Chinese Journal of Tissue Engineering Research ›› 2020, Vol. 24 ›› Issue (28): 4580-4587.doi: 10.3969/j.issn.2095-4344.2317
Previous Articles Next Articles
Cardiac valve prosthesis implantation and surgical maze ablation for the treatment of valvular disease with atrial fibrillation
Ma Chao1, 2, Wang Huishan2, Han Jinsong2, Yin Zongtao2, Zhang Xiling1, 2
1Graduate School, General Hospital of Northern Theater Command, Jinzhou Medical University, Shenyang 110016, Liaoning Province, China; 2Department of Cardiovascular Surgery, General Hospital of Northern Theater Command, Shenyang 110016, Liaoning Province, China
-
Received:2019-12-05Revised:2019-12-10Accepted:2020-01-22Online:2020-10-08Published:2020-09-01 -
Contact:Han Jinsong, MD, Associate chief physician, Master candidate, Department of Cardiovascular Surgery, General Hospital of Northern Theater Command, Shenyang 110016, Liaoning Province, China -
About author:Ma Chao, Master candidate, Graduate School, General Hospital of Northern Theater Command, Jinzhou Medical University, Shenyang 110016, Liaoning Province, China; Department of Cardiovascular Surgery, General Hospital of Northern Theater Command, Shenyang 110016, Liaoning Province, China -
Supported by:the Major Project of the Natural Science Foundation of Liaoning Province in 2017, No. 20170540977
CLC Number:
Cite this article
Ma Chao, Wang Huishan, Han Jinsong, Yin Zongtao, Zhang Xiling.
