Chinese Journal of Tissue Engineering Research ›› 2017, Vol. 21 ›› Issue (23): 3741-3746.doi: 10.3969/j.issn.2095-4344.2017.23.023
Previous Articles Next Articles
Selection of implants and repair in posterolateral fractures of the tibial plateau
Lu Yan-dong1, Li Fang-guo1, Miao Jun2, Sun Jie1
- 1Second Ward of Traumatic Knee Joint, 2Sceond Ward of Spine, Tianjin Hospital, Tianjin 300211, China
-
Online:2017-08-18Published:2017-09-01 -
Contact:Sun Jie, Associate chief physician, Second Ward of Traumatic Knee Joint, Tianjin Hospital, Tianjin 300211, China -
About author:Lu Yan-dong, Attending physician, Second Ward of Traumatic Knee Joint, Tianjin Hospital, Tianjin 300211, China -
Supported by:the National Natural Science Foundation of China, No. 81472140
CLC Number:
Cite this article
Lu Yan-dong, Li Fang-guo, Miao Jun, Sun Jie. Selection of implants and repair in posterolateral fractures of the tibial plateau[J]. Chinese Journal of Tissue Engineering Research, 2017, 21(23): 3741-3746.
share this article
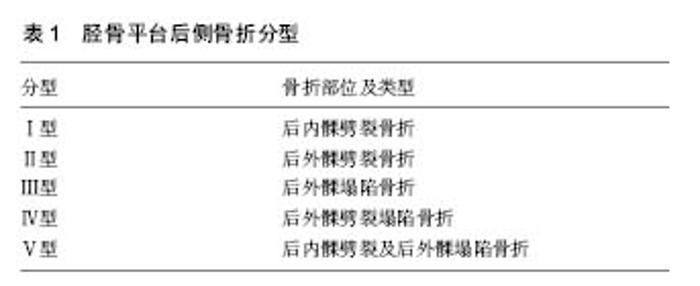
2.1 解剖学特征 胫骨外侧平台比内侧平台位置高,胫骨平台内倾角(与胫骨解剖轴成角)为87°(范围85°-90°),同时胫骨外侧平台呈凸面状,面积较内侧平台小。这一解剖特点使胫骨平台应力呈偏心性分布,外侧平台要承受约40%的膝关节负荷。胫骨外侧平台相对薄弱的软骨下骨密度,人体下肢轴线存在外翻及小腿更容易受向内的暴力,这些原因导致了低能量损伤中外侧平台骨折更常见。当膝关节受到屈曲外翻的暴力时便发生了胫骨平台后外侧髁的骨折[1-2]。胫骨平台后外侧毗邻的解剖结构相对复杂[6]。当胫骨平台后外侧骨折合并腓骨头骨折时容易损伤腓总神经。腘动脉在腓骨颈水平分叉为两支,胫前动脉和胫后动脉。胫前动脉穿过骨间膜上裂孔时被骨间膜纤维固定,移动度小,容易受到外力牵拉而损伤,限制了后外侧切口向远端延伸。其与胫骨外侧平台关节面的距离约为(4.93±0.56) cm,距离腓骨头顶点距离(3.77±0.72) cm,这个距离也限制了后外侧切口固定骨折的钢板长度[7]。 除了腓总神经、胫前动脉之外,后外侧复合体是不能忽视的。作为维持膝关节后外侧稳定的重要结构,其主要为外侧副韧带、腘肌腱复合体、腘腓韧带、弓状韧带和后外侧关节囊组成的复合体。有限制膝关节内翻和胫骨向对于股骨后移外旋的作用。若损伤可致膝关节后外侧不稳定,并加速关节软骨退变[8]。因此,任何对胫骨平台后外侧骨折块进行直接显露、钢板固定等手术操作,均有可能导致后外侧复合体医原性损伤,但目前尚无研究确定这种医原性后外侧复合体损伤对膝关节稳定性有何影响。 2.2 临床分型 目前,对于胫骨平台骨折分型,国内外应用最为广泛的分型仍为Schatzker分型,其主要基于膝关节正、侧位X射线平片,共分为6型。但所有分型中对冠状面的后外侧胫骨平台骨折均没有准确的具体描述。国际内固定研究协会(AO/OTA)制定的AO分型将平台后外侧骨折分为6型:B1.1.4(胫骨外侧平台冠状面后侧劈裂)、B2.2.4(胫骨外侧平台后侧塌陷)、B3.1.2(胫骨外侧平台后外侧劈裂塌陷)和B3.1.4(胫骨外侧平台后内侧劈裂塌陷)。尽管AO分型将骨折形态划分详细,利于学术交流,但难于记忆。 Khan等[9]在1999年提出了一种新的分型方法,胫骨平台后侧骨折被单独列为I型(P型),细分为P1型一后外侧骨折和P2型一后内侧骨折。但无论是AO分型还是Khan分型都只是在形态学上对骨折进行描述,而对骨折的严重程度和预后没有指导意义。随着CT临床应用的普及,国内外专家认为CT可为胫骨平台骨折提出更可靠的分型,尤其是后外侧骨折,CT横断面能非常直观地反映出骨折的特点。Luo等[10]通过CT提出了胫骨平台骨折“三柱理论”,将胫骨平台分为3个柱:内侧柱、外侧柱、后柱。