Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (20): 3117-3123.doi: 10.3969/j.issn.2095-4344.1192
Whether direct anterior approach for total hip arthroplasty is a risk factor of eccentric reaming to the anterior column of the acetabulum?
Su Lianbin1, 2, Feng Eryou1, Zhang Yiyuan1, 2, Zhuo Youguang1, 2, Xiao Lili1, Wang Wulian1, Lin Feitai1
- 1Department of Joint Surgery, FuZhou Second Hospital of Xiamen University, Fuzhou 350007, Fujian Province, China; 2Medical College of Xiamen University, Xiamen 361005, Fujian Province, China
-
Online:2019-07-18Published:2019-07-18 -
Contact:Zhang Yiyuan, Chief physician, Professor, Master’s supervisor, Department of Joint Surgery, FuZhou Second Hospital of Xiamen University, Fuzhou 350007, Fujian Province, China; Medical College of Xiamen University, Xiamen 361005, Fujian Province, China -
About author:Su Lianbin, Master candidate, Department of Joint Surgery, FuZhou Second Hospital of Xiamen University, Fuzhou 350007, Fujian Province, China; Medical College of Xiamen University, Xiamen 361005, Fujian Province, China -
Supported by:the Natural Science Foundation of Fujian Province, No. 2017J01333 (to FEY)
CLC Number:
Cite this article
Su Lianbin, Feng Eryou, Zhang Yiyuan, Zhuo Youguang, Xiao Lili, Wang Wulian, Lin Feitai. Whether direct anterior approach for total hip arthroplasty is a risk factor of eccentric reaming to the anterior column of the acetabulum?[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(20): 3117-3123.
share this article

Quantitative analysis of participants With parameters of 10 cases in preparatory work, and according to formula of estimation of sample size in group design, the results showed that at least 26 cases would be needed to reach statistical significance. Therefore, we chose eligible 30 cases from October 2015 to December 2017, and 575 cases of THA were completed in our department. Comparison of the measurement parameters between PLA and DAA groups There was no significant difference in all preoperative parameters (P > 0.05) (Table 2). The postoperative CSA of the anterior column in the DAA group was larger than that in the PLA group (P=0.04). No significant differences were observed for the CSA of the anterior-posterior, posterior column, height of the anterior and posterior column, acetabular diameter and anteversion postoperation (P > 0.05) between two groups. Meanwhile, there was no significant difference in the bone loss perioperatively (Table 3)."
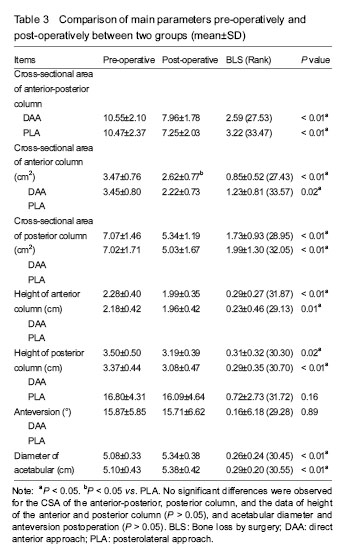
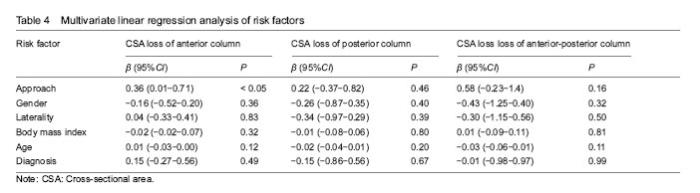
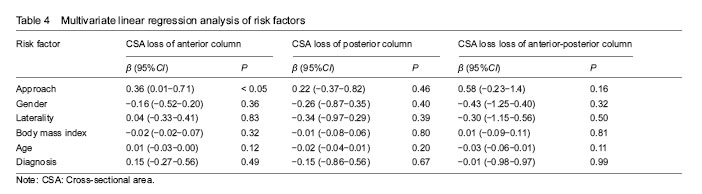
Comparison of perioperative parameters between PLA or DAA groups The postoperative cross-sectional area of the anterior and posterior column of the acetabulum, and the height of the anterior and posterior column in the two groups were less than those at baseline (P < 0.05), the acetabular diameter was larger than that at baseline (P < 0.01), and the anteversion showed no significant difference (P=0.89) (Table 3). Multivariate linear regression analysis The approach was a risk factor of the CSA loss of anterior column (β=0.36, 95%CI: 0.01-0.71, P < 0.05), and not significantly risk factor for CSA loss of posterior (β=0.22, 95%CI: -0.37-0.82, P=0.46), and anterior-posterior column (β=0.58, 95%CI: -0.23-1.40, P=0.16). The gender, laterality, body mass index, age, primary diagnosis were not associated with CSA loss of anterior, posterior and anterior-posterior column (P > 0.05) (Table 4)."
