Chinese Journal of Tissue Engineering Research ›› 2019, Vol. 23 ›› Issue (12): 1908-1914.doi: 10.3969/j.issn.2095-4344.1128
Previous Articles Next Articles
Clinical complications and analysis of internal fixation through the second iliac crest screw technique
He Chenyang1, Wu Yonggang2, Zhao Yan3
- 1Graduate School of Inner Mongolia Medical University, Hohhot 010000, Inner Mongolia Autonomous Region, China; 2Bayannur Hospital, Bayannur 015000, Inner Mongolia Autonomous Region, China; 3the Second Affiliated Hospital of Inner Mongolia Medical University, Hohhot 010000, Inner Mongolia Autonomous Region, China
-
Online:2019-04-28Published:2019-04-28 -
Contact:Wu Yonggang, MD, Bayannur Hospital, Bayannur 015000, Inner Mongolia Autonomous Region, China -
About author:He Chenyang, Master candidate, Graduate School of Inner Mongolia Medical University, Hohhot 010000, Inner Mongolia Autonomous Region, China -
Supported by:the National Natural Science Foundation of Inner Mongolia Autonomous Region, No. 2016MS08132 (to ZY)
CLC Number:
Cite this article
He Chenyang, Wu Yonggang, Zhao Yan. Clinical complications and analysis of internal fixation through the second iliac crest screw technique [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(12): 1908-1914.
share this article
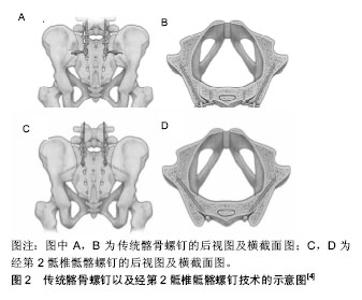
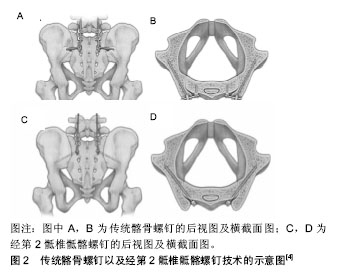