这种分型有助于指导手术入路和内固定方式的选择,对理解整个骨折类型起到了更好的帮助作用。但其对后外侧骨折划归为后柱骨折,无具体细分,对于后外侧骨折缺少了具体的临床指导作用。 Chen等[11-12]综合了Schatzker分型及三柱分型,结合X射线平片、CT和三维重建图像,提出了胫骨平台后侧骨折新分型,其分型体系包括5型(表1):Ⅰ型、Ⅱ型、Ⅲ型、Ⅳ型、Ⅴ型。该分型对胫骨平台骨折的特点进行了详细描述,且方便于临床手术方案的制定。但该分型将后侧骨折从胫骨平台骨折中孤立出来,对于复杂的胫骨平台骨折来说,该分型又不具备指导意义。一个科学的分型,应遵从评判受伤机制,指导治疗方案,评判预后,方便统计与交流。探索更加合理的能全面反应胫骨平台后外侧骨折损伤情况,又能体现周围软组织损伤程度的分型,目前依然是迫切需要解决的问题。"

2.3 形态学特征 随着CT临床应用的普及,国内外专家意识到,通过CT可以对胫骨平台后外侧骨折块形态学特征进行综合分析,有助于临床医师对于此类骨折有更进一步的认识[13-18]。高翔等[13]统计了264例胫骨平台骨折患者资料,39例存在后外侧骨折块(14.8%)。该骨折线偏于冠状位,骨折线轴向角度为-43°-62°,平均22°;其面积占整个胫骨平台面积的8%-32%,平均14.1%;其矢状位角度为58°-97°,平均76°;其高度为18-42 mm,平均28 mm;其平均移位2-19 mm,平均10.48 mm。此研究指出了后外侧骨折块的形态学特点包括骨折线偏于冠状位,矢状位角度较大,累及关节面的面积较小。Sohn等[15]统计分析了278例胫骨平台骨折患者CT资料,后外侧骨折有84例(44.2%),外侧主要骨折块角度为-56.02°-72.44°,平均12.69°,后侧主要骨折块角度为-39.47°-61.10°,平均19.13°,对角线距离为15.03-59.14 mm,平均 32.75 mm,外侧前后距离为-11.18-31.17 mm,平均10.22 mm,后侧皮质高度为10.84-63.93 mm,平均31.12 mm,矢状位骨折块角度为41.69°-105.12°,平均78.48°,受累面积平均为 522.18 mm(14.5%),大约占平台外侧关节面面积的1/3。由此可见,胫骨平台后外侧骨折大部分是需要手术固定的。 2.4 手术入路 鉴于胫骨平台后外侧骨折的特殊性,目前,国内外专家并未对此类型骨折手术入路达成共识,争议较大,各有优缺点。 2.4.1 膝关节前侧入路 治疗胫骨平台外侧骨折,最经典和标准的手术入路为前外侧入路。这一入路无重要血管、神经走行,能充分暴露外侧平台,保证内植物表明有良好的软组织覆盖。术中需将胫前肌剥离骨面至关节囊水平,切开冠状韧带,抬起外侧半月板,显露外侧平台塌陷劈裂关节面。结合顶棒和克氏针临时固定复位后关节面,最后支撑锁定钢板固定。术中对于后外侧骨折的处理,通常将前外侧开窗或前内侧开窗撬拨塌陷的后外侧关节面,通过C型臂透视判断复位质量[19-21]。 冯刚等[22]采用前外侧联合前内侧入路治疗累及后外侧骨折的C3型胫骨平台骨折15例。其特点是利用锁定螺钉的角稳定特性,前外侧锁定钢板支撑固定外侧柱、后内侧柱;前内侧锁定钢板支撑固定内侧柱及后外侧柱。15例患者骨折均愈合良好,无膝关节不稳,无复位丢失,无发生感染等并发症。Sassoon等[23]经前外侧入路通过腓骨干自体移植治疗11例胫骨平台后外侧关节面压缩性骨折的患者。其特点是显露后外侧塌陷关节面和明确腓骨取骨位置后,于胫骨外侧干骺端皮质开骨窗。C型臂监视下,将自体腓骨干通过骨窗植入,撬拨垫起塌陷的后外侧关节面,同时腓骨尽量在压缩的关节面下方后侧,复位满意后,剪除过长的腓骨,使它与胫骨外侧皮质平行。最后通过螺钉或钢板固定胫骨外侧皮质和移植的腓骨。随访结果显示,3例患者术后出现并发症,1例创伤性关节炎,1例感染,1例复位丢失,外翻畸形。前侧入路的优点是避免了膝关节后外侧血管、神经以及后外侧复合体等复杂解剖的困扰。然而缺点也是明显的,由于股骨髁和外侧半月板的阻挡,胫骨平台后外侧显露不充分,且平台外侧关节面呈凸起不规则,术中不能直视下复位后外侧骨折块,只能通过C型臂透视下定位,这就不利于骨折的解剖复位。因此,这种入路在临床实践中受到了很大的限制。 2.4.2 膝关节后外侧入路 腓骨头截骨入路:由于腓骨头的阻挡,当发生胫骨平台后外侧骨折时,术中往往不能直视下显露后外侧骨折块。腓骨头截骨入路使术者更清晰的显露胫骨平台外侧和后外侧关节面,更利于对后外侧骨折块的复位及固定[24]。根据后外侧关键骨折块的特点,通过膝关节前外侧、外侧及后外侧入路均可施行腓骨头截骨[24-25]。庄岩等[26]采用经腓骨头截骨入路治疗17例累及后外侧胫骨平台骨折,平均随访时间18个月,其中1例术后出现腓总神经损伤症状,术后2周恢复。18例均达到骨性愈合,未出现复位高度丢失,关节功能满意。Solomon等[24]采用腓骨头截骨入路治疗8例后外侧胫骨平台骨折,8例均未出现腓总神经损伤等并发症,均达到骨性愈合。Yu等[25]采用腓骨头截骨入路治疗82例外侧及后外侧胫骨平台骨折,随访结果显示,6例出现膝关节周围疼痛,3例出现平台高度丢失,3例出现膝关节外侧不稳定。全部病例均未出现腓总神经损伤及腓骨头骨不连等并发症。