Cardiac valve prosthesis implantation and surgical maze ablation for the treatment of valvular disease with atrial fibrillation [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(28): 4580-4587.
share this article
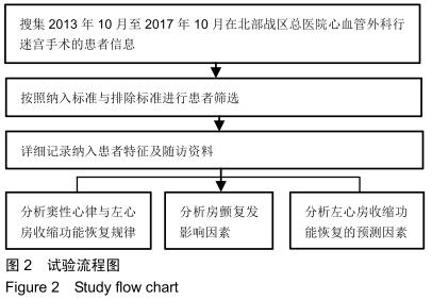
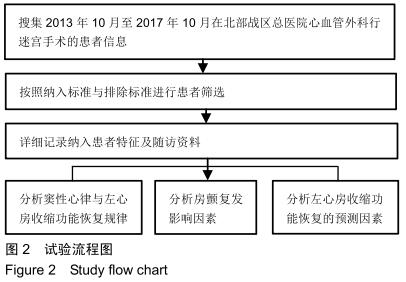
2.1 参与者数量分析 324例患者均进入结果分析。 2.2 试验流程 见图2。 "
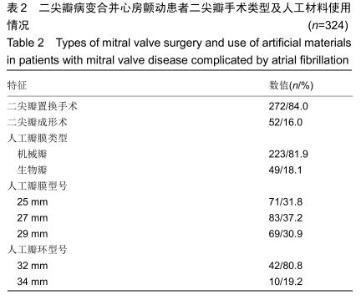
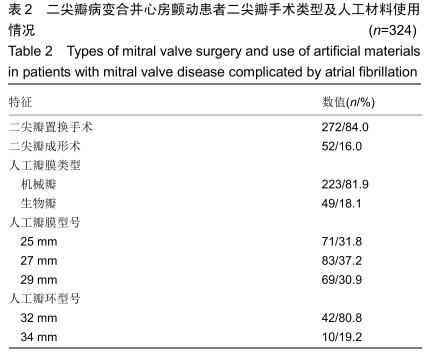
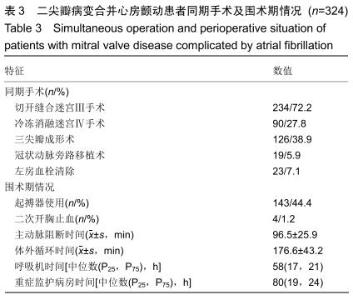
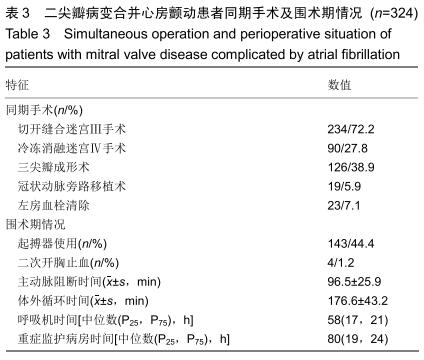
2.3 患者围术期情况 随访情况及并发症:324例患者均接受二尖瓣置换或瓣环成形术,二尖瓣置换材料以机械瓣为主,人工瓣环型号以32 mm较多。详见表2。术后4例患者(1.2%)因出血接受二次开胸手术,其病因均非迷宫手术切口引起。有2例患者(0.6%)在术后早期死亡,原因均为心力衰竭。其余所有患者均获得2年临床随访,随访期间无患者死亡和脑卒中,详见表3。术后2年,3例患者(0.9%)因窦性心动过缓需要永久性起搏器。 不良反应:瓣环成形患者无成形环断裂或撕脱、无溶血、左室流出道梗死、传导组织损伤。无再次手术行瓣膜置换患者。瓣膜置换患者无心内膜炎、非结构性功能障碍,结构性损伤,心肌缺血及血栓等发生。 植入材料与宿主反应 :①局部反应:本组病例均无局部炎症、刺激反应、过敏反应及组织增生;无材料腐蚀、磨损、生物降解、材料退化等。②全身反应:本组病例均无炎症和过敏现象,未发现细胞毒性、凝血改变、补体激活、致癌表现及免疫反应等。 "
"
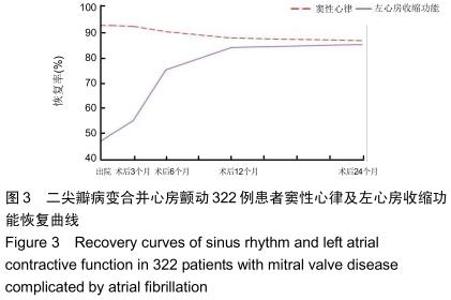
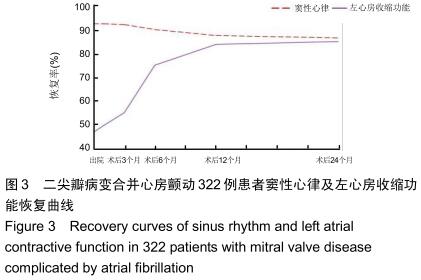
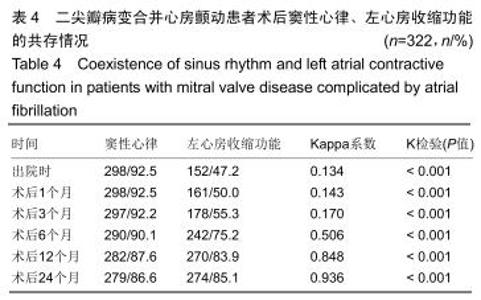
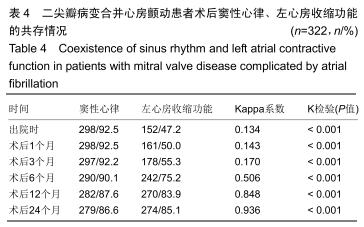
2.4 生物相容性随访结果 322例患者均获得2年临床随访,随访期间无患者发生死亡和脑卒中。 2.4.1 窦性心律与左心房收缩功能 322例患者中,出院时298例患者(92.5%)获得窦性心律。出院至术后3个月,窦性心律与左心房收缩功能共存的一致性较差(Kappa系数<0.40,P < 0.05),表明此阶段大多数窦性心律不能伴随相应的左心房收缩功能。术后6个月时窦性心律与左心房收缩功能共存的一致性较一般(0.75>Kappa系数≥0.40,P < 0.05),术后12个月至术后2年,窦性心律与左心房收缩功能共存的一致性较好(Kappa系数≥0.75,P < 0.05),见图3,表4。术后2年,98.2%的窦性心律可伴随相应的左心房收缩功能。在不同时间的随访检查中,无相应左心房收缩功能的窦性心律患者无明显突出假体植入类型特征。 "