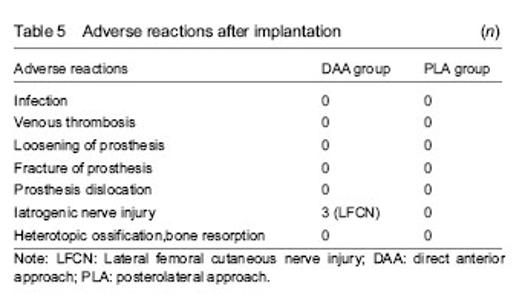
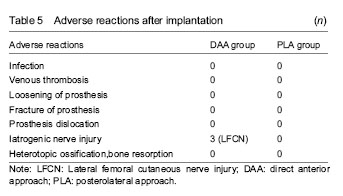
Adverse reactions Three patients in the DAA group suffered from lateral femoral cutaneous nerve injury and all recovered at postoperative 6 months. No adverse reactions such as infection, prosthesis loosening and rupture, venous thrombosis, heterotopic ossification or bone resorption occurred (Table 5). "
| [1] Moretti V, Post Z. Surgical approaches for total hip arthroplasty Indian J Orthop. 2017;51(4):368-376.[2] Jordan J, Helmick J, Renner B, et al. Prevalence of hip symptoms and radiographic and symptomatic hip osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project. J Rheumatol. 2009;36(4):809-815. [3] Maradit Kremers H, Larson DR, Crowson CS, et al. Prevalence of total hip and knee replacement in the United States. J Bone Joint Surg Am. 2015;97(17):1386-1397.[4] Singh JA. Epidemiology of knee and hip arthroplasty: a systematic review. Open Orthop J. 2011;16(5):80-85. [5] Petis S, Howard JL, Lanting BL, et al. Surgical approach in primary total hip arthroplasty: anatomy, technique and clinical outcomes. Can J Surg. 2015;58(2):128-139. [6] Connolly KP, Kamath AF. Direct anterior total hip arthroplasty: literature review of variations in surgical technique.World J Orthop. 2016;7(1):38-43. [7] Ji W, Stewart N. Fluoroscopy assessment during anterior minimally invasive hip replacement is more accurate than with the posterior approach. Int Orthop. 2016;40(1):21-27. [8] Zhang YJ, Li J, Qi K, et al. Comparison of efficacy and safety between the anterior and the posterior approaches to total hip arthroplasty. Beijing Da Xue Xue Bao. 2017;49(2):201-205. [9] Lin TJ, Bendich I, Ha AS, et al. A comparison of radiographic outcomes after total hip arthroplasty between the posterior approach and direct anterior approach with intraoperative fluoroscopy. J Arthroplasty. 2017;32(2):616-623. [10] Post ZD, Orozco F, Diaz-Ledezma C,et al. Direct anterior approach for total hip arthroplasty: indications, technique, and results. J Am Acad Orthop Surg. 2014;22(9):595-603. [11] Radoicic D, Zec V, Elassuity WI, et al. Patient's perspective on direct anterior versus posterior approach total hip arthroplasty. Int Orthop. 2018;42(12):2771-2775. [12] Nistor DV, Caterev S,. Bolboaca SD, et al. Transitioning to the direct anterior approach in total hip arthroplasty. Is it a true muscle sparing approach when performed by a low volume hip replacement surgeon? Int Orthop. 2017;41(11):2245-2252. [13] Seng BE, Berend KR, Ajluni AF, et al. Anterior-supine minimally invasive total hip arthroplasty: defining the learning curve. Orthop Clin North Am. 2009;40(3):343-350. [14] Kobayashi H, Homma Y. Surgeons changing the approach for total hip arthroplasty from posterior to direct anterior with fluoroscopy should consider potential excessive cup anteversion and flexion implantation of the stem in their early experience. Int Orthop.2016;40(9):1813-1819. [15] Barton C, Kim PR. Complications of the direct anterior approach for total hip arthroplasty. Orthop Clin North Am. 2009;40(3):371-375. [16] Chechik O, Khashan M, Lador R, et al. Surgical approach and prosthesis fixation in hip arthroplasty world wide. Arch Orthop Trauma Surg. 2013;133(11):1595-600.[17] Holst DC, Yang CC. Surgical anatomy of the direct anterior approach for total hip arthroplasty. Ann Joint. 2018;3:23-23.[18] Uemura K, Takao M. Sakai T, et al. Volume increases of the gluteus maximus, gluteus medius, and thigh muscles after hip arthroplasty. J Arthroplasty. 2016;31(4):906-912. [19] Xu D, Koyama H, Furuhashi H, et al. Comparison of hip muscle volume between fit-and-fill stem and tapered-wedge stem after total hip arthroplasty using the anterolateral approach. J Orthop Sci. 2017;22(6):1102-1106. [20] Tongdee T, Keawaen P, Tongdee R. Evaluation of standard liver volume in adult Thai population using CT volumetric measurement. J Med Assoc Thai. 2013;96(2):217-2124.[21] Dandachli W, Islam UL, Tippettr R, et al. Analysis of acetabular version in the native hip: comparison between 2D axial CT and 3D CT measurements. Skeletal Radiol. 2011;40(7):877-883. [22] Pankal A, Mittal A, Chawla A. The validity and reproducibility of cross table radiographs compared with CT scans for the measurement of anteversion of the acetabular component after total hip arthroplasty. Bone Joint J. 2017;99-b(8):1006-1011. [23] Nomura T, Naito M, Nakamura Y, et al. An analysis of the best method for evaluating anteversion of the acetabular component after total hip replacement on plain radiographs. Bone Joint J. 2014;96-b(5):597-603. [24] Shemesh S, Robinson S, Keswani A, et al. The accuracy of digital templating for primary total hip arthroplasty: is there a difference between direct anterior and posterior approaches? J Arthroplasty. 