、Randomized controlled trial等;②中文数据库选用中国知网(CNKI)与万方数据知识服务平台,检索词包括肌肉减少症、肌少症性肥胖、肌少骨质疏松症、肌肉衰减症、中国传统运动、太极拳、八段锦、易筋经、气功、武术、随机对照试验等。检索策略以PubMed为例,见表1。
检索完成后,首先通过EndNote等文献管理软件剔除重复文献。随后依据预先制定的纳入与排除标准,对文献标题和摘要进行初筛,排除明显不相关的研究。初筛合格的文献进一步获取全文,由2名独立研究者分别进行复筛、质量评价及数据提取。若出现分歧,将由通讯作者组织讨论会议协商解决。
1.2 研究方案设计 见图1。
1.3 文献纳入与排除标准 根据Cochrane的PICOS原则,此次研究所制定的文献纳入与排除标准如下:
纳入标准:①研究对象:平均年龄≥60岁的老年人群,涵盖所有性别,并且需明确依据相关诊断标准或指南确诊为肌少症及其合并症,其中肌少症合并症包括肌少症性肥胖、肌少骨质疏松症、骨肌少症性肥胖;②干预措施:试验组采用易筋经、太极拳、八段锦等中国传统运动中的一项或多项进行干预,对照组进行健康教育、常规护理或远程太极拳指导;③研究类型:仅纳入随机对照试验,无论是否采用盲法;④结局指标:研究需包含以下至少一项结局指标,以握力、膝关节肌肉力量作为评价指标,以四肢骨骼肌质量指数作为肌肉质量评价指标,以坐立测试、步速、站立-行走计时测试及简易体能状况表作为身体功能评价指标排除标准:非随机对照试验研究;试验组干预措施存在混杂,如采用其他类型运动干预(抗阻训练、骑行、游泳、间歇训练等其他非中国传统运动项目),或未清晰界定运动类型;研究对象不符合要求,包括非人类受试者、干预对象平均年龄< 60岁,或未提及肌少症及其他合并症诊断标准或指南;研究数据不完整且无法获取补充;未涉及任何预设结局指标。
1.4 数据提取 2名研究人员在文献检索的过程中,以双盲的形式对纳入文献进行数据提取工作。若在提取过程中出现意见分歧,则由通讯作者组织会议协商解决。提取的数据具体内容如下:①文献基本信息:第一作者、发表年份;②受试者信息:样本量、年龄、身体状态等受试者特征;③干预措施信息:收集中国传统运动干预的具体方案,涵盖具体运动方式、干预周期、干预频率及单次干预时长,后续将基于这些数据开展进一步的亚组分析,以探究中国传统运动在不同干预参数条件下(运动方式、干预周期、干预频率单次干预时长),对老年

肌少症及其合并症患者各项结局指标的干预效果,同时明确不同类型中国传统运动针对相关指标进行干预时的最佳参数;④试验结果数据:对于各项指标的干预结果,仅提取结局指标的最终值与基线值,并以干预前和干预后的平均值及标准差的形式呈现。
1.5 质量评价 此次研究采用Cochrane手册推荐的偏倚风险评估工具(RoB2)[33],由2名研究人员独立完成纳入文献的偏倚风险评估。若评估结果存在分歧,则由通讯作者组织讨论协商解决。评估内容涵盖以下维度:①随机化过程中存在的选择偏倚;②干预措施未按既定方案实施产生的执行偏倚;③结局数据缺失引起的报告偏倚;④结局测量方法运用不当所产生的检测偏倚;⑤选择性报告研究结果所产生的报告偏倚;⑥其他潜在的风险偏倚。各评估条目依据风险程度划分为“低风险”“高风险”和“不清楚”3个等级。根据综合评估结果,将纳入文献分为3个等级:A级(所有评估条目均为“低风险”)、B级(部分条目为“低风险”)和C级(无条目为“低风险”)。