"

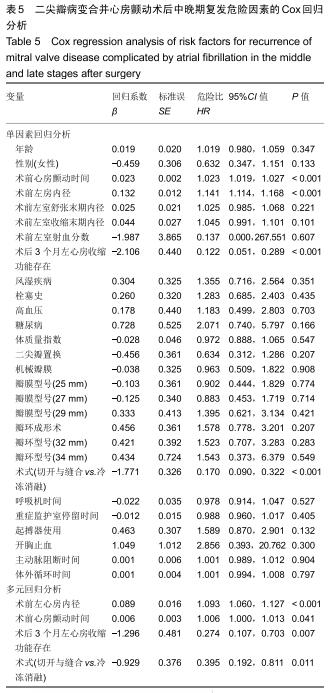
2.4.2 心房颤动中晚期复发的危险因素分析 在Cox单因素回归分析中发现,二尖瓣置换、机械瓣膜的选择、瓣膜型号、瓣环成形术及瓣环型号等并未对中晚期房颤复发造成影响(P均> 0.05),而较长术前房颤时间、较大术前左心房内径、术后3个月左心房收缩功能缺失、冷冻消融术式是术后中晚期房颤复发的重要危险因素(P均< 0.05),将它们纳入多元Cox回归模型后发现它们作为房颤中晚期复发的危险因素仍具有统计学意义,见表5。 "

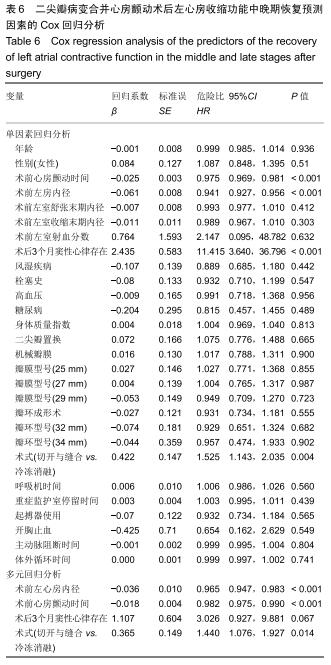
2.4.3 左心房收缩中晚期恢复的预测因素分析 在对左心房收缩功能中晚期恢复预测因素的Cox单变量回归分析中,二尖瓣置换、机械瓣膜的选择、瓣膜型号、瓣环成形术以及瓣环型号等并不是左心房收缩功能中晚期恢复的影响因素(P值均> 0.05)。术前较短的房颤持续时间、较小术前左心房内径、术后3个月窦性心律存在及切开与缝合术式的应用是其重要预测因子(P均< 0.05)。在多变量Cox模型中,再次确认了较长术前心房颤动持续时间、较大术前左心房内径以及切开与缝合术式的应用对于左心房收缩功能中晚期恢复所起的预测作用(表6)。 "
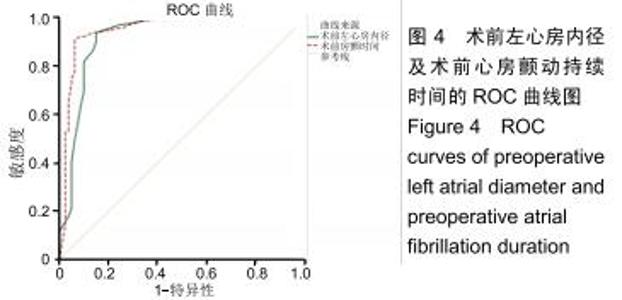
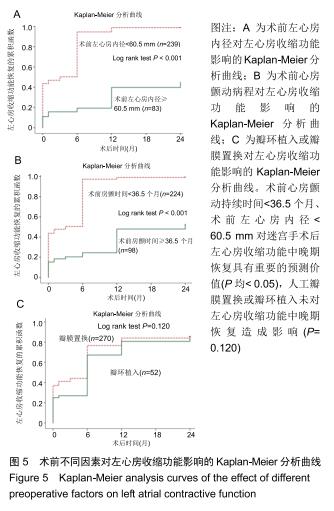
结合左心房收缩功能中晚期恢复预测因素结果绘制ROC曲线,见图4。术前心房颤动持续时间、术前左心房内径曲线下面积分别为 0.948,0.921,均大于0.9[95%CI (0.913,0.984),P < 0.001;95%CI(0.876,0.966),P <0.001]。术前心房颤动持续时间与术前左心房内径预测左心房收缩功能恢复的最佳临界值分别为36.5个月(敏感度90.5%,特异性93.7%),60.5 mm(敏感度93.8%,特异性85.0%)。Kaplan-Meier分析还证实,术前心房颤动持续时间<36.5个月、术前左心房内径<60.5 mm对迷宫手术后左心房收缩功能中晚期恢复具有重要的预测价值(Log rank test P均< 0.05),见图5A,B;人工瓣膜置换或瓣环植入并未对左心房收缩功能中晚期恢复造成影响(Log rank test P=0.120),见图5C。 "

"
|
[1] LIP GYH, COLLET JP, CATERINA R, et al. Antithrombotic therapy in atrial fibrillation associated with valvular heart disease: a joint consensus document from the European Heart Rhythm Association (EHRA) and European Society of Cardiology Working Group on Thrombosis, endorsed by the ESC Working Group on Valvular Heart Disease,Cardiac