Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (7): 1056-1065.doi: 10.3969/j.issn.2095-4344.0117
Previous Articles Next Articles
Geometric features of proximal closing wedge osteotomy in the treatment of hallux valgus
Mao Wei, Zhang Jian-zhong, Sun Chao, Wang Xian-jun, Li Hai-tao
- Department of Ankle Surgery, Beijing Tongren Hospital Affiliated to Capital Medical University, Beijing 100016, China
-
Online:2018-03-08Published:2018-03-08 -
Contact:Zhang Jian-zhong, Chief physician, Professor, Department of Ankle Surgery, Beijing Tongren Hospital Affiliated to Capital Medical University, Beijing 100016, China -
About author:Mao Wei, M.D., Attending physician, Department of Ankle Surgery, Beijing Tongren Hospital Affiliated to Capital Medical University, Beijing 100016, China
CLC Number:
Cite this article
Mao Wei, Zhang Jian-zhong, Sun Chao, Wang Xian-jun, Li Hai-tao. Geometric features of proximal closing wedge osteotomy in the treatment of hallux valgus [J]. Chinese Journal of Tissue Engineering Research, 2018, 22(7): 1056-1065.
share this article

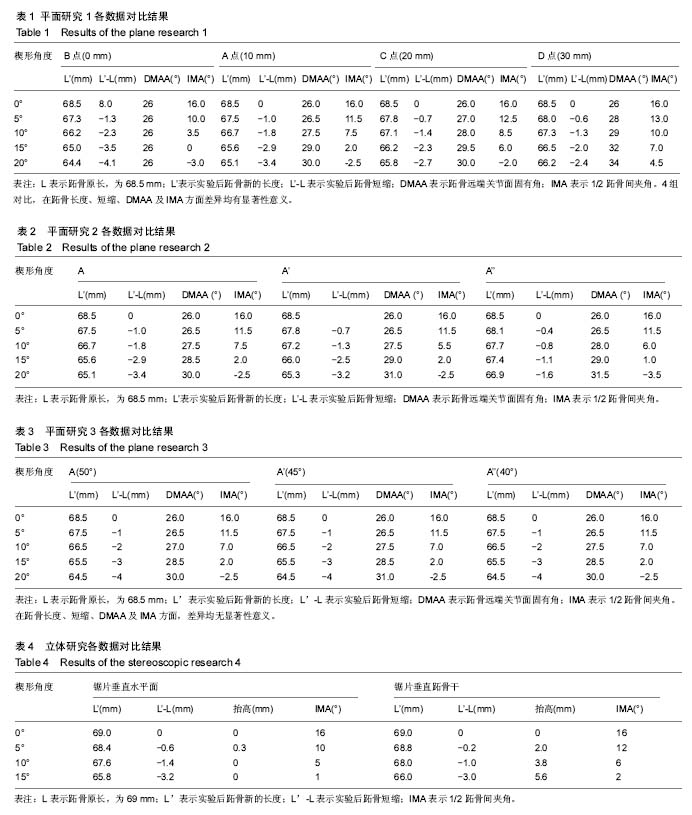
2.1 研究1的结果 IMA对比:组间IAM矫正程度对比,差异均有显著性意义(P < 0.007),见表1。B点为截骨定矫形结果最好,截骨角度为10°,15°时,可以将IMA矫正为3.5°,0°。而A点在相同截骨角度为时,可以将IMA矫正为7.5°,2°,这样的结果理论上符合临床矫形要求。C、D两点的矫正程度较差,在相同的矫正程度下,仅能将IMA理论值矫正到6°,7°,如果患者的IMA>16°,从研究结果看,需要加大截骨的角度,才能满足矫正要求。总体来看,截骨角度相同,楔形截骨的顶点越靠近关节,获得的矫形结果越大。10°-15°的楔形角度,比较适合临床于临床使用。 跖骨长度对比:组间跖骨长度的对比显示各组之间对比差异均有显著性意义(P < 0.009),见表1。选择D点为截骨顶点时,在相同的截骨角度下,所造成的跖骨短缩最小,在截骨角度为10°与 15°时,跖骨短缩分别为1.25 mm与2.00 mm。而B点为顶点时,跖骨长度短缩分别2.3 mm与3.5 mm,两者相差将近1 mm,绝对短缩达2.0-3.0 mm。而A点时,跖骨长度分别短缩1.8 mm与2.9 mm,与B点结果对比,平均相差0.5 mm,比较使用于临床。总体来看,在相同的截骨角度下,楔形截骨的顶点越靠近关节,所造成的跖骨短缩越大。 DMAA对比:组间DMMA对比显示各组组间比较均有统计学意义(P < 0.05),见表1。A点、C点、D点发现在楔形角度为5°,10°,15°,20°的情况下,DMAA逐渐增大,其中A点增大最小,在楔形角度10°-15°范围,DMAA增大在1.5°-3°。D点增大最多分别是3°-6.5°,C点居中。但在B点测得的结果比较特殊,楔形角度不同的情况,测量的DMAA无明显变化,通过进一步测量,得知由于B点在位置上更靠近端,裁剪后的第一跖骨轴线在跖骨近端发生变化明显,但在跖骨远端发生重叠,另外用测量用精度为1°的量角器,对于测量小于1°甚至小于0.5°的数值确实有一定困难。以至在DMAA的测量上,角度始终未发生明显变化。 总体看来,在同样的截骨角度下,越靠近关节,DMAA变化越小;越靠近远端,DMAA越易增大。 2.2 研究2的结果 IMA与DMAA的对比结果:发现3组的结果对比差异无显著性意义(P > 0.05),见表2。 跖骨长度对比结果:3组对比,组内与组间差异均有显著性意义。在相同程度的楔形角度时,选择A点为截骨顶点所造成的跖骨短缩最为明显,如在临床楔形截骨角度10°-15°时,跖骨短缩分别为1.8至2.9 mm。而在A’,A’’点时,短缩分别为1.3至2.5 mm,0.8至1.1 mm。由此推论,初步认为,越是靠近跖骨中线,造成短缩的程度越小,见表2。 本次测量并未在IMA及DMAA方面发现3组之间差异有显著性意义,但通过做图,作者发现,3组在进行5°,10°,15°及20° 时所获得的跖骨轴线确实有不同,但其差别小于1°。由于测量工具精度与测量技术有一定局限性,所以测出的结果在统计分析中未发现明显差异。 2.3 研究3的结果 在跖骨长度,IMA,DMAA方面,以上3组之间的对比差异无显著性意义。在以A点为顶点的楔形截骨,楔形角度相同的情况下,不同的截骨角度,IMA、跖骨长度及DMAA的的变化结果相似。也就是说,截骨顶点固定,楔形截骨角度固定,跖骨长度不会因近端截骨斜率不同而发生明显变化,见表3。 通过研究1,2,3,总结基底闭合截骨存在以下规律:①楔形截骨角度相同时,截骨顶点越靠近端,所获得的矫形越大,DMAA的改变越小,但造成的短缩越明显;②在同一跖骨水平线(与第一跖楔关节内外侧连线平行)任意一点作为截骨顶点,IMA、DMAA改变相似,但截骨顶点越靠近跖骨中线,所引起的跖骨短缩越小;③截骨顶点固定,楔形截骨角度固定,截骨初始倾角不同,IMA,跖骨长度及DMAA结果相同。 