Chinese Journal of Tissue Engineering Research ›› 2013, Vol. 17 ›› Issue (5): 938-944.doi: 10.3969/j.issn.2095-4344.2013.05.026
Previous Articles Next Articles
Infection after anterior cruciate ligament reconstruction
Xu Chang-ming, Yang Le, Hu Chuan-liang, Hu Yu-hua
- Department of Orthopedics, Jiangsu Provincial Corps Hospital, Chinese People’s Armed Police Force, Yangzhou 225003, Jiangsu Province, China
-
Received:2012-07-26Revised:2012-09-13Online:2013-01-29Published:2013-01-29 -
About author:Xu Chang-ming☆, Doctor, Associate chief physician, Department of Orthopedics, Jiangsu Provincial Corps Hospital, Chinese People’s Armed Police Force, Yangzhou 225003, Jiangsu Province, China sea009@126.com
CLC Number:
Cite this article
Xu Chang-ming, Yang Le, Hu Chuan-liang, Hu Yu-hua. Infection after anterior cruciate ligament reconstruction[J]. Chinese Journal of Tissue Engineering Research, 2013, 17(5): 938-944.
share this article
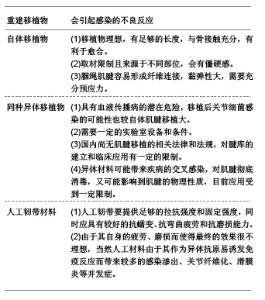
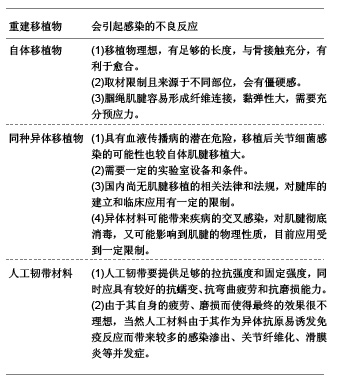
2.1 纳入文献基本情况 中文文献中仅有1篇文章对前交叉韧带重建术后感染进行了详细的探讨[6]。英文文献对这一问题报道较多,主要探讨了前交叉韧带重建术后感染的原因[8,9]、临床表现[10, 20]、诊断[11,17,21-32]、治疗方法[17,18,33-41]以及预后[11]。 2.2 结果描述 2.2.1 前交叉韧带重建后感染的原因 细菌污染手术工具或者韧带移植物是导致前交叉韧带重建术后感染的最常见原因[8-10]。Maria等[11]发现他们的患者前交叉韧带重建术感染率比较高的原因是由于移植物板上的凝固酶隐性葡萄球菌导致的。他们发现尽管消毒是用合格的高压锅进行的,但是移植物板缝合夹的金属部分和橡胶板之间的缝隙并没有得到满意的消毒。 异体移植物的应用可能和前交叉韧带重建后感染有关[12],因为异体移植物在植入关节内之前有一定的污染率,但也有的作者认为这种污染并不一定导致前交叉韧带重建后感染[13],因而无需特殊处理[14]。也有的作者认为异体移植物的应用并不增加前交叉韧带重建后的感染率[15]。移植物固定的方式和重建后感染之间可能有一定的关系。Fong等[16]发现他们所有患者的膝关节术后感染可能都是由胫骨隧道侧导致的,也就是由关节外到关节内的感染,这是因为不管采用什么方法固定胫骨侧,所有的胫骨隧道都受到了感染。Daniel等[17]发现采用腘绳肌腱重建前交叉韧带的术后感染率较高。他们认为这可能是和移植物的固定方法或者额外的软组织剥离有关,不一定和使用某种移植物之间具有相关性。Barker等[18]则认为采用自体腘绳肌腱重建前交叉韧带的术后感染率要比采用自体或者异体骨-髌腱-骨重建前交叉韧带的术后感染率要高。在采用腘绳肌腱重建的手术中,移植物的长度比较短,这就使得有一部分缝线被留在关节腔内。他们认为较短的移植物和关节内的缝合材料都有可能导致炎性反应。 还有的医生对前交叉韧带重建后常规使用引流管和术后感染的相关性进行了研究。Matava等[19]发现那些常规使用引流管的医生的感染率(0.27%)是那些不使用引流的医生的两倍多(0.10%)。考虑到前交叉韧带重建手术后的感染率本来就比较低,所以这个数据不但有很高的临床价值,而且更有统计学意义。 2.2.2 前交叉韧带重建后感染的临床表现 典型的前交叉韧带重建术后感染的症状和普通的化脓性关节炎的症状类似。大多数患者会出现化脓性关节炎的典型症状,具体包括:发热,膝关节肿胀、疼痛、局部红肿,切口处有液体渗出,局部皮温增高,有的人还感到全身不适。但是,Maria等[11]发现有的前交叉韧带重建术后感染的病例并没有感染的典型表现,有的患者的情况很容易和普通的重建后改变相混淆。但是,应该注意的是一般的术后疼痛持续几天就会缓解,如果重建后患者疼痛持续时间过长或者术后疼痛并不随时间的推移而逐步改善,这时要考虑化脓性关节炎的可能性[20]。所以Maria等[11]建议:对于那些术后膝关节功能逐步恢复的患者,如果之后又出现了发热、局部疼痛、肿胀、膝关节僵硬、身体不适等情况,应该及时到医院就诊,以明确是否出现了前交叉韧带重建重建后感染。 重建移植物引起感染的不良反应:"