腓骨头截骨入路的优势在于术中经腓骨截骨,胫骨平台后外侧骨折暴露更加充分,更便于对骨折块的复位及固定。这一入路的局限性在于可能出现腓总神经损伤和腓骨骨不连,此入路术中需要解剖并游离腓总神经,腓骨头截断及固定,手术操作相对复杂,且钢板位于上胫腓关节之间,对于该关节的微动存在影响。因此,腓骨头截骨仍存在争议,仍需大样本的研究来证实。 不需腓骨头截骨入路:尽管膝关节后外侧的解剖复杂,毗邻重要的血管、神经,以及膝关节后外侧复合体等结构,不需腓骨头截骨的后外侧入路可能有损伤血管、神经的风险,但国内外专家仍将更多的目光投入到这一入路。因为生物力学实验表明,采用后外侧入路直接放置支撑钢板固定,可以取得可靠的稳定性[27]。近年来,国内外有诸多关于后外侧入路治疗累及胫骨平台后外侧骨折的报道(图1)[28-38]。Carlson[28]于2005年采用后内侧、后外侧双“S”形切口入路治疗胫骨平台后侧骨折,并取得了满意的疗效。该入路中后外侧“S”形切口位于股二头肌上方,术中需将股二头肌后方的腓总神经显露和向外侧牵开保护。Tao等[29]采用改良倒“L”形切口治疗11例胫骨平台后外侧骨折,1例术后伤口出现血性渗出外,余均无感染,无复位丢失等并发症发生。这一入路是充分显露股二头肌与腓肠肌肌间隙,游离腓总神经并保护,深层通过腓肠肌、腘肌和比目鱼肌间隙暴露后外侧胫骨平台骨折。Liu等[30]应用改良的后外侧入路治疗9例单纯后外侧胫骨平台骨折。全部病例均获得满意的疗效,术后胫骨平台关节面复位好6例,中等3例,术后2年均未出现关节面复位丢失,未出现关节不稳等并发症。这一入路是采取后外侧直切口,切口起自腘窝皮肤横纹下1 cm,沿腓骨头内侧缘1.5 cm直向下。这样,腓总神经位于切口的外上方,腘血管位于切口的内侧,术中无需显露腓总神经。他们认为对于单纯的胫骨平台后外侧骨折,该入路降低腓总神经损伤的风险,又能直视下复位固定骨折,是一较好的入路固定方式。然而,对于胫骨平台前外侧及后外侧同时累及的骨折来说,无论是“S”形切口,还是后外侧“L”形、直切口,均不能满足骨折的显露及固定。 Frosch等[31]针对上述骨折,于2010年提出了一个新的手术入路,及扩展的后外侧切口,此入路将前外侧入路与后外侧入路相结合设计而成,采用侧卧位或漂浮体位,术中通过前外侧肌间隙复位固定前外侧平台骨折,通过后外侧肌间隙复位固定后外侧平台骨折。优点是通过一个切口,一个体位即能完成两处骨折的复位和固定,缩短了手术时间,降低了手术并发症。此后,相关学者对这种入路进行了改良,仍获得了满意效果[32-34]。但认为该入路也存在一定的局限性,这种入路受到切口的限制,对于后外侧骨折块,需从前外侧翻书样打开劈裂的骨折块,显露后外侧骨折块,通过前外和后外两个间隙同时进行复位后外侧骨折,然后于后外侧支撑钢板固定,增加了手术难度,同样有损伤腓总神经的风险。 2.4.3 后内侧入路 膝关节后内侧入路更适合于胫骨平台后侧柱骨折或累及后外侧的复杂胫骨平台骨折[39-42]。切口起自膝关节的后外侧腘窝中间,沿朗格线向内侧延长,至腘窝内侧边缘时转向下延伸。充分牵开皮肤筋膜,在近端注意保护小隐静脉和腓肠内侧皮神经,在远端要保护隐神经和大隐静脉。分离腓肠肌内侧头并拉向外侧,同时用霍夫曼拉钩保护好腘窝后部的血管神经束。软组织分离必须在腘肌下进行,以免损伤到腘窝重要的血管神经束。即可充分显露胫骨平台后侧,手术视野良好,骨折复位及钢板固定相对容易。Qiu等[39]利用后内侧倒“L”形或联合其他入路治疗95例胫骨平台患者,78例增加前外侧入路处理外侧柱骨折。术后并发症率为4.2%,有2例患者术中分别发生腘动脉损伤和腓肠肌内侧头滋养动脉损伤,还有 2 例患者术后发生局部皮肤麻木。结果表明:后内侧倒“ L”入路治疗胫骨平台后柱和内侧柱骨折,安全可靠,并发症发生率低。作者认为这可能与胫骨平台前外侧的腓肠肌和比目鱼肌较宽厚有关,血供丰富,且可完全覆盖内固定物。Berber等[40]介绍了一种改良后内侧入路治疗伴有后内侧或后外侧劈裂骨块的复杂胫骨平台骨折。作者认为该入路能在直视下对关节面进行直接复位和内固定置入,能对后外侧角骨折进行复位固定,同时能对腘部血管神经损伤进行修复。同时也总结了该入路的优缺点;优点:对冠状位劈裂骨块直接复位的良好暴露;俯卧位重力有助于后方骨折脱位的复位;倒L形切口便于显露后外侧骨折和软组织结构;拉开胫前动脉能达到后外侧骨折块更远端固定;使支撑钢板的放置更具力学优势;拉开腓肠肌内侧头使腘部血管修复得到更好暴露;切口远端延伸(劈开比目鱼肌)可以在远端暴露胫后动脉;舒适的手术体位。劣势:俯卧位麻醉不利;如需联合前外侧入路,则需术中变换体位;解剖较复杂,容易损伤血管神经;必须术前计划,如需要独立的外侧复位,内侧固定螺钉要短,以免影响外侧复位;对腓肠肌的操作存在晚期马蹄足畸形风险。因此,多数专家认为后内侧切口更多的适用于辅助治疗复杂胫骨平台骨折累及后内侧、或者整个后侧柱的骨块[42]。 2.5 内固定材料 针对于治疗胫骨平台后外侧骨折的不同手术入路,内固定材料也需要“量身定做”,通常前侧入路选用前外侧4.5 mm解剖锁定钢板,前内侧T型锁定钢板,6.5 mm松质骨螺钉[22,27,30];由于胫骨平台后外侧髁的解剖轮廓不规则,干骺端区域弯度较大,临床上尚无商品化的精确塑形,于后外侧髁相匹配的解剖型钢板。因此,后侧入路通常选择3.5 mm桡骨远端T形或L形解剖钢板,术中需视情况塑形后再进行固定[29,32]。钢板的长度通常应在5 cm以内,以避免损伤胫前动脉。目前,大多数生物力学实验表明,后外侧支撑钢板的生物力学优势更明显[43-45],可以有效避免骨折块的剪切力造成的复位丢失。因此,对于累及后外侧的胫骨平台骨折,后外侧支撑钢板固定是一个不错的选择。 "