在截骨角度相同的情况下,就研究本身而言,针对IMA15°以上的拇外翻患者,截骨角度控制在15°以下,截骨顶点选择A或B点较为合适,矫形后的IMA可以达到一个满意的程度。 2.4 研究4结果 见表4。 IMA对比:截骨锯片垂直于水平面在截骨角度为10°与15°的时候,IMA分别为5°,1°。而后者分别为6°,2°。2组的对比差异有显著性意义(P < 0.05)。 跖骨短缩对比:当锯片垂直于水平面时,在楔形角度位10°与15°时,跖骨分别短缩1.4 mm与3.2 mm。而后者分别是1 mm与3 mm。两者之间的差异有显著性意义(P < 0.05)。跖骨头抬高对比:垂直于跖骨干截骨所得结果明显大于前者,在以15°为楔形截骨时,抬高达到5.6 mm,即使在10°的截骨量下,抬高也达到了3.8 mm。而前者所获得的测量值在统计分析时,差异无显著性意义(P > 0.05)。 "
| [1] Scranton PE Jr.Principles in bunion surgery.J Bone Joint Surg Am. 1983;65(7): 1026-1028.[2] Peterson DA, Zilberfarb JL, Greene MA, et al. Avascular necrosis of the first metatarsal head: incidence in distal osteotomy combined with lateral soft tissue release. Foot Ankle Int. 1994;15(2):59-63.[3] Mann RA,Rudicel S,Graves SC. Repair of hallux valgus with a distal soft-tissue procedure and proximal metatarsalosteotomy. A long-term follow-up.J Bone Joint Surg Am. 1992;74(1):124-129.[4] Coughlin MJ, Grimes S. Proximal metatarsal osteotomy and distal soft tissue reconstruction as treatment for hallux valgus deformity.Keio J Med. 2005;54(2): 60-65.[5] Zettl R, Trnka HJ, Easley M, et al. Moderate to severe hallux valgus deformity: correction with proximal crescentic osteotomy and distal soft-tissue release. Arch Orthop Trauma Surg .2000;120(7): 397-402.[6] Coughlin MJ, Mann RA. Hallux valgus. Surgery of the footand ankle. vol 1, 8th edn. Mosby.1999.[7] Easley ME, Trnka HJ. Current concepts review: halluxvalgus part II: operative treatment. Foot Ankle Int.2007;28(6):748-758.[8] Jahss MH, Troy AI, Kummer FJ. Roentgenographic and mathematical analysis of first metatarsal osteotomies for metatarsus primus varus: a comparative study. Foot Ankle.1985;5:280-321.[9] Kummer FJ. Mathematical analysis of first metatarsal osteotomies. Foot Ankle. 1989;9:281-289.[10] Kummer FJ, Jahss MH. Mathematical analysis of foot and ankle osteotomies. In: Jahss M; editor. Disorders of the foot and ankle: medical and surgical Management. Philadelphia: WB Saunders, 1991:541-563.[11] Palmanovich E, Myerson MS. Correction of moderate and severe hallux valgus deformity witha distal metatarsal osteotomy using anintramedullary plate. Foot Ankle Clin. 2014;19(2):191-201.[12] Park YB, Lee KB, Kim SK, et al. Comparison of distal soft-tissue procedures combined with a distal chevron osteotomy for moderate to severehallux valgus: first web-space versus transarticular approach. J Bone Joint Surg Am. 2013;95(21):e158.[13] Bai LB, Lee KB, Seo CY, et al. Distal chevron osteotomy with distal soft tissue procedure for moderate to severe hallux valgus deformity. Foot Ankle Int. 2010;31(8):683-688.