2.2.3 前交叉韧带重建后感染的诊断和鉴别诊断 如果前交叉韧带重建后出现关节感染的典型临床症状,那么诊断前交叉韧带重建术后感染并不困难。但是很多作者注意到,前交叉韧带术后感染的诊断并不一定很容易,典型的膝关节感染的症状常常会被一些术后反应所掩盖。为了排除化脓性关节炎,Maria等[11]推荐患者作实验室检查(比如C-反应蛋白和血沉)。在那些膝关节或者髋关节感染的患者中,这两个实验室指标都被发现明显增高。由于手术创伤,那些没有并发术后感染的前交叉韧带重建患者在术后短期血沉和C-反应蛋白也会出现增高[17],重建后2周时C-反应蛋白恢复至正常水平,而血沉在重建后4周内一直保持轻度增高的状态。这种情况可能会干扰感染的早期诊断。 膝关节穿刺是诊断术后感染的最好方法[21]。关节液外观、白细胞计数和革兰氏染色是早期正确诊断感染的可靠手段[22]。发生前交叉韧带重建后感染时,关节液外观一般为混浊脓性、稠厚,有时呈黄色,关节液中往往有多形核白细胞浓聚,这些结果强烈提示化脓性感染。如果关节液中能培养出致病菌,那么可以确定患者为前交叉韧带重建术后化脓性感染。 导致前交叉韧带重建术后化脓性感染的常见病菌有: 金黄色葡萄球菌(Staphylococcus aureus) [18, 23, 24]。 表皮葡萄球菌(Staphylococcus epidermidis)。 胨链球菌(Peptostreptococcus)。 肠杆菌属(Enterobacter)[17,25]。 其他致病菌还有: 耐甲氧西林的金黄色葡萄球菌(methicillinresistant Staphylococcus aureus)。 丹毒丝菌(Erysipelothrix rhusiopathiae)[26]。 丙酸杆菌(Propionibacteriaceae)。 小韦荣菌(Veillonella parvula)。 产气荚膜梭菌(Clostridium perfringens)[8,27]。 结核菌(Mycobacterium tuberculosis)[28]。 真菌(Fungi)[29,30]。 分枝杆菌(Mycobacterium fortuitum)[31]。 里昂葡萄球菌(Staphylococcus lugdunensis)[32]。 但是由于抗生素的使用、培养条件的限制以及致病菌的活性等原因,关节液的培养不一定会有阳性结果。如果关节液培养阴性,那么可以根据粒细胞计数增高、血沉、 C-反应蛋白水平以及感染的临床表现来诊断感染[22]。 2.2.4 前交叉韧带重建后感染的治疗 前交叉韧带重建术后化脓性关节炎的治疗目标是: 第一,保护关节软骨。 第二,保护移植物[33]。目前,85%的外科医师选择静脉使用敏感的抗生素、膝关节灌洗并保留移植物作为自体移植物重建前交叉韧带术后感染的首选治疗方法[34],对于异体移植物,有64%的医生采用同样的处理方法[18]。如果初次治疗后效果不明显,仍然有39%的医生继续静脉使用敏感抗生素结合关节灌洗、保留移植物作为最常用的治疗方法。 合适的抗生素治疗是非常重要的治疗措施。一个动物试验的结果显示:金黄色葡萄球菌导致的膝关节化脓性关节炎,如果在感染症状出现后7 d内仍然没有进行合理的治疗,那么关节软骨将会丢失一半以上的黏多糖和胶原蛋白[35-37]。Daniel等[17]则报道:实验室检查完善后,按照感染科医生的会诊意见,所有患者都根据经验给予静脉抗生素治疗,选择头孢唑啉或万古霉素。在他们的11例患者中有6例患者初期使用的抗生素是细菌耐药的。11例患者中,仅1例患者的细菌对头孢唑啉敏感,其余10例患者的细菌对万古霉素敏感。抗生素使用的疗程因患者的实验室结果而不尽相同。Viola等[38]报道,抗生素治疗后一般5-30 d(平均14.4 d)时临床体征首先缓解,而实验室结果稍晚些时候才变得正常。实验室检查结果正常后两三天,停用抗生素。 除了抗生素治疗之外,为了减少严重并发症的发生(比如退变性关节炎、骨髓炎),还需要对感染的膝关节作适当的减压治疗[39-41]。对于化脓性关节炎,Daniel等[17]建议采用关节镜灌洗和关节镜下清创术。关节镜可以很容易地达到膝关节的所有部位,同时可以使膝关节减压,充分清创,对移植物的完整性以及有无感染迹象作评估,破坏膝关节内的纤维粘连,从而减少术后出现膝关节强直的可能。关节镜术中往往可以看到移植物的表面一般都有一薄层的纤维覆盖,其他并没有什么明显的异常,移植物的张力一般比较好[42-43]。 以往有的医生认为前交叉韧带移植物可能是感染的发源地[44],所以他们认为如果经治疗后感染的症状和体征一直存在,那么在第二次手术时应该将移植物取出。2011年Demira?等[45]报道他们采用长期抗生素(6周)、关节镜下清创、保留移植物和内固定物以及适当康复治疗处理前交叉韧带重建后发生感染的7例患者,获得了满意的疗效。感染控制后所有膝关节的Lachman试验均为阴性,轴移试验:3例为阳性,4例为阴性。和健腿相比,单腿纵向跳跃距离是对侧的78%(63%-100%),单腿水平跳跃距离是对侧的72%(88%-93%)。Monaco等[46-47]采用类似的方法也取得了良好的临床效果,而且他们的所有患者都恢复到术前和感染前的运动水平。 2.2.5 预后 Maria等[11]对他们的两组患者进行对比发现,每个感染的膝关节的评分等于或者小于对照组的没有感染的膝关节的评分。感染的患者有更多的主观症状,具体包括[48-50]:活动受限,膝关节屈曲受限。他们还发现感染患者的膝关节功能差的不是由移植物失败导致的,而是由于感染导致关节软骨破坏引起的。"

| [1] Musso AD, McCormack RG. Infection after ACL reconstruction: what happens when cultures are negative? Clin J Sport Med. 2005;15(5):381-384.[2] Zalavras CG, Patzakis MJ, Tibone J, et al. Treatment of persistent infection after anterior cruciate ligament surgery. Clin Orthop Relat Res. 2005;439:52-55. [3] Jameson SS, Dowen D, James P, et al: Complications following anterior cruciate ligament reconstruction in the English NHS. Knee. 2012;19(1):14-19.[4] 汪群力,云雄,陈奇,等.关节镜下腘绳肌腱及生物界面螺钉重建交叉韧带27例[J].中国组织工程研究与临床康复,2010,14(52): 9831-9834.[5] 谭志超,蔡立民,邓怀东,等.