| [1] Bhattacharyya T, McCarty LP 3rd, Harris MB, et al. The posterior shearing tibial plateau fracture: treatment and results via a posterior approach. J Orthop Trauma. 2005; 19:305-310.[2] Chang SM,Zheng HP,Li HF,et al.Treatment of isolated posterior coronal fracture of the lateral tibial plateau through posterolateral approach for direct exposure and buttress plate fixation. Arch Orthop Trauma Surg. 2009; 129(7): 955-962.[3] Higgins TF,Klatt J,Bachus KN.Biomechanical analysis of bicondylar tibial plateau fixation: How does lateral locking plate fixation compare to dual plate fixation.J Orthop Trauma. 2007; 21(5): 30l-306.[4] Zhu Y, Yang G, Luo CF,et al. Computed tomography-based Three-Column Classification in tibial plateau fractures: introduction of its utility and assessment of its reproducibility. J Trauma Acute Care Surg. 2012; 73(3): 731-737.[5] Heidari N,Lidder S,Grechenig W,et al. The risk of injury to the anterior tibial artery in the posterolateral approach to the tibia plateau:acadaver study.J Orthop Trauma. 2013;27(4): 221-225.[6] Sun H,Luo CF,Yang G,et al.Anatomical evaluation of the modified posterolateral approach for posterolateral tibial plateau fracture.Eur J Orthop Surg Traumatol. 2013; 23(7): 809-818.[7] 胡孙君,张世民,张英琪,等. 胫骨平台后外侧象限骨折手术入路的深层解剖及后外侧与后内侧比较[J]. 中国临床解剖学杂志, 2015,33(5): 497-501.[8] Pacheco RJ,Ayre CA,Bollen SR.Posterolateral comer injuries of the knee:a serious injury commonly missed.J Bone Joint Surg Br. 2011; 93(2): 194-197.[9] Khan RM,Khan SH,Ahmad AJ,et al. Tibial plateau fractures. A new classification scheme. Clin Orthop Relat Res. 2000; 375: 231-242.[10] Luo CF,Sun H,Zhang B,et al.Three-column fixation for complex tibial plateau fractures.J Orthop Trauma. 2010; 24(11): 683-692.[11] Chen HW,Chen CQ,Yi XH. Posterior tibial plateau fracture: a new treatment-oriented classification and surgical management. Int J Clin Exp Med. 2015; 8(1): 472-479.[12] 陈红卫,赵钢生,王子阳,等. 胫骨平台后髁骨折的CT分型[J]. 中华医学杂志.2011; 91(3): 180-184.[13] 高翔,李杭,郑强,等.胫骨后外侧平台骨折的CT形态学研究[J]. 