1.6 统计学分析 此次研究通过运用Revman 5.4和Stata 15.1软件对纳入文献的结局指标开展Meta分析及相关研究,旨在明确中国传统运动对老年肌少症及其合并症的干预效果与最佳干预参数。研究中,所有纳入文献的结局指标均为连续性变量,当测量单位统一时,以合并均数差(Mean Difference,MD)及其95%置信区间(95% Confidence Interval,95%CI)作为Meta分析的效应尺度;反之则采用标准化均数差(Standardized Mean Difference,SMD)及其95%CI进行统计分析。
在异质性评估方面,运用I2与Q检验判断是否存在异质性:当I2≤50%且P≥0.01,为低异质性,采用固定效应模型;当I2 > 50%且P < 0.01,则为高异质性,采用随机效应模型。为评估潜在发表偏倚,研究采用Begg检验和Egger检验进行统计学分析,若检测到发表偏倚,将使用剪补与填充法评估研究总体效应的稳定性。此外,通过逐一剔除纳入文献开展敏感性分析,以检验Meta分析结果的稳健性;同时进行亚组分析,以探究不同干预方式、干预频率、干预时长及干预周期对结局指标的影响差异。该文生物统计学方法已经安徽工程大学生物统计学专家审核。
中国传统运动,如八段锦、易筋经、太极拳等,通常被归类为中低强度的有氧运动[49],整合现有研究来看,它们的分子机制可能与二者在执行过程中均能激活骨骼肌中与耐力适应性相关的关键信号通路——AMP活化蛋白激酶/过氧化物酶体增殖物激活受体γ共激活因子1α信号通路有关。其中,有氧运动的特征是持续能量消耗,这会导致细胞内能量状态改变,即AMP与ATP的比率升高;而这种细胞能量状态的改变是激活AMP活化蛋白激酶的关键信号[50];被激活的AMP活化蛋白激酶通过直接磷酸化过氧化物酶体增殖物激活受体γ共激活因子1α,进而增强过氧化物酶体增殖物激活受体γ共激活因子1α的转录活性[51]。作为线粒体生物发生与代谢重塑的“调节因子”,被激活的过氧化物酶体增殖物激活受体γ共激活因子1α可驱动一系列基因表达,最终促进线粒体生成、毛细血管密度增加、脂肪酸氧化,并诱导肌纤维类型向更具抗疲劳性的氧化型纤维转化[52]。然而,目前仅有少量研究表明中国传统运动可有效改善老年人的骨骼肌能量代谢,缩短肌酸磷酸的恢复时间,并增强线粒体功能[53]。缺乏相关蛋白质组学或特定分子标志物的检测对中国传统运动改善身体状态的分子机制进行深入探究,这就提示在未来研究中应深入探究中国传统运动对相关信号通路及分子标志物的影响,以明确其改善身体状态的具体分子机制。
在运动促进肌肉功能改善方面,已有大量研究证实,抗阻训练可通过激活胰岛素样生长因子1/蛋白激酶B信号通路促进肌肉蛋白质合成和肌肉肥大,进而提升肌肉绝对力量[54];同时,抗阻训练可通过特异性激活MKK3b/6-p38-MK2-哺乳动物靶蛋白雷帕霉素复合体1通路促进蛋白合成,进而改善肌肉质量[55]。而作为中国传统运动的上位概念,有氧训练对肌肉力量的改善主要体现于肌肉功能性力量及耐力的提升,潜在机制主要与上述AMP活化蛋白激酶/过氧化物酶体增殖物激活受体γ共激活因子1α通路相关:通过增强线粒体密度和氧化酶活性,有氧运动能够提高肌肉在长时间工作中的供能效率与抗疲劳能力,这通常意味着肌肉可更持久、更有效地进行力量输出[56];同时,受到激活的AMP活化蛋白激酶还能促进骨骼肌对葡萄糖和脂肪酸的摄取与利用,减少肌内脂肪的堆积,而过多的肌内脂肪是肌肉质量下降的一个重要标志[57];此外,有氧运动还能够激活α运动神经元,增强肌纤维募集效率,并促进神经递质释放以刺激肌腱,进而实现肌肉力量的增强[58];通过提高骨骼肌AMP活化蛋白激酶活性抑制哺乳动物雷帕霉素靶蛋白信号通路,减少哺乳动物雷帕霉素靶蛋白对Unc-51样激酶1的磷酸化作用,从而上调自噬水平,降解肌肉蛋白质,为肌肉收缩和代谢活动提供能量底物[59]。