2017;32(6):1884-1889. [25] Hartford JM, Knowles SB. Risk factors for perioperative femoral fractures: cementless femoral implants and the direct anterior approach using a fracture table. J Arthroplasty. 2016;31(9): 2013-2018.[26] Wang Z, Hou JZ, Wu CH, et al. A systematic review and meta-analysis of direct anterior approach versus posterior approach in total hip arthroplasty. J Orthop Surg Res. 2018;13(1): 229-240. [27] Cheng TE, Wallis JA, Taylor NF, et al. A prospective randomized clinical trial in total hip arthroplasty-comparing early results between the direct anterior approach and the posterior approach. J Arthroplasty. 2017;32(3):883-890. [28] Cadossi M, Sambri A, Tedesco G, et al. Anterior approach in total hip replacement. Orthopedics. 2017;40(3):e553-556.[29] Pilliar RM, Leeand J, Maniatopoulos C. Observations on the effect of movement on bone ingrowth into porous-surfaced implants. Clin Orthop Relat Res. 1986;(208):108-113. [30] Fehring K, Owen A. Kurdin A, et al. Initial stability of press-fit acetabular components under rotational forces. J Arthroplasty. 2014;29(5):1038-1042. [31] Markel D, Horaand N, Grimm M. Press-fit stability of uncemented hemispheric acetabular components: a comparison of three porous coating systems. Int Orthop. 2002;26(2):72-75. [32] Saleh K, Bear B, Wright T, et al. Initial stability of press-fit acetabular components: an in vitro biomechanical study. Am J Orthop. 2008;37(10):519. [33] Kim YH. Acetabular Cup Revision. Hip Pelvis. 2017;29(3):155-158.[34] Lingaraj K, Teoand YH, Bergman N. The management of severe acetabular bone defects in revision hip arthroplasty using modular porous metal components. J Bone Joint Surg Br. 2009;91(12):1555-1560. [35] Meneghini RM, Elston AS, Chen AF, et al. Direct anterior approach: risk factor for early femoral failure of cementless total hip arthroplasty: a multicenter study. J Bone Joint Surg Am. 2017;99(2):99-105. [36] Homma Y, Baba T, Sano K, et al. Lateral femoral cutaneous nerve injury with the direct anterior approach for total hip arthroplasty. Int Orthop. 2016;40(8):1587-1593. [37] Eto S, Hwang K, Huddleston JI, et al. The direct anterior approach is associated with early revision total hip arthroplasty. J Arthroplasty. 2017;32(3):1001-1005. [38] Ozaki Y, Homma Y, Baba T, et al. Spontaneous healing of lateral femoral cutaneous nerve injury and improved quality of life after total hip arthroplasty via a direct anterior approach. J Orthop Surg. 2017;25(1) 1-7. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zhang Yu, Tian Shaoqi, Zeng Guobo, Hu Chuan. Risk factors for myocardial infarction following primary total joint arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1340-1345. |
| [3] | Zhang Chong, Liu Zhiang, Yao Shuaihui, Gao Junsheng, Jiang Yan, Zhang Lu. Safety and effectiveness of topical application of tranexamic acid to reduce drainage of elderly femoral neck fractures after total hip arthroplasty [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1381-1386. |
| [4] | Wang Haiying, Lü Bing, Li Hui, Wang Shunyi. Posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis: prediction of functional prognosis of patients based on spinopelvic parameters [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1393-1397. |
| [5] | Zhang Chao, Lü Xin. Heterotopic ossification after acetabular fracture fixation: risk factors, prevention and treatment progress [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1434-1439. |
| [6] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [7] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [8] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [9] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [10] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [11] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [12] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [13] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [14] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [15] | Liu Jianyou, Jia Zhongwei, Niu Jiawei, Cao Xinjie, Zhang Dong, Wei Jie. A new method for measuring the anteversion angle of the femoral neck by constructing the three-dimensional digital model of the femur [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(24): 3779-3783. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||