2.1 经第2骶椎骶髂螺钉及其发展历史 脊柱骨盆固定起始于20世纪60年代,可重建腰骶部的稳定性。其发展历史先后经历了Harrington,Luque以及GaLveston技术[6-8],然而这些固定方式存在许多问题,如假关节形成、生物力学强度不足、螺钉松动以及断裂等。直至髂骨螺钉技术的出现,作为Galveston技术的改良方法,髂骨螺钉将髂骨固定强度提高了3倍[9],为脊柱骨盆固定提供了良好的生物力学支持,并逐渐成为目前应用最为广泛的脊柱骨盆固定方法。但传统髂骨螺钉在收到良好治疗效果的同时,也存在如手术切口大、剥离范围广、置入后感染风险增加、螺钉突出导致的疼痛、压疮甚至皮肤破溃等缺点[10]。为了解决这一系列问题,于2007年提出了经第2骶椎骶髂螺钉技术,相对于传统髂骨螺钉置入技术,该技术具有更少的组织剥离,与上位椎体的椎弓根螺钉可直对接,无需对连接棒进行特殊的预弯和使用额外的连接杆,以及进钉点更深、钉头距皮肤表面更远、不影响髂骨取骨等优势[11]。 目前经第2骶椎骶髂螺钉主要应用于涉及到骶骨融合的长节段脊柱固定、严重的腰椎滑脱、L5/S1假关节的补救治疗、纠正神经源性脊柱侧弯患者的骨盆倾斜等疾病的治疗中。国际上也有经第2骶椎骶髂螺钉用于治疗化脓性椎间盘炎以及下腰部结核的报道,且取得了良好的治疗效果[12-15]。 经第2骶椎骶髂螺钉从S1-2后孔之间进钉,贯穿整个骶髂关节,指向髋臼上方[16],见图2。因经第2骶椎骶髂螺钉的置钉路径毗邻上臀动脉、髂内动静脉、坐骨神经、闭孔神经、腰骶丛神经等重要的血管和神经[17]。早期的经第2骶椎骶髂螺钉置入多在O-ARM影像系统的辅助下完成[18],此后不断发展出经皮置入经第2骶椎骶髂螺钉以及机器人辅助置钉等技术[19-22]。目前国内也有首个通过3 D打印个体化模板辅助置入经第2骶椎骶髂螺钉的报道[23]。近年来,国际上外多位学者提倡徒手置入经第2骶椎骶髂螺钉以减少置入中放射暴露对患者及术者的伤害,且有多项徒手置钉以及置入后随访的研究,均取得良好的治疗效果[24-25]。"
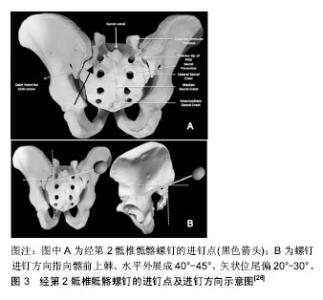
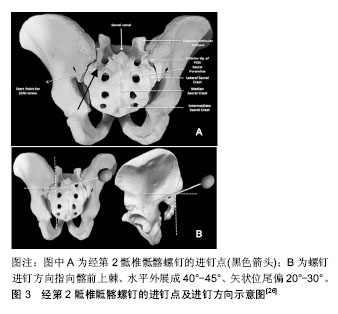
2.2 经第2骶椎骶髂的徒手置入螺钉方法 患者在俯卧位下取后路正中切口,显露至骶骨并暴露S1-2后孔以确定经第2骶椎骶髂螺钉的进钉点,取分别距骶1后孔外缘与下缘1 mm的垂线和水平线的交点作为进钉点,见图3A,并尽可能的与上位的S1螺钉以及其他椎弓根螺钉相对齐,在确定好进钉点后,先以咬骨钳或高速钻钻破进钉点处骶骨皮质,然后使用开路椎以指向髂前上棘、水平外展成40°-45°、矢状位尾偏20°-30°的方向扩宽钉道,见图3B,并穿透骶髂关节(开路锥穿透骶髂关节时,会有明显的落空感),当开路锥进入深度约50 mm时,使用球头探针对钉道的“前”、“后”、“内”、“外”、“底” 5个壁的完整性进行探查无误后依据扩好的钉道置入经第2骶椎骶髂螺钉。当临床上需置入2枚经第2骶椎骶髂螺钉时,可将S1-2后孔间骨质平分后,在2处骨质中心以上述方法分别置入经第2骶椎骶髂螺钉[11,26]。"
2.3 经第2骶椎骶髂螺钉与传统髂骨的生物力学差异 作为传统髂骨螺钉的替代技术,经第2骶椎骶髂螺钉在生物力学强度方面是否接近、甚至超越传统髂骨螺钉,是检验其替代技术成功与否的重要标准。经第2骶椎骶髂螺钉的置钉路径贯穿了整个骶髂关节,螺钉本身穿透了3层皮质骨,按照既往骨科螺钉置入的经验,螺钉较多的穿过皮质骨理论上可以增加螺钉的把持力和生物力学强度。