考虑到老年肌少症及其合并症患者身体较为虚弱,可能无法完成单一的高强度抗阻运动,因此,在进行有氧运动的同时联合中等强度抗阻训练或可进一步促进患者肌肉质量的改善,潜在机制可能在于:胰岛素样生长因子1作为影响骨代谢的肌因子,它水平的提升有助于刺激肌肉与骨膜生长;抗阻训练通过对骨骼肌施加机械刺激能促进生长激素的急性分泌[60],并激活细胞膜上的ADAM10和ADAM17等蛋白酶[61],而生长激素是促进肝脏合成胰岛素样生长因子1的主要上游信号,蛋白酶的活化也为局部组织中胰岛素样生长因子1的释放提供了可能;随后衔接的有氧训练可通过促进血管扩张降低血管内阻力,增加血液流动[62],可能提高因抗阻训练产生或激活的生长激素及ADAM10、ADAM17等蛋白酶向肝脏与相关靶组织的输送效率;同时,有氧运动可通过磷脂酰肌醇3激酶/蛋白激酶B信号通路汇聚于哺乳动物靶蛋白雷帕霉素复合体1节点,并增强p70S6K和4E-BP1的磷酸化,对因抗阻训练所激活的蛋白合成形成协同放大效应[63]。
对老年肌少症及其合并症患者而言,长期的训练依从性是决定预防与康复成败的关键。虽同属于有氧训练序列,但相较于骑行、跑步等传统有氧训练而言,中国传统运动的动作柔和、节奏缓慢、强度可控,几乎没有运动冲击,极大地降低了肌肉拉伤、关节损伤和心血管意外的风险[64]。目前,有研究针对于中国传统运动对于肌肉功能的改善成效进行了分析:在中国传统运动过程中,训练者髋、膝、踝关节需完成多方向的向心与离心收缩运动[65],而两种收缩形式均可增强肌肉力量,并且离心收缩的肌力提升效果更佳[66];以太极拳、八段锦为代表的传统健身运动强调缓慢连贯的动作控制,该运动模式通过反复激活拮抗肌群有助于增强神经肌肉募集能力,改善肌肉协同收缩的协调性[67]。此外,慢性炎症是肌少症发生发展的重要病理基础[68],炎症反应可直接损伤肌纤维结构,加剧肌少症进展[69],而易筋经锻炼可显著降低肌少症患者血清肿瘤坏死因子α、白细胞介素8等促炎因子水平[38],并且肿瘤坏死因子α水平与握力呈显著负相关;中国传统运动还可通过下调促炎因子白细胞介素6的表达减轻骨骼肌炎症反应,进而促进肌肉力量提升[70-71]。此外,老年肌少症及其合并症患者常存在生长激素分泌不足现象,而作为中国传统运动的所属项目,气功锻炼可显著提高机体生长激素水平[72],进而提升患者体内的胰岛素样生长因子水平,改善患者肌肉质量[73-74]。
除单一的运动干预以外,维生素、抗氧化营养素、蛋白质和长链多不饱和脂肪酸等营养物质与抗炎等药物补充,对肌肉质量的改善也有着积极作用[75]:在运动后补充乳清蛋白或支链氨基酸,能够协同激活哺乳动物雷帕霉素靶蛋白通路,进而放大蛋白质的合成效应[76]。ω-3脂肪酸减少线粒体活性氧生成,能够保护肌纤维结构,联合有氧运动可显著提高肌肉力量[77]。太极拳联合β-羟基-β-甲基丁酸可增强胰岛素样生长因子1的表达,进而放大磷脂酰肌醇3激酶/蛋白激酶B信号[78]。非类固醇抗炎药(如布洛芬)联合有氧运动可进一步抑制炎症因子(如白细胞介素6),减少肌肉分解[76]。因此,在实施中国传统运动干预的同时同步开展营养补充与药物辅助治疗,可通过多靶点协同作用显著增强肌肉质量改善效果。