Arrhythmia Society of Southern Africa (CASSA), Heart Rhythm Society (HRS), Asia Pacific Heart Rhythm Society (APHRS), South African Heart (SA Heart) Association and Sociedad Latinoamericana de Estimulacion Cardiaca y Electrofisiologia (SOLEACE).Europace.2017;117(12):2215-2236.
[2] RUAENGSRI C, SCHILL MR, KHIABANI AJ, et al. The Cox-maze IV procedure in its second decade: still the gold standard? Eur J Cardiothorac Surg.2018;53(suppl_1):i19-i25.
[3] DENEKE T, KHARGI K, GREWE PH, et al. Efficacy of an additional MAZE procedure using cooled-tip radiofrequency ablation in patients with chronic atrial fibrillation and mitral valve disease. A randomized, prospective trial.Eur Heart J.2002;23(7):558-566.
[4] GILLINOV M,SOLTESZ EG.Atrial fibrillation in the patient undergoing mitral valve surgery: A once-in-a-lifetime opportunity.J Thorac Cardiovasc Surg.2018;155(3):995-996.
[5] LOMBARD FW, LIANG Y. Risk Factors for Mitral Valve Surgery: Atrial Fibrillation and Pulmonary Hypertension.Semin Cardiothorac Vasc Anesth.2019;23(1):57-69.
[6] FIRMANSYAH DK, SOESANTO AM, HANAFY DA, et al. Cox maze IV versus left atrial reduction for atrial contraction restoration.Asian Cardiovasc Thorac Ann.2019;27(5):353-361.
[7] NITTA T, ISHII Y, FUJII M, et al. Restoration of sinus rhythm and atrial transport function after the maze procedure: U lesion set versus box lesion set.J Thorac Cardiovasc Surg. 2016;151(4):1062-1069.