关于经第2骶椎骶髂螺钉最早的生物力学强度试验由O’Brien等[2]于2013年进行,其对置入经第2骶椎骶髂螺钉的尸体标本在不同状态下的应力进行了分析,得出其经第2骶椎骶髂螺钉与传统髂骨螺钉在生物力学强度方面接近,在其研究中也对不同长度的经第2骶椎骶髂螺钉的生物力学性能进行了比较,结论为直径为65,80,90 mm的经第2骶椎骶髂螺钉的生物力学性能接近,但是O’Brien等[2]指出由于螺钉钉头与钉身间的杠杆作用,钉头与钉身指尖颈部的较长的距离会使经第2骶椎骶髂螺钉其断裂风险可能会相应增加。在此之后,Sutterlin等[3-5]的经第2骶椎骶髂螺钉生物力学实验均围绕尸体标本进行,同样与传统髂骨螺钉进行比较,并得出了类似的结果。 2.4 经第2骶椎骶髂螺钉置入后并发症 2.4.1 置入后螺钉松动与断裂 有研究指出骶髂关节为两性关节,其长时间的微动可能加速经第2骶椎骶髂螺钉的松动及断裂[27];但在近些年的研究显示,经第2骶椎骶髂螺钉较髂骨螺钉呈现出较低螺钉松动率。Ilyas等[28]分别对接受髂骨螺钉和经第2骶椎骶髂螺钉固定的成人及儿童患者进行了回顾性分析,在平均22.3个月的随访时间内,经第2骶椎骶髂螺钉组中无一例发生螺钉松动的情况,而同期髂骨螺钉组松动率为18.1%。国内学者谢雁春等[29]进行了类似的研究,同样未在经第2骶椎骶髂螺钉组发现螺钉松动的情况。Smith等[30]在对86例使用经第2骶椎骶髂螺钉固定的患者进行了2年以上的随访,9例发生螺钉松动,松动率为11%。 经第2骶椎骶髂螺钉的断裂发生率也呈现低水平,大多数经第2骶椎骶髂螺钉断裂集中在直径为8 mm及以下的螺钉,断裂位置多在螺钉头与钉身交界的颈部,此外未置入S1螺钉也是经第2骶椎骶髂螺钉断钉的危险因素之一。在Ilyas等[28]的研究中,成人组的22例与儿童组的15例患者中各发生了1例断钉,总体的断钉率为5%,成人组中的1例患者在手术过程中因解剖学变异的原因未置入S1螺钉,且该患者与其他人所使用的经第2骶椎骶髂螺钉直径及长度均为8/80 mm,因此认为该患者发生断钉的主要原因是未置入S1螺钉。儿童组的断钉则被认为是由于患儿使用的经第2骶椎骶髂螺钉直径为6.5 mm,< 8-10 mm的推荐直径[31],且该患儿的复查X射线结果显示,断钉发生于螺钉的颈部。在Smith等[30]的断钉报道中,1例患者在外伤后出现螺钉断裂,发生断裂的螺钉直径为7.5 mm。Jain等[32]对80例接受经第2骶椎骶髂螺钉固定的儿童进行了至少2年(平均3.5年)的随访,共发现9例断钉,所有螺钉的折断部位均位于螺钉颈部,且螺钉直径均≤8 mm,没有发现9或10 mm螺钉断裂的情况。 与上述研究中经第2骶椎骶髂螺钉的低断钉率所不同,Guler等[33]在其早先的报道中提出经第2骶椎骶髂螺钉存在高达35%的螺钉断裂率。其将螺钉断裂的原因归结于以下2点:①经第2骶椎骶髂螺钉固定后螺钉头与螺钉杆之间形成锐角,两者之间存在剪切力;②不同品牌的螺钉本身的质量问题。 针对上述研究中经第2骶椎骶髂螺钉断裂在小直径螺钉上的集中,结合此前O?Brien等[2]的观点总结为:①不同直径的经第2骶椎骶髂螺钉在生物力学强度上没有明显差异,较长的经第2骶椎骶髂螺钉反而由于杠杆作用使得断裂发生的风险增加,作者得出在手术安全允许的前期下尽量使用直径较大、较短的经第2骶椎骶髂螺钉,这可能有助于预防经第2骶椎骶髂螺钉的断裂;②经第2骶椎骶髂螺钉断裂的位置多集中在螺钉颈部,因此建议螺钉厂家有意识的对该部位进行加固,也是预防经第2骶椎骶髂螺钉断裂的一种新思路;③对于因解剖学变异或S1椎体破坏严重无法置入S1螺钉时,经第2骶椎骶髂螺钉的断裂率有增加的风险,这点应引起临床医生的足够重视,在手术中应对局部进行加固,以降低经第2骶椎骶髂螺钉发生断裂的风险。 