老年人的身体功能是一个综合概念,包括平衡能力、步态稳定性、记忆力等。有氧运动对此的促进作用涉及中枢神经系统和外周系统的多重分子机制。在神经可塑性与认知功能方面,脑源性神经营养因子是一种关键的蛋白质,能促进神经元的存活、生长和分化,增强突触可塑性,这对学习和记忆至关重要。有研究表明,有氧运动可增加循环血清和海马区的脑源性神经营养因子水平[79];同时与改善肌肉质量类似,有氧运动可通过降低全身和中枢神经系统内的白细胞介素6和肿瘤坏死因子α等促炎因子水平,能够保护神经元免受炎症损伤,延缓认知衰退[80]。中国传统运动促进身体功能改善的潜在机制主要为:太极拳练习中,缓慢的动作模式促使练习者专注于各运动姿势下的本体感觉输入,从而增强本体感觉系统的敏感性[81];同时,太极拳和八段锦可激活前额叶皮质,尤其是背外侧前额叶皮质和内侧前额叶皮质的神经活动,进而改善注意力、执行功能和记忆功能[82]。太极拳训练可显著提升老年人血浆脑源神经营养因子和胰岛素样生长因子1水平,上述因子通过促进神经元生长、增强突触可塑性,对认知功能产生改善作用[72]。八段锦通过改善视觉-前庭系统功能可有效提升整体平衡能力[83]。易筋经可提高慢肌纤维与快肌纤维的做功量及效率增强骨骼肌收缩协调性与关节稳定性,并显著改善静态与动态平衡能力及核心稳定性[84]。八段锦可增强肺部通气与换气功能促进微循环中毛细血管内外物质的交换,加快血液循环速度,优化细胞组织对氧气的利用效率,进而调节机体能量代谢[85]。中国传统运动锻炼还能够通过调节自主神经系统增强副交感神经活动,降低交感神经活动,从而改善老年人的免疫功能和整体健康状况[86]。此外,还有研究通过表面肌电图等技术发现,太极拳能显著改善老年肌少症患者的神经肌肉反应时间与姿势控制能力,这意味着即使肌肉绝对力量没有大幅增加,患者也能更快速、更精确地调动肌肉以维持平衡,这对于预防突发性跌倒至关重要[87]。
综上所述,无论是中国传统运动还是有氧运动,均能通过对肌肉力量、质量与身体功能的促进,进而对老年肌少症及其合并症的预防与康复起到相应作用。但中国传统运动的所属项目较多,运动形式、运动强度等也所有不同,因此,对于肌肉力量、质量与身体功能的改善侧重点也有所不同。此次研究亚组分析结果显示,与易筋经相比,太极拳对肌肉质量的直接提升效果并无统计学意义,然而,太极拳在改善肌肉力量,特别是下肢功能性力量和耐力方面却效果显著,这可能是由于:太极拳的作用机制更侧重于优化肌肉募集与协调能力,而并非单纯地提升肌肉围度[67];由于太极拳动作连贯、重心在两腿间不断转换的特点,可能对于下肢的支撑力、控制力和稳定性以及预防跌倒相关的髋部和膝关节周围肌群力量有独特优势[88];同时,太极拳的持续性负荷可能更侧重于优化慢肌纤维(Ⅰ型纤维)的氧化能力和抗疲劳特性。八段锦的动作分节,每一式都有特定的拉伸和发力点,例如“左右开弓似射雕”对上肢和背部肌群有较强刺激,“攒拳怒目增气力”则强调握力和下盘稳定,因此,八段锦可能对全身不同肌群提供更为均衡和针对性的刺激[89]。易筋经独特的发力模式可能在提升绝对力量方面最具潜力。有研究指出,易筋经训练能显著提高老年人及肌少症患者的肌肉力量,它强调的“刚”性发力,对肌肉施加的机械张力可能更大,从而更能有效地刺激肌肉力量的增长[90]。