[8] 韩劲松,王辉山,汪曾炜,等.人工瓣环置入和迷宫Ⅲ型手术治疗退行性二尖瓣环扩张伴发心房颤动[J].中国组织工程研究,2015,19(52):3562-3569.
[9] 谢赛旗,王辉山,韩劲松,等.机械瓣膜或生物瓣膜置换及经典迷宫Ⅲ型手术治疗心房颤动合并巨大左心房和风湿性二尖瓣病变[J].中国组织工程研究,2019,23(26):4187-4193.
[10] 韩冰,王辉山,韩劲松,等.瓣膜置换或瓣环置入同期迷宫Ⅲ手术治疗老年二尖瓣病变合并持续性或长期持续性心房颤动[J].中国组织工程研究,2019, 23(22):3562-3569.
[11] WANG H, HAN J, WANG Z, et al. A prospective randomized trial of the cut-and-sew Cox-maze procedure in patients undergoing surgery for rheumatic mitral valve disease.J Thorac Cardiovasc Surg. 2018;155(2): 608-617.
[12] 肖雄,王辉山,韩劲松,等.冷冻消融迷宫术治疗瓣膜病合并心房颤动的围术期管理[J].中国体外循环杂志,2018,16(1):29-32.
[13] COX JL. A brief overview of surgery for atrial fibrillation. Ann Cardiothorac Surg. 2014;3(1):80-88.
[14] COX JL, CHURYLA A, MALAISRIE SC, et al. When Is a Maze Procedure a Maze Procedure? Can J Cardiol. 2018 ;34(11):1482-1491.
[15] ABO-SALEM E, LOCKWOOD D, BOERSMA L, et al. Surgical treatment of atrial fibrillation.J Cardiovasc Electrophysiol.2015;26:1027-1037.
[16] COX JL, SCHUESSLER RB, D'AGOSTINO HJ JR, et al. The surgical treatment of atrial fibrillation. III. Development of a definitive surgical procedure.J Thorac Cardiovasc Surg. 1991;101(4):569-583.
[17] WU CC, CHANG JP, CHEN MC, et al. Long-term results of radiofrequency maze procedure for persistent atrial fibrillation with concomitant mitral surgery.J Thorac Dis. 2017;9(12):5176-5183.
[18] AD N, DAMIANO RJ JR, BADHWAR V, et al. Expert consensus guidelines: Examining surgical ablation for atrial fibrillation.J Thorac Cardiovasc Surg.2017;153(6):1330-1354.e1.
[19] SCHILL MR, MUSHARBASH FN, HANSALIA V, et al. Late results of the Cox-maze IV procedure in patients undergoing coronary artery bypass grafting.J Thorac Cardiovasc Surg.2017;153(5):1087-1094.
[20] YUDA S, NAKATANI S, ISOBE F, et al. Comparative efficacy of the maze procedure for restoration of atrial contraction in patients with and without giant left atrium associated with mitral valve disease.J Am Coll Cardiol.1998;31(5):1097-1102.
[21] AD N, HENRY L, HUNT S, et al. The Cox-Maze III procedure success rate: comparison by electrocardiogram, 24-hour holter monitoring and long-term monitoring.Ann Thorac Surg. 2009;88(1):101-105.
[22] CHOI JB, KIM JH, CHA BK. Outcome of concomitant cox maze procedure with narrow mazes and left atrial volume reduction.Korean J Thorac Cardiovasc Surg.2014;47(4):358-366.
[23] WANG H, HAN J, WANG Z, et al. Efficacy of Cut-and-Sew Surgical Ablation for Atrial Fibrillation in Patients With Giant Left Atria Undergoing Mitral Valve Surgery: A Propensity-Matched Analysis. Semin Thorac Cardiovasc Surg.2019;31(4):796-802.
[24] BRENNAN AP, MARTIN W, ADAMS H, et al. Impact of the Cox-Maze IV Procedure on Left Atrial Mechanical Function.Heart Lung Circ. 2019; 28(12):1835-1840.