中华骨科杂志. 2014;34(7)709-716.[14] Barei DP,O’Mara Tj,Taitsman LA,et al.Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns.J Orthop Trauma. 2008; 22(3): 176-182.[15] Sohn HS,Yoon YC,Cho JW,et al.Incidence and fracture morphology of posterolateral fragments in lateral and bicondylar tibial plateaufractures.J Orthop Trauma. 2015; 29(2):91-97.[16] Zhu Y,Meili S,Dong MJ,et al. Pathoanatomy and incidence of the posterolateral fractures in bicondylar tibial plateau fractures: a clinical computed tomography-based measurement and the associated biomechanical model simulation. Arch Orthop Trauma Surg. 2014; 134(10): 1369-1380.[17] Xiang G,Zhi-Jun P,Qiang Z,et al.Morphological characteristics of posterolateral articular Fragments in tibial plateau fractures.Orthopedics. 2013; 36(10): e1256-e1261.[18] Zhai Q,Luo C,Zhu Y,et al.Morphological characteristics of split-depression fractures of the lateral tibial plateau(Schatzker type II):a computer-tomography-based study.Int Orthop. 2013; 37(5): 911-917.[19] Kenneth AE. Split depression posterolateral tibial plateau fracture direct open reduction and internal fixation. Tech Knee Surg. 2005; 4(4): 257-262.[20] 刘立峰,蔡锦力,梁进. 胫骨平台后外壁骨折的治疗[J]. 中国骨伤,2003,16(6): 338-339.[21] Hsieh CH. Treatment of the posterolateral tibial plateau fractures using the anterior surgical approach.J Biomed Sci. 2010; 6(4): 316-320.[22] 冯刚,潘志军,李杭,等. 双锁定钢板交叉支撑固定治疗累及后外侧的C3型胫骨平台骨折[J]. 中华骨折杂志,2014; 34(7): 695-702.[23] Sassoon AA,Torchia Me,Cross Ww,et al.Fibular shaft allograft support of posterior joint depression in tibial plateau fractures.J Orthop Trauma. 2014; 28(7): e169-e175.[24] Solomon LB,Stevenson AW,Baird RP,et al.Posterolateral transfibular approach to tibial plateau fractures:technique,results,and rationale.J Orthop Trauma. 2010; 24(8): 505-514.[25] Yu B,Han K,Zhan C,et al.Fibular head osteotomy:a new approach for the treatment of lateral or posterolateral tibial plateau fractures.Knee. 2010; 17(5): 313-318.[26] 庄岩,王鹏飞,张堃,等. 经腓骨截骨入路治疗胫骨平台后外侧骨折的疗效观察. 中华骨科杂志. 2012; 32(8): 732-738.[27] Zhang W,Luo CF,Putnis S,et al.Biomechanical analysis of four different fixations for the posterolateral shearing tibial plateau fracture. Knee. 2012; 19(2): 94-98.