[14] Fakoor M, Sarafan N, Mohammadhoseini P, et al. Comparison of clinical outcomes of scarf and chevron osteotomies and the McBride procedure in the treatment of hallux valgus deformity. Arch Bone Jt Surg. 2014; 2(1): 31-36.[15] Easley ME, Trnka HJ. Current concepts review: hallux valgus part 1: pathomechanics, clinical assessment, and nonoperative management. Foot Ankle Int.2007;28(5):654-659. [16] Lucijanic I, Bicanic G, Sonicki Z, et al. Treatment of hallux valgus with three-dimensional modification ofMitchell’s osteotomy: technique and results. J Am Podiatr Med.2009;.99(2):162-172.[17] Robinson AH, Bhatia M, Eaton C, et al. Prospectivecomparative study of the scarf and Ludloff osteotomies in thetreatment of hallux valgus. Foot Ankle Int.2009;31(10):955-963.[18] Saragas NP. Proximal opening-wedge osteotomy of the firstmetatarsal for hallux valgus using a low profile plate. Foot Ankle Int.2009;30(10): 967-980.[19] Adam SP, Choung SC, Gu Y, et al.Outcomes afterscarf osteotomy for treatment of adult hallux valgus deformity.Clin Orthop Relat Res. 2011; 469(3):854-859.[20] Kinnard P, Gordon D. A comparison between Chevron and Mitchell osteotomies for hallux valgus. Foot Ankle. 1984;4(5):241-243.[21] Loison M. Note sur le traitment chirurgical de hallux valgus d’apres l’etude radiographique de la deformation. Bull Mem Soc Chir. 1901; 27:528.[22] Balacescu J. Un caz de hallux balgus simetric. Rev Cir.1903;7:128.[23] Curda GA, Sorto LA.The McBride bunionectomy with closing abductory wedge osteotomy: a postoperative review. J Am Podiatry Assoc. 1981;71(7):349-355.[24] Graziano TA. Proximal closing wedge osteotomy and adductor tenotomy for treatment of hallux valgus.Foot Ankle. 1989;10(3):191.[25] Resch S, Stenström A, Egund N. Proximal closing wedge osteotomy and adductor tenotomy for treatment of hallux valgus.Foot Ankle. 1989; 9(6):272-280.[26] Toepp FC, Salcedo M. First metatarsal closing base wedge osteotomy using real-time fluoroscopy. Clin Podiatr Med Surg. 1991;8(1):137-151.[27] Christenson C, Jones RO, Basque M, et al. Comparison of oblique closing base wedge osteotomies of the first metatarsal: stripping versus nonstripping of the periosteum. J Foot Surg. 1991;30(2): 107-113.[28] Nigro JS, Greger GM, Catanzariti AR. Closing base wedge osteotomy. J Foot Surg. 1991;30(5):494-505.[29] Coughlin MJ, Carlson RE. Treatment of hallux valgus with an increased distal metatarsal articular angle: evaluation of double and triple first ray osteotomies. Foot Ankle Int. 1999;20(12):762-770.[30] Wagner E, Ortiz C, Gould JS, et al. Proximal oblique sliding closing wedge osteotomy for hallux valgus. Foot Ankle Int. 2013;34(11): 1493-500.[31] Yano K, Ikari K, Iwamoto T, et al. Proximal rotational closing-wedge osteotomy of the first metatarsal in rheumatoid arthritis: clinical and radiographic evaluation of a continuous series of 35 cases. Mod Rheumatol. 