[25] JEON CS, SHIM MS, PARK SJ, et al.The absence of atrial contraction as a predictor of permanent pacemaker implantation after maze procedure with cryoablation.Korean J Thorac Cardiovasc Surg. 2017; 50(3):163-170.
[26] GHAVIDEL AA, JAVADPOUR H,SHAFIEE M, et al. Cryoablation for surgical treatment of chronic atrial fibrillation combined with mitral valve surgery: a clinical observation.Eur J Cardiothorac Surg. 2008; 33(6):1043-1048.
[27] HEMELS ME, GU YL, TUINENBURG AE, et al. Favorable long-term outcome of Maze surgery in patients with lone atrial fibrillation.Ann Thorac Surg.2006;81(5):1773-1779.
[28] PARK JH, LEE JS, KO YG, et al. Histological and Biochemical Comparisons between Right Atrium and Left Atrium in Patients with Mitral Valvular Atrial Fibrillation.Korean Circ J. 2014;44(4):233-242.
[29] LÖNNERHOLM S, BLOMSTRÖM P, NILSSON L, et al. Long-term effects of the maze procedure on atrial size and mechanical function. Ann Thorac Surg.2008;85(3):916-920.
[30] WANG M, YIP GW, WANG AY, et al. Peak early diastolic mitral annulus velocity by tissue Doppler imaging adds independent and incremental prognostic value.J Am Coll Cardiol.2003;41(5):820-826.
[31] PATTERSON T, ADAMS H, ALLEN C, et al. Indirect Annuloplasty to Treat Functional Mitral Regurgitation: Current Results and Future Perspectives.Front Cardiovasc Med.2019;6:60.
[32] KHERADVAR A, GROVES EM, SIMMONS CA, et al. Emerging trends in heart valve engineering: Part III. Novel technologies for mitral valve repair and replacement.Ann Biomed Eng.2015;43(4):858-870.
[33] KIM JB, YUN TJ, CHUNG CH, et al. Long-term outcome of modified maze procedure combined with mitral valve surgery: analysis of outcomes according to type of mitral valve surgery.J Thorac Cardiovasc Surg.2010;139(1):111-117.
[34] GILLINOV AM, SIRAK J, BLACKSTONE EH, et al. The Cox maze procedure in mitral valve disease: predictors of recurrent atrial fibrillation.J Thorac Cardiovasc Surg.2005;130(6):1653-1660.
[35] YUDA S, NAKATANI S, KOSAKAI Y, et al. Long-term follow-up of atrial contraction after the maze procedure in patients with mitral valve disease. J Am Coll Cardiol.2001;37(6):1622-1627.
[36] KIM HW, MOON MH, JO KH, et al. Left atrial and left ventricular diastolic function after the maze procedure for atrial fibrillation in mitral valve disease: degenerative versus rheumatic. Indian J Surg.2015;77(1):7-15.
[37] LOARDI C, ALAMANNI F, GALLI C, et al. Surgical Treatment of Concomitant Atrial Fibrillation: Focus onto Atrial Contractility. Biomed Res Int.2015;2015:274817.
[38] LI Z, WANG H, HAN J, et al. Gender differences in fibrosis remodeling in patients with long-standing persistent atrial fibrillation.Oncotarget. 2017;8(32):53714-53729.
[39] SUNDERLAND N, MARUTHAPPU M, NAGENDRAN M. What size of left atrium significantly impairs the success of maze surgery for atrial fibrillation?Interact Cardiovasc Thorac Surg. 2011;13(3):332-338.
[40] GAN GCH, FERKH A, BOYD A, et al. Left atrial function: evaluation by strain analysis. Cardiovasc Diagn Ther.2018;8(1):29-46.