关节镜下自体胭绳肌肌腱移植重建膝前交叉韧带的临床观察[J].岭南现代临床外科,2011,11(2): 131-133,145. [6] 王成,敖英芳,王健全,等.关节镜下前交叉韧带重建术后膝关节感染的临床诊断与治疗[J].中华外科杂志,2008,46(10): 745-748.[7] Frank M, Schmucker U, David S, et al. Devastating femoral osteomyelitis after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2008;16(1):71-74.[8] Kurokouchi K, Takahashi S, Yamada T, et al. Methicillin-resistant Staphylococcus aureus-induced septic arthritis after anterior cruciate ligament reconstruction. Arthroscopy. 2008;24(5):615-617.[9] Nakayama H, Yagi M, Yoshiya S, et al. Micro-organism colonization and intraoperative contamination in patients undergoing arthroscopic anterior cruciate ligament reconstruction. Arthroscopy. 2012;28(5):667-671.[10] Tuman J, Diduch DR, Baumfeld JA, et al. Joint infection unique to hamstring tendon harvester used during anterior cruciate ligament reconstruction surgery. Arthroscopy. 2008;24(5):618-620.[11] Schollin-Borg M, Michaëlsson K, Rahme H. Presentation, outcome, and cause of septic arthritis after anterior cruciate ligament reconstruction: a case control study. Arthroscopy. 2003;19(9):941-947.[12] Romanini E, D'Angelo F, De Masi S, et al. Graft selection in arthroscopic anterior cruciate ligament reconstruction. J Orthop Traumatol. 2010;11(4):211-219.[13] Centeno JM, Woolf S, Reid JB 3rd, et al. Do anterior cruciate ligament allograft culture results correlate with clinical infections? Arthroscopy. 2007;23(10):1100-1103.[14] Fowler JR, Truant AL, Sewards JM. The incidence of and clinical approach to positive allograft cultures in anterior cruciate ligament reconstruction. Clin J Sport Med. 2011;21(5):402-4. [15] Katz LM, Battaglia TC, Patino P, et al. A retrospective comparison of the incidence of bacterial infection following anterior cruciate ligament reconstruction with autograft versus allograft. Arthroscopy. 2008;24(12):1330-1335.[16] Fong SY, Tan JL. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction. Ann Acad Med Singapore. 2004;33(2):228-234.[17] Judd D, Bottoni C, Kim D, et al. Infections following arthroscopic anterior cruciate ligament reconstruction. Arthroscopy. 2006;22(4):375-384.[18] Barker JU, Drakos MC, Maak TG, et al. Effect of graft selection on the incidence of postoperative infection in anterior cruciate ligament reconstruction. Am J Sports Med. 2010;38(2):281-286.[19] Matava MJ, Evans TA, Wright RW, et al. Septic arthritis of the knee following anterior cruciate ligament reconstruction: results of a survey of sports medicine fellowship directors. Arthroscopy. 1998;14(7):717-725.[20] Armstrong RW, Bolding F, Joseph R. Septic arthritis following arthroscopy: clinical syndromes and analysis of risk factors. Arthroscopy. 