[28] Carlson DA.Posterior bicondylar tibial plateau fractures.J Orthop Trauma. 2005; 19(2): 73-78.[29] Tao J,Hang DH,Wang QG,et al.The posterolateral shearing tibial plateau fracture: treatment and results via a modified posterolateral approach.Knee. 2008; 15(6): 473-479.[30] Liu GY,Xiao BP,Luo CF, et al.Results of a modified posterolateral approach for the isolated posterolateral tibial plateau fracture. Indian J Orthop. 2016; 50(2):117-122.[31] Frosch KH,Balcarek P,Walde T,et al.A new posterolateral approach without fibula osteotomy for the treatment of tibial plateau fractures.J Orthop Trauma. 2010; 24(8): 515-520.[32] Chen HW,Luo CF. Extended anterolateral approach for treatment of posterolateral tibial plateau fractures improves operative procedure and patient prognosis. Int J Clin Exp Med. 2015; 8(8): 13708-13715.[33] 朱海涛,王文跃,王俭,等. 外后侧弧形切口双肌间隙入路治疗胫骨后外侧平台塌陷骨折[J]. 中华骨科杂志, 2014; 34(7): 703-708.[34] Chen HW, Zhou SH, Liu GD,et al. An extended anterolateral approach for posterolateral tibial plateau fractures. Knee Surg Sports Traumatol Arthrosc. 2015; 23(12):3750-3755.[35] Hu SJ,Chang SM,Zhang YQ,et al.The anterolateral supra-fibular-head approach for plating posterolateral tibial plateau fractures: A novel surgical technique. Injury. 2016; 47(2): 502-507.[36] 刘观燚,罗从风,赵华国,等. 改良后外侧入路治疗孤立性后外侧胫骨平台骨折[J]. 中华创伤骨科杂志,2015,17(10): 895-898.[37] He X,Ye P,Hu Y,et al.A posterior inverted L-shaped approach for the treatment of posterior bicondylar tibial plateau fractures.Arch Orthop Trauma Surg. 2013;133(1): 23-28.[38] Solomon LB,Stevenson AW,Lee YC,et al.Posterolateral and antero-lateral approaches to unicondylar posterolateral tibial plateau fractures:a comparative study.Injury. 2013; 44(11): 1561-1568.[39] Qiu WJ,Zhan Y,Sun H,et al. A posterior reversed L-shaped approach for the tibial plateau fractures—A prospective study of complications (95 cases) . Injury. 2015; 46: 1613–1618.[40] Berber R,Lewis CP,Copas D,et al.Postero-medial approach for complex tibial plateau injuries with a postero-medial or postero-lateral shear fragment. Injury. 2014; 45(4): 757-765.[41] Sun H,Zhai QL,Xu YF,et al.Combined approaches for fixation of Schatzker type II tibial plateau fractures involving the posterolateralcolumn: a prospective observational cohort study. Arch Orthop Trauma Surg. 2015; 135(2): 209-221.