2013;23(5):953-958[32] Day T, Charlton TP, Thordarson DB. First metatarsal length change after basilar closing wedge osteotomy for hallux valgus.Foot Ankle Int. 2011;32(5):S513-518.[33] Nedopil A, Rudert M, Gradinger R, et al.Closed wedge osteotomy in 66 patients for the treatment of moderate to severe hallux valgus.Foot Ankle Surg. 2010;16(1): 9-14.[34] John M, Schuberth DPM. The closing base wedge osteotomy for severe hallux valgus.Tech Foot Ankle Surg.2007;6(3):175-184. [35] Neese DJ, Zelichowski JE, Patton GW. Mau osteotomy: an alternative procedure tothe closing abductory base wedge osteotomy.JFoot Surg. 1989;28(4):352-362.[36] Martin DE, Blitch EL. Alternatives to the closing base wedge osteotomy. Clin Podiatr Med Surg. 1996;13(3):515-531.[37] Trnka HJ, Mühlbauer M. Basal closing wedge osteotomy for correction of hallux valgus and metatarsus primus varus: 10- to 22-year follow-up. Foot Ankle Int. 1999;20(3):171-177.[38] Zembsch A, Trnka HJ, Ritschl P. Correction of hallux valgus. Metatarsal osteotomy versus excision arthroplasty. Clin Orthop Relat Res. 2000;(376):183-194.[39] Nyska M, Trnka HJ, Parks BG, et al. Proximal metatarsal osteotomies: A comparative geometric analysis conducted on sawbone models. Foot Ankle Int. 2002;23:938-945.[40] Palladino SJ. Orientation of the first metatarsal base wedge osteotomy: perpendicular to the metatarsal versus weight-bearingsurface.J Foot Surg. 1988;27(4):294-298.[41] Wolke B, Sparmann M.Results after distal Austin and proximal displacement osteotomy: therapy for hallux valgus.Foot Ankle Surg. 1999;5(1):47-52.[42] Denim F, Rees S, Tagoe M. A radiographic evaluation of oblique closing base wedge osteotomies for correction of hallux abductus valgus. Foot. 1998;8:33-37.[43] Easley ME, Darwish HH. Hallux Valgus: Proximal first metatarsal osteotomies. Int Adv Foot Ankle Surg. 2012; 11-25.[44] Fillinger EB, McGuire JW, Hesse DF, et al. Inherent stability of proximal first metatarsal osteotomies: a comparative analysis. J Foot Ankle Surg. 1998;37: 292-302.[45] Trnka HJ, Parks BG, Ivanic G, et al. Six first metatarsal shaft osteotomies: mechanical and immobilization comparisons. Clin Orthop Relat Res. 2000;(381):256-265.[46] Haas Z, Hamilton G, Sundstrom D, et al. Maintenance of correction of first metatarsal closing base wedge osteotomies versus modified lapidus arthrodesis for moderate to severe hallux valgus deformity.J Foot Ankle Surg. 2007;46(5):358-365.[47] Haendel C, Lindholm JA. First metatarsal wedge osteotomies:a retrospective study. JAPA. 1982;72: 550.