1992;8(2):213-223.[21] Burks RT, Friederichs MG, Fink B, et al. Treatment of postoperative anterior cruciate ligament infections with graft removal and early reimplantation. Am J Sports Med. 2003; 31(3):414-418.[22] Binnet MS, Bas K. Risk and outcome of infection after different arthroscopic anterior cruciate ligament reconstruction techniques. Arthroscopy. 2007;23(8):862-868. [23] Kurokouchi K, Takahashi S, Yamada T, et al. Methicillin-resistant Staphylococcus aureus-induced septic arthritis after anterior cruciate ligament reconstruction. Arthroscopy. 2008;24(5):615-617.[24] Pola E, Logroscino G, Santis VD, et al: Onset of Berger Disease After Staphylococcus aureus Infection: Septic Arthritis After Anterior Cruciate Ligament Reconstruction. Arthroscopy. 2003;19(4):E29.[25] Van Tongel A, Stuyck J, Bellemans J, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: a retrospective analysis of incidence, management and outcome. Am J Sports Med. 2007;35(7):1059-1063.[26] Allianatos PG, Tilentzoglou AC, Koutsoukou AD. Septic arthritis caused by Erysipelothrix rhusiopathiae infection after arthroscopically assisted anterior cruciate ligament reconstruction. Arthroscopy. 2003;19(3):E26.[27] Farooq AH, Dabke HV, Majeed MA, et al. Clostridial wound infection following reconstruction of the anterior cruciate ligament using bone-patella-bone autograft. J Coll Physicians Surg Pak. 2007;17(6):369-370.[28] Nag HL, Neogi DS, Nataraj AR, et al. Tubercular infection after arthroscopic anterior cruciate ligament reconstruction. Arthroscopy. 2009;25(2):131-136. [29] Muscolo DL, Carbo L, Aponte-Tinao LA, et al. Massive bone loss from fungal infection after anterior cruciate ligament arthroscopic reconstruction. Clin Orthop Relat Res. 2009; 467(9): 2420-2425.[30] Sun L, Zhang L, Wang K, et al. Fungal osteomyelitis after arthroscopic anterior cruciate ligament reconstruction: a case report with review of the literature. Knee. 2012;19(5):728-731. [31] Oh HL, Chen DB, Seeto BG, et al. Mycobacterium fortuitum infection after anterior cruciate ligament reconstruction using a polylactic acid bioabsorbable screw: Case report. Knee. 2010;17(2):176-178.[32] Mei-Dan O, Mann G, Steinbacher G, et al. Septic arthritis with Staphylococcus lugdunensis following arthroscopic ACL revision with BPTB allograft. Knee Surg Sports Traumatol Arthrosc. 2008;16(1):15-18.[33] Indelli PF, Dillingham M, Fanton G, et al. Septic arthritis in postoperative anterior cruciate ligament reconstruction. Clin Orthop Relat Res. 2002;(398):182-188. [34] Demira? B, Unal OK, Ozakin C. Graft retaining debridement in patients with septic arthritis after anterior cruciate ligament reconstruction. Acta Orthop Traumatol Turc. 2011;45(5):342-347.