[41] CURTA A, FICHTNER S, WAKILI R, et al. Prospective evaluation of left atrial function and late gadolinium enhancement with 3 T MRI in patients with atrial fibrillation before and after catheter ablation.Int J Cardiovasc Imaging.2019;35(3):499-504. |
| [1] | Wang Zhengdong, Huang Na, Chen Jingxian, Zheng Zuobing, Hu Xinyu, Li Mei, Su Xiao, Su Xuesen, Yan Nan. Inhibitory effects of sodium butyrate on microglial activation and expression of inflammatory factors induced by fluorosis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1075-1080. |
| [2] | Liu Bo, Chen Xianghe, Yang Kang, Yu Huilin, Lu Pengcheng. Mechanism of DNA methylation in exercise intervention for osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 791-797. |
| [3] | Cheng Jun, Tan Jun, Zhao Yun, Cheng Fangdong, Shi Guojia. Effect of thrombin concentration on the prevention of postoperative cerebrospinal leakage by fibrin glue [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 570-575. |
| [4] | Li Li, Ma Li. Immobilization of lactase on magnetic chitosan microspheres and its effect on enzymatic properties [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 576-581. |
| [5] | Li Yanle, Yue Xiaohua, Wang Pei, Nie Weizhi, Zhang Junwei, Tan Yonghai, Jiang Hongjiang. Intramedullary nail fixation versus plate fixation in the treatment of displaced midshaft clavicular fractures in adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 471-476. |
| [6] | Wang Xinting, Xu Dandi, Zhang Junxia, Su Hailong Wang Qi. Stability of load-bearing cross barrier of different arch structures [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3838-3843. |
| [7] | Li Shanshan, You Ran, Guo Xiaoxiao, Zhao Lu, Wang Yanling, Chen Xi. Advances in the mechanisms of optic nerve regeneration [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(23): 3740-3745. |
| [8] | Wang Zhen, Lin Haiqi, He Fei, Lin Wentao. Exercise activates skeletal muscle satellite cells: exercise prevention and treatment for age-related sarcopenia and muscle injury [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(23): 3752-3759. |
| [9] | Zhou Anqi, Tang Yufei, Wu Bingfeng, Xiang Lin. Designing of periosteum tissue engineering: combination of generality and individuality [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3551-3557. |
| [10] | Lang Limin, He Sheng, Jiang Zengyu, Hu Yiyi, Zhang Zhixing, Liang Minqian. Application progress of conductive composite materials in the field of tissue engineering treatment of myocardial infarction [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3584-3590. |
| [11] | Liu Fang, Shan Zhengming, Tang Yulei, Wu Xiaomin, Tian Weiqun. Effects of hemostasis and promoting wound healing of ozone sustained-release hydrogel [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3445-3449. |
| [12] | Liu Jun, Yang Long, Wang Weiyu, Zhou Yuhu, Wu Ying, Lu Tao, Shu Liping, Ma Minxian, Ye Chuan. Preparation and properties of poly3-hydroxybutyrate 4-hydroxybutyrate/polyethylene glycol/graphene oxide tissue-engineered scaffolds [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3466-3472. |
| [13] | Cui Tiantian, Yi Lan, Ouyang Hougan, Wu Huiting, Ouyang Yanchu, Chen Chu. Effect of thermosensitive moxibustion in a rat model of pelvic inflammation based on trifocal focal membrane theory [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(20): 3168-3172. |
| [14] | Xu Hui, Kang Bingxin, Zhong Sheng, Gao Chenxin, Zhao Chi, Qiu Guowei, Sun Songtao, Xie Jun, Xiao Lianbo, Shi Qi. Pressing local acupoints plus adjustion of the knee joint in a sitting position for treating knee osteoarthritis: a randomized controlled trial [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(2): 216-221. |
| [15] | Lu Mingfeng, Zhao Lilian, Xing Jisi, He Lilei, Xu Ting, Wang Changbing. Posttraumatic progression of cartilage degeneration following anterior cruciate ligament reconstruction: a second-look arthroscopic analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(2): 222-227. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||