[42] Chang SM,Hu SJ,Zhang YQ,et al.A surgical protocol for bicondylar four-quadrant tibial plateau fractures. Int Orthop. 2014;38(12): 2559-2564.[43] Jiang R,Luo CF,Zeng BF.Biomechanical evaluation of different fixation methods for fracture dislocation involving the proximal tibia.Clin Biomech(Bristol,Avon). 2008; 23(8): 1059-1064.[44] Zeng ZM,Luo CF,Putnis S,et al.Biomechanical analysis of posteromedial tibial plateau split fracture fixation.Knee. 2011; 18(1): 51-54.[45] 张巍,罗从风,曾炳芳.四种不同内固定治疗胫骨平台后外侧剪应力骨折的生物力学研究[J].中华创伤骨科杂志. 2010; 12(11): 1069-1073. |
| [1] | Xue Yadong, Zhou Xinshe, Pei Lijia, Meng Fanyu, Li Jian, Wang Jinzi . Reconstruction of Paprosky III type acetabular defect by autogenous iliac bone block combined with titanium plate: providing a strong initial fixation for the prosthesis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1424-1428. |
| [2] | Zhuang Zhikun, Wu Rongkai, Lin Hanghui, Gong Zhibing, Zhang Qianjin, Wei Qiushi, Zhang Qingwen, Wu Zhaoke. Application of stable and enhanced lined hip joint system in total hip arthroplasty in elderly patients with femoral neck fractures complicated with hemiplegia [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1429-1433. |
| [3] | Yao Xiaoling, Peng Jiancheng, Xu Yuerong, Yang Zhidong, Zhang Shuncong. Variable-angle zero-notch anterior interbody fusion system in the treatment of cervical spondylotic myelopathy: 30-month follow-up [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1377-1382. |
| [4] | Jiang Huanchang, Zhang Zhaofei, Liang De, Jiang Xiaobing, Yang Xiaodong, Liu Zhixiang. Comparison of advantages between unilateral multidirectional curved and straight vertebroplasty in the treatment of thoracolumbar osteoporotic vertebral compression fracture [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(9): 1407-1411. |
| [5] | Li Wei, Zhu Hanmin, Wang Xin, Gao Xue, Cui Jing, Liu Yuxin, Huang Shuming. Effect of Zuogui Wan on bone morphogenetic protein 2 signaling pathway in ovariectomized osteoporosis mice [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1173-1179. |