2.4.2 骶髂关节疼痛及关节退变 由于经第2骶椎骶髂螺钉的置钉路径贯穿了整个骶髂关节,有研究认为在经第2骶椎骶髂螺钉置入过程中,有60%螺钉会对骶髂关节面造成侵犯[34]。因此经第2骶椎骶髂螺钉的置入是否会引起骶髂关节疼痛及关节退变,自然成为临床医生在选择经第2骶椎骶髂螺钉固定时所关注的重点。目前国内外文献中对于骶髂关节退变的诊断及评估方法主要为置入后影像学观察以及与骶髂关节相关的查体实验。 Mazur等[35]对13例接受经第2骶椎骶髂螺钉固定的患者,分别在置入前及置入后至少12个月时进行了CT扫描,并对骶髂关节的退变情况进行了观察。其对于骶髂关节退变的影像学表现定义为:①整个关节区域的硬化、关节面变性(髂骨关节 > 5 mm,骶骨关节面 > 3 mm)、糜烂;②超出骶髂关节外的骨赘形成;③关节间隙狭窄 < 2 mm;④关节内出现破碎的骨片或者软骨下囊肿。Mazur等[35]并未从影像学角度发现经第2骶椎骶髂螺钉固定后会导致骶髂关节退变的证据。 Elder等[36]与刘臻等[37]则通过查体试验的方式对经第2骶椎骶髂螺钉置入后患者的骶髂关节疼痛及退变情况进行评价。在Elder等[36]的研究中骶髂关节疼痛的检测包括:①骶骨按压试验(sacral compression test);②大腿推力试验(thigh thrust test);③“4”字试验(Patrick’s test),在这3项查体试验中有3个以上阳性结果的患者才可被认为存在骶髂关节疼痛。根据Elder等[36]对25例髂骨螺钉固定和68例经第2骶椎骶髂螺钉固定的患者至少1年的随访显示,髂骨螺钉组中有3例出现骶髂关节疼痛(12%),经第2骶椎骶髂螺钉组为6例(9%)。2组骶髂关节疼痛的发生率相似(P=0.70)。刘臻等[37]对骶髂关节退变情况的评价则采用5项检测:①Gillet 实验;②站立屈曲实验;③骨盆分离实验;④Gaenslen实验;⑤骶骨按压实验。在5项实验中3项阳性的患者被认为存在骶髂关节功能障碍。刘臻等[37]对2组22例分别使用髂骨螺钉及经第2骶椎骶髂螺钉治疗后出现退变性脊柱后突出的成年患者进行了置入后随访,其中经第2骶椎骶髂螺钉组随访时间为(26.8±1.7)个月,髂骨螺钉组随访时间为(35.9±11.5)个月,结果髂骨螺钉及经第2骶椎骶髂螺钉组均未发现有骶髂关节疼痛或退变的证据。 综上,经第2骶椎骶髂螺钉的置钉路径虽然贯穿整个骶髂关节,但并未因此增加患者骶髂关节疼痛及退化的风险。相反,在涉及到L5/S1融合的长节段脊柱固定中,由于L5/S1的融合,骶髂关节的生物力学负担可能相应增加,从而加重了骶髂关节退化并引起患者出现骶髂关节疼痛。而使用经第2骶椎骶髂螺钉对骶髂关节进行稳定,可能有助于减缓少这些并发症的发生。此前国外的解剖学研究结果显示,骶骨在髂骨上的投影远大于骶髂关节的关节软骨面[38],因此经第2骶椎骶髂螺钉有足够的行走空间来避免损伤骶髂关节软骨,加上精确的置入前影像学评估、螺钉路径规划及置入中O-ARM影像系统的使用,可以在经第2骶椎骶髂螺钉置入过程中尽可能的保证骶髂关节的完整性,从而减少骶髂关节相关并发症。 2.4.3 切口并发症 传统髂骨螺钉的一大弊端在于手术切口较大,对周围组织的剥离较多,患者置入后感染以及切口愈合不良甚至裂开的风险较高。