[35] Smith RL, Schurman DJ, Kajiyama G, et al. The effect of antibiotics on the destruction of cartilage in experimental infectious arthritis. J Bone Joint Surg Am. 1987;69(7): 1063-1068.[36] Kim YM, Joo YB. Clinical Presentation of Staphylococcus epidermidis Septic Arthritis Following Anterior Cruciate Ligament Reconstruction. Knee Surg Relat Res. 2012;24(1): 46-51.[37] Vertullo CJ, Quick M, Jones A, et al. A surgical technique using presoaked vancomycin hamstring grafts to decrease the risk of infection after anterior cruciate ligament reconstruction. Arthroscopy. 2012;28(3):337-342. [38] Viola R, Marzano N, Vianello R. An unusual epidemic of Staphylococcus-negative infections involving anterior cruciate ligament reconstruction with salvage of the graft and function. Arthroscopy. 2000;16(2):173-177. [39] De la Garza-Castro S, González-Rivera CE, Vilchez-Cavazos JF, et al. Septic knee arthritis caused by Pseudomonas aeruginosa after anterior cruciate ligament reconstruction in an adolescent athlete. Acta Ortop Mex. 2012;26(1):53-56.[40] Wang C, Ao Y, Wang J, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: a retrospective analysis of incidence, presentation, treatment, and cause. Arthroscopy. 2009;25(3):243-249. [41] Wang C, Ao YF, Wang JQ, et al. Diagnosis and management of septic arthritis after arthroscopic anterior cruciate ligament (ACL) reconstruction. Zhonghua Wai Ke Za Zhi. 2008;46(10): 745-748. [42] 谭志超,蔡立民,邓怀东,等.关节镜下LARS人工韧带重建膝前交叉韧带的临床观察[J].现代医院,2011,11(2):36-38.[43] 马晓生,姜建元. 移植物取出并早期再次重建治疗前交叉韧带重建术后感染[J]. 中华创伤骨科杂志,2012,14(11):935-939.[44] Outcomes of Williams RJ 3rd, Laurencin CT, Warren RF, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction. Diagnosis and management. Am J Sports Med. 1997;25(2):261-267.[45] Demira? B, Unal OK, Ozakin C. Graft retaining debridement in patients with septic arthritis after anterior cruciate ligament reconstruction. Acta Orthop Traumatol Turc. 2011;45(5): 342-347.[46] Monaco E, Maestri B, Vadalà A, et al. Return to sports activity after postoperative septic arthritis in ACL reconstruction. Phys Sportsmed. 2010;38(3):69-76.[47] Monaco E, Maestri B, Labianca L, et al. Clinical and radiological outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction. J Orthop Sci. 2010; 15(2):198-203. [48] Papastergiou SG, Koukoulias NE, Koumis P, et al. Brucella arthritis of the knee, 1 year after revision of anterior cruciate ligament reconstruction. BMJ Case Rep. 2011 Apr 1;2011. [49] Sajovic M, Ni? Ar GL, Dernovš Ek MZ. Septic arthritis of the knee following anterior cruciate ligament reconstruction. Orthop Rev (Pavia). 