而要从根本上理解上述异质性,需深入到细胞和分子层面,但目前关于中国传统运动促进肌肉力量、质量或身体功能的研究现状呈现“功能与分子”脱节的特点:一方面,功能性、临床性益处拥有大量实证支持;另一方面,直接来源于人体肌肉组织的分子生物学证据(尤其是用于区分不同传统运动特异性效果的比较性研究)几乎为空白。对分子机制的阐述,多为基于运动生理学理论的逻辑推断,例如,易筋经凭借高机械张力负荷,最有可能强烈激活哺乳动物靶蛋白雷帕霉素复合体1信号通路,促进p70S6K和4E-BP1的磷酸化,进而启动蛋白质翻译和肌肉合成;太极拳则凭借持续性中等强度负荷,可能通过抑制分解代谢通路、降低炎症水平及改善线粒体功能等综合作用改善肌肉健康。因此,未来研究应深入分析不同种类的中国传统运动对AMP活化蛋白激酶磷酸化、过氧化物酶体增殖物激活受体γ共激活因子1α、蛋白激酶B磷酸化等关键信号分子及相关生物标志物的影响,以进一步明确不同中国传统运动在改善相关指标方面的差异性。
此次研究聚焦于中国传统运动对老年肌少症及其合并症患者肌肉力量、质量与身体功能的干预效果分析,在既往相关Meta分析的基础上,通过纳入最新发表的相关研究成果,扩大了研究所纳入的样本总量;同时,研究严格遵循PRISMA指南,在PROSPERO平台完成了研究方案的预注册(注册号:CRD420251071083),确保研究流程的透明、可重复。此次研究开展了不同中国传统运动对肌少症患者肌肉质量干预效果的系统性比较,通过亚组分析,首先明确了中国传统运动在改善患者握力、膝关节肌肉力量、四肢骨骼肌质量与身体功能方面,于运动周期、运动频率与单次运动时长上的最佳干预参数;继而针对不同类型的中国传统运动,进一步分析了它们的相关最佳干预参数,可为后续临床试验的设计与个性化运动处方的制定提供相关参考。
但与此同时,此次研究仍存在以下局限性:①原始文献的质量局限,纳入研究的质量整体有限,仅1篇为A级文献,其余均为B级。部分研究未实施盲法和分配隐藏,可能会存在一定程度的选择偏倚和实施偏倚。此外,根据2004年相关声明,临床试验需完成注册以确保研究的科学性与透明度[91],但此次研究纳入的多数中文文献未进行注册,存在研究规范性不足的问题。②语言局限性,此次研究仅对英文与中文数据库进行检索,可能遗漏其他语种发表的相关研究。③结局指标与样本限制:符合纳入标准的研究中,针对于膝关节肌肉力量与简易体能状况表的研究数量少、样本量不足,可能影响结果准确性;同时,现有中英文数据库中缺乏中国传统运动对肌少性骨质疏松、肌少症性肥胖等合并症的干预研究,导致此次研究在该领域证据不足,可能会影响结论针对性。除此之外,在所纳入文献中,仅7篇文献对所采用的运动干预强度进行了标注,并且均为中低等运动强度,因此无法对中国传统运动在不同干预强度下的效应量变化进行分析。④长期干预效果的评估不足,研究所纳入文献缺乏长期的随访证据,无法对中国传统运动干预效果的持续性和远期影响进行有效评估。
针对此次研究现存局限性,后续研究可从以下维度深化完善:①优化研究设计:建议开展多中心、大样本量的随机对照试验,统一中国传统运动干预参数标准,延长随访周期,以此降低研究间的异质性,提升结果论证强度。同时需严格规范盲法实施与分配隐藏策略,并完成临床试验注册,确保研究过程的透明化与标准化。②深化机制研究:胰岛素样生长因子1作为重要的生长调节因子,在肌肉合成代谢及肌少症防治中发挥关键作用,后续研究需系统探究中国传统运动对老年人群胰岛素样生长因子1合成代谢的调控机制,以完善相关生理病理模型。③拓展干预模式:需进一步验证中国传统运动与营养补充、药物治疗、抗阻训练或振动训练等干预手段的协同效应,探索建立多模式联合干预方案。④促进临床转化:基于相关研究得出的干预参数模型,构建个性化运动处方体系,为临床精准治疗提供理论依据与实践指导,切实提升治疗的有效性与安全性。