而经第2骶椎骶髂螺钉技术具有的组织剥离更少、与上位椎体的椎弓根螺钉可直对接,无需对连接棒进行特殊的预弯以及使用额外的连接杆,手术时间相对缩短等优势,理论上可以减少置入后切口并发症发生率,且既往研究的结果也证实了这一观点[36,39-40],经第2骶椎骶髂螺钉较传统髂骨螺钉表现出较低的置入后感染和切口裂开率,且在迟发性感染方面更加明显。 在Elder等[36]的研究中,25例接受髂骨螺钉固定的患者中有11例出现了切口感染(44%),而68例接受经第2骶椎骶髂螺钉固定的患者中切口感染仅有1例(2%),两者差异有显著性意义(P=0.001),髂骨螺钉与经第2骶椎骶髂螺钉的切口裂开率分别为36%和2%,差异也有显著性意义(P=0.001)。Ishida等[39]在对17例接受髂骨螺钉和46例经第2骶椎骶髂螺钉固定患者的随访研究中也得到了类似的结果,传统髂骨螺钉与经第2骶椎骶髂螺钉的感染率分别为24%和2%,切口裂开率分别为18%和2%。Montero等[40]观察31例接受经第2骶椎骶髂螺钉固定的患儿后得出经第2骶椎骶髂螺钉的感染率仅为7%。Ilyas等[28]同样对这2种固定方式螺钉置入后发生急性、迟发性感染以及切口开裂问题进行了研究,在汇总了成人与儿童的数据后指出,与传统髂骨螺钉相比,使用经第2骶椎骶髂螺钉固定可使患者的急性感染和迟发感染率明显降低,其绝对危险度分别降低为13%和11%。国内对于经第2骶椎骶髂螺钉的切口并发症的研究相对较少,在谢雁春等[29]的研究中,经第2骶椎骶髂螺钉较髂骨螺钉同样保持低感染率(4.5% vs. 23.3%)和切口裂开率(9.1% vs. 16.3%),但两者差异无显著性意义。 内置物置入后感染是长久以来困扰骨科医生的一大难题,也是临床上非计划再手术的重要原因,其增加了患者的痛苦和经济损失。传统髂骨螺钉由于其较大的手术切口和较多组织剥离,导致置入后感染、切口裂开等切口并发症的发生率相对较高,减少这些并发症的是经第2骶椎骶髂螺钉的设计初衷之一。上述研究中经第2骶椎骶髂螺钉较传统髂骨螺钉所表现出的低感染率和低切口裂开率,可以说很好的达到了这一目的,并且对于患有营养不良、糖尿病、肿瘤以及各种原因所导致的免疫力低下时,置入后易发生切口并发症的高危人群来说,其受益可能更多。 2.4.4 症状性螺钉突出 传统髂骨螺钉另一项比较明显的并发症为螺钉突出所引起的疼痛及钉头上方的局部压疮甚至皮肤溃破等,上述情况被称为症状性螺钉突出[27]。症状性螺钉突出成为困扰髂骨螺钉最明显的置入后并发症,在Tsuchiya等[41]对传统髂骨螺钉固定患者的随访中,有23例患者因无法忍受螺钉突出所带来的痛苦而选择二次手术将螺钉取出。此外在O?Shaughnessy 等[42]的研究中78%的存在症状性螺钉突出的患者表示在取出了螺钉后疼痛症状得到了缓解。 在Ilyas等[28]的研究中,68例髂骨螺钉固定的成人患者有13例出现了迟发性的臀肌疼痛,出现疼痛的平均时间为11.8个月;而25例成人经第2骶椎骶髂螺钉固定患者中仅有2例出现迟发性臀肌疼痛,且出现疼痛的平均时间为18个月,明显晚于髂骨螺钉组;在其儿童组随访中没有发现经第2骶椎骶髂螺钉导致迟发性臀肌疼痛发现的情况。综合成人和儿童的随访数据,指出相较于传统髂骨螺钉,经第2骶椎骶髂螺钉的使用使得迟发型臀肌疼痛的绝对危险度下降了19%。在Elder等[36]的研究中经第2骶椎骶髂螺钉导致的症状性螺钉突出率为0%。尽管同研究中所有髂骨螺钉固定患者在手术过程中均使用咬骨钳在髂骨上咬除一部分骨质,为髂骨螺钉钉头预留了空间,尽可能的减少螺钉突出,但髂骨螺钉组症状性螺钉突出的发生率仍然高达11%。 