2009;1(1):e3. [50] Gérard R, Tandé D, Hery G, et al. Septic arthritis after arthroscopic cruciate ligament reconstruction: in vitro comparison of the behavior of two types of interference screws towards the Staphylococcus aureus adherence. Rev Chir Orthop Reparatrice Appar Mot. 2008;94(6):541-545.[51] 徐青镭,李飞,邵顺健,等. 前交叉韧带重建术后感染的诊断分型与分期治疗[J].中华创伤骨科杂志,2012,14(11):935-939.[52] 刘武,王瑞华. 关节镜下膝关节前交叉韧带自体半腱肌股薄肌重建术后并发症的研究进展[J]. 微创医学,2012,7(1):65-68.[53] 侯存强,周宪华,孙磊, 等. 骨骼肌对前交叉韧带重建腱性移植物关节内愈合效果的影响[J]. 中国骨科临床与基础研究杂志, 2012,4(2):133-137.[54] 郑佳鹏,翟文亮,丁真奇,等. 富血小板血浆与异体脱蛋白骨复合物颗粒促进前交叉韧带重建术后腱骨愈合的临床研究[J]. 中国骨与关节损伤杂志,2012,27(4):304-306.[55] 贝涛,赵劲民,丁晓飞,等. 前交叉韧带重建中可吸收螺钉与金属螺钉两种固定方式比较的系统评价[J]. 中国组织工程研究与临床康复,2011,15(52):9817-9822.[56] McAllister DR, Parker RD, Cooper AE, et al. Outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction. Am J Sports Med. 1999;27(5):562-570.[57] Williams RJ 3rd, Laurencin CT, Warren RF, et al. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction. Diagnosis and management. Am J Sports Med. 1997;25(2):261-267.[58] Torres-Claramunt R, Pelfort X, Erquicia J, et al. Knee joint infection after ACL reconstruction: prevalence, management and functional outcomes. Knee Surg Sports Traumatol Arthrosc. 2012 Oct 27.[59] Myers P,Logan M,Stokes A,et al.Bioabsorbable versus titanium interference screws with hamstring autograft in anterior cruciate ligament reconstruction:a prospective randomized trial with 2-year follow-up.Arthroscopy.2008;24(7):817-823.[60] 董向辉,凌鸣,冯伟楼,等. 关节滑液对兔前交叉韧带重建后腱骨愈合生物力学和组织学的影响[J]. 中国组织工程研究,2012, 16(11): 1937-1940.[61] 杨伟毅,练文兴,曹学伟,等. 肌力强化训练对膝关节前交叉韧带重建术后伴股四头肌萎缩患者肌力恢复的疗效[J]. 实用医学杂志,2012,28(13):2221-2223. |
| [1] | Xu Feng, Kang Hui, Wei Tanjun, Xi Jintao. Biomechanical analysis of different fixation methods of pedicle screws for thoracolumbar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1313-1317. |
| [2] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [3] | Du Xiupeng, Yang Zhaohui. Effect of degree of initial deformity of impacted femoral neck fractures under 65 years of age on femoral neck shortening [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1410-1416. |
| [4] | Zhang Shangpu, Ju Xiaodong, Song Hengyi, Dong Zhi, Wang Chen, Sun Guodong. Arthroscopic suture bridge technique with suture anchor in the treatment of acromioclavicular dislocation [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1417-1422. |