| [6] | Wang Jing, Xiong Shan, Cao Jin, Feng Linwei, Wang Xin. Role and mechanism of interleukin-3 in bone metabolism [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1260-1265. |
| [7] | Xiao Hao, Liu Jing, Zhou Jun. Research progress of pulsed electromagnetic field in the treatment of postmenopausal osteoporosis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1266-1271. |
| [8] | Wu Bingshuang, Wang Zhi, Tang Yi, Tang Xiaoyu, Li Qi. Anterior cruciate ligament reconstruction: from enthesis to tendon-to-bone healing [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(8): 1293-1298. |
| [9] | An Weizheng, He Xiao, Ren Shuai, Liu Jianyu. Potential of muscle-derived stem cells in peripheral nerve regeneration [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1130-1136. |
| [10] | Tian Chuan, Zhu Xiangqing, Yang Zailing, Yan Donghai, Li Ye, Wang Yanying, Yang Yukun, He Jie, Lü Guanke, Cai Xuemin, Shu Liping, He Zhixu, Pan Xinghua. Bone marrow mesenchymal stem cells regulate ovarian aging in macaques [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 985-991. |
| [11] | Hu Wei, Xie Xingqi, Tu Guanjun. Exosomes derived from bone marrow mesenchymal stem cells improve the integrity of the blood-spinal cord barrier after spinal cord injury [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 992-998. |
| [12] | Gao Yujin, Peng Shuanglin, Ma Zhichao, Lu Shi, Cao Huayue, Wang Lang, Xiao Jingang. Osteogenic ability of adipose stem cells in diabetic osteoporosis mice [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 999-1004. |
| [13] | Wu Weiyue, Guo Xiaodong, Bao Chongyun. Application of engineered exosomes in bone repair and regeneration [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1102-1106. |
| [14] | Zhou Hongqin, Wu Dandan, Yang Kun, Liu Qi. Exosomes that deliver specific miRNAs can regulate osteogenesis and promote angiogenesis [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1107-1112. |
| [15] | Zhang Jinglin, Leng Min, Zhu Boheng, Wang Hong. Mechanism and application of stem cell-derived exosomes in promoting diabetic wound healing [J]. Chinese Journal of Tissue Engineering Research, 2022, 26(7): 1113-1118. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||