此次研究采用Meta分析方法,系统分析中国传统运动对老年肌少症及其合并症患者握力、膝关节肌肉力量、四肢骨骼肌质量与身体功能的影响,结果显示,中国传统运动有助于提高老年肌少症及其合并症患者的握力、膝关节肌肉力量、四肢骨骼肌质量与身体功能。同时,两轮亚组分析结果表明:在提升此类患者握力方面,易筋经(干预> 12周、每周干预> 3次、单次运动≤30 min)的效果最佳;在改善患者四肢骨骼肌质量指数方面,八段锦(干预12周、每周干预≤3次、单次运动> 30 min)的效果最优;太极拳(干预> 12周、每周干预> 3次、单次运动≤30 min)或八段锦(干预12周、每周干预3次、单次运动> 30 min)均能显著提升患者步速;在改善患者坐立测试成绩方面,易筋经(干预8周、每周干预5次、单次运动≤40 min)的效果最佳;八段锦(干预> 12周、每周干预≤3次、单次运动> 30 min且≤40 min)对起立-行走测试成绩的改善最显著。除此之外,此次研究纳入文献中仅少数注明运动强度,但均属中低强度。因此,建议在临床应用或运动处方制定过程中,无论采用何种参数模型,均需将强度控制为:Borg自觉疲劳量表11-14级、60%-70%最大心率、主观疲劳度11-13级、50%-55%最大摄氧量等中低档运动强度。
综上所述,此次研究为老年肌少症及其合并症的预防与康复提供了中国传统运动的应用策略与循证依据,在当前外源性治疗方法存在一定局限性的背景下,研究结果可为该类疾病的防治提供初步证据,对临床实践具有一定指导意义。未来研究需进一步深化机制探索,设计涵盖多种干预参数组合的随机对照试验,以持续提升中国传统运动在肌少症预防与康复中的实用性和科学性。
中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
此次研究系统比较了中国传统运动对老年肌少症及其主要合并症患者肌肉力量、肌肉质量和身体功能的多维度干预效果。通过严格的Meta分析方法,整合了21项随机对照试验(n=1313)的相关数据。研究不仅证实中国传统运动可显著改善患者握力、膝关节肌力、四肢骨骼肌质量指数(ASMI)、步速、坐立能力、起立-行走能力(TUG)及综合体能(SPPB),更通过详尽的亚组分析,明确了针对不同改善目标的最佳中国传统运动方式及关键干预参数(如周期、频率、单次时长)。研究揭示,中国传统运动对老年肌少症及其合并症的干预效果存在“剂量-效应”关系及运动类型特异性,这可为临床医生和康复治疗师制定精准化、个性化的老年肌少症运动处方提供循证依据,也在一定程度上弥补了既往综述仅关注单一运动或缺乏参数优化的不足。此外,研究探讨了中国传统运动改善肌肉功能的潜在生理生化机制,可为未来的机制研究提供参考。
中国组织工程研究杂志出版内容重点:干细胞;骨髓干细胞;造血干细胞;脂肪干细胞;肿瘤干细胞;胚胎干细胞;脐带脐血干细胞;干细胞诱导;干细胞分化;组织工程
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||