| [5] | Liang Yan, Zhao Yongfei, Xu Shuai, Zhu Zhenqi, Wang Kaifeng, Liu Haiying, Mao Keya. Imaging evaluation of short-segment fixation and fusion for degenerative lumbar scoliosis assisted by highly selective nerve root block [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1423-1427. |
| [6] | Yuan Jiawei, Zhang Haitao, Jie Ke, Cao Houran, Zeng Yirong. Underlying targets and mechanism of Taohong Siwu Decoction in prosthetic joint infection on network pharmacology [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1428-1433. |
| [7] | Zhou Jihui, Li Xinzhi, Zhou You, Huang Wei, Chen Wenyao. Multiple problems in the selection of implants for patellar fracture [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1440-1445. |
| [8] | Chen Junming, Yue Chen, He Peilin, Zhang Juntao, Sun Moyuan, Liu Youwen. Hip arthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures in older adults: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1452-1457. |
| [9] | Hu Kai, Qiao Xiaohong, Zhang Yonghong, Wang Dong, Qin Sihe. Treatment of displaced intra-articular calcaneal fractures with cannulated screws and plates: a meta-analysis of 15 randomized controlled trials [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1465-1470. |
| [10] | Ji Zhixiang, Lan Changgong. Polymorphism of urate transporter in gout and its correlation with gout treatment [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(8): 1290-1298. |
| [11] | Wan Ran, Shi Xu, Liu Jingsong, Wang Yansong. Research progress in the treatment of spinal cord injury with mesenchymal stem cell secretome [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1088-1095. |
| [12] | Jiao Hui, Zhang Yining, Song Yuqing, Lin Yu, Wang Xiuli. Advances in research and application of breast cancer organoids [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1122-1128. |
| [13] | Xu Yulin, Shen Shi, Zhuo Naiqiang, Yang Huilin, Yang Chao, Li Yang, Zhao Heng, Zhao Lu. Biomechanical comparison of three different plate fixation methods for acetabular posterior column fractures in standing and sitting positions [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 826-830. |
| [14] | Liu Shaohua, Zhou Guanming, Chen Xicong, Xiao Keming, Cai Jian, Liu Xiaofang. Influence of anterior cruciate ligament defect on the mid-term outcome of fixed-bearing unicompartmental knee arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 860-865. |
| [15] | Hou Guangyuan, Zhang Jixue, Zhang Zhijun, Meng Xianghui, Duan Wen, Gao Weilu. Bone cement pedicle screw fixation and fusion in the treatment of degenerative spinal disease with osteoporosis: one-year follow-up [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(6): 878-883. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||