[48] Denton J, Kuwada GT.Retrospective study of closing wedge osteotomy complications at the base of the first metatarsal with bone screw fixation. J Foot Surg. 1983;22:314.[49] Zlotoff H. Shortening of the first metatarsal following osteotomy and its clinical significance. JAPA.1977;67: 412.[50] Jeremin PJ, Devincentis A, Goller W. Closing base wedge osteotomy: an evaluation of twenty-four cases. J Foot Surg. 1982;21: 316.[51] Schuberth JM, Reilly CH, Gudas CJ. The closing wedge osteotomy: a critical analysis of first metatarsal elevation.JAPA.1984;74:13.[52] Nigro JS, Greger GM, Catanzariti AR. Closing base wedge osteotomy. J Foot Surg. 1991;30: 494.[53] Ruch JA. “First Metatarsal Osteotomies in the Treatment of Hallux Abducto Valgus: Rigi Internal Fixation Techniques-Results and Complications,” in Doctors Hospital Podiatric Education and Research Institute Seminar Manual, ed by ED McGlamry, The Podiatry Institute, Tucker, GA, 1982.[54] Kummer FJ. Mathematical analysis of first metatarsal osteotomies. Foot Ankle.1989;9: 281.[55] Banks AS, Cargill RS 2nd, Carter S, et al. Shortening of the first metatarsal following closing base wedge osteotomy. J Am Podiatr Med Assoc. 1997;87(5): 199-208. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [3] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [4] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [5] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [6] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [7] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [8] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [9] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [10] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [11] | Jie Ke, Deng Peng, Zeng Yirong. Application and comparison of four commonly used methods for patellar height measurement [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3875-3881. |
| [12] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [13] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| [14] | Mo Jianling, He Shaoru, Feng Bowen, Jian Minqiao, Zhang Xiaohui, Liu Caisheng, Liang Yijing, Liu Yumei, Chen Liang, Zhou Haiyu, Liu Yanhui. Forming prevascularized cell sheets and the expression of angiogenesis-related factors [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3479-3486. |
| [15] | Liu Chang, Li Datong, Liu Yuan, Kong Lingbo, Guo Rui, Yang Lixue, Hao Dingjun, He Baorong. Poor efficacy after vertebral augmentation surgery of acute symptomatic thoracolumbar osteoporotic compression fracture: relationship with bone cement, bone mineral density, and adjacent fractures [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3510-3516. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||