Ishida等[27]则在对接受髂骨螺钉和经第2骶椎骶髂螺钉固定的患者进行了CT检查,提出了螺钉头距皮肤的最小距离的概念并指出,经第2骶椎骶髂螺钉的平均螺钉头距皮肤的最小距离为41.3 mm,髂骨螺钉则为 32.8 mm,而螺钉头距皮肤的最小距离< 23 mm被定义为螺钉突出,Ishida等[27]使用这一指标对症状性螺钉突出进行的预测和诊断。根据Ishida等[27]的研究结果,螺钉头距皮肤的最小距离< 23 mm是诊断螺钉突出的最强预测因子,其敏感性为100%,特异性为94.1%,阳性预测值及阴性预测值分别为47.6%和100%,可以很好的诊断和预测症状性螺钉突出。 综合上述研究,尽管接受经第2骶椎骶髂螺钉固定的患者在置入后仍然存在症状性螺钉突出的情况,但其发生率较传统髂骨螺钉明显较低,疼痛出现的时间也相对较晚。换言之,经第2骶椎骶髂螺钉明显降低了症状性螺钉突出的发生率。这很大程度上可能是因为经第2骶椎骶髂螺钉置入点的深度较髂骨螺钉更深、钉头距皮肤的距离更远。有研究指出 经第2骶椎骶髂螺钉的进钉点深度至少深15 mm[43],并且与传统髂骨螺钉相比,经第2骶椎骶髂置钉过程中对于局部肌肉及组织的剥离也更少,经第2骶椎骶髂螺钉上方有更多的组织给予缓冲和保护,从而减少症状性螺钉突出的发生率。通过对患者CT的观察及螺钉头距皮肤的最小距离的测量,可以更早的预测和诊断症状性螺钉突出。 2.4.5 交界性后凸及假关节形成 有研究指出在长节段脊柱固定后假关节的发生率为8%-42%,尤其在远端仅固定骶骨时假关节的发生率更高达24%[19]。既往研究已证实远端固定会对交界性后凸/交界性失败产生影响。Yagi等[44]对76例患者进行的回顾性研究发现骶骨的融合与交界性后凸的发生显著相关。脊柱骨盆联合固定理论上可以增强局部的稳定性,减少单独使用S1螺钉进行远端固定所带来的并发症。然而不同的骨盆固定方式是否也会对假关节及交界性后凸的发生产生影响? Elder等[36]在对25例髂骨螺钉固定和68例经第2骶椎骶髂螺钉固定的患者至少随访1年后发现,髂骨螺钉组中假关节的发生率为8%,经第2骶椎骶髂螺钉组为5.9%,2组差异无显著性意义(P=0.66)。该研究中2种固定方式的交界性后凸发生率也很相近,分别为28%和25%,差异无显著性意义(P=0.79)。Ishida等[39]在对接受2种固定方式的患者进行了平均21.1个月随访得出了类似的结果,髂骨螺钉与经第2骶椎骶髂螺钉固定后假关节的发生率为分别为11.8%和4.3%,差异无显著性意义(P=0.18),交界性后凸的发生率为35.3%和32.6%(P > 0.99),该研究显示虽然2组的交界性后凸发生率接近,但经第2骶椎骶髂螺钉在因交界性失败所导致的再手术时间明显要晚于传统髂骨螺钉。 上述研究还指出假关节多发生于L5/S1关节,这与既往研究结果一致。Elder等[36]发现远端固定后螺钉松动与L5/S1假关节的形成并没有存在必然的联系,而经第2骶椎骶髂螺钉组的2名患者虽然存在明显的假关节症状,但患者并没有出现明显的螺钉松动迹象,因此认为脊柱骨盆固定后L5/S1假关节形成与远端螺钉松动关系尚需进一步研究。 尽管骨盆固定方式对假关节形成及交界性后凸/交界性失败产生影响的确切机制尚不清楚,但可以肯定的是经第2骶椎骶髂螺钉与其他骨盆植入物固定方式相比并没有明显增加假关节及交界性后凸/交界性失败发生率。相反,在因交界性后凸/交界性失败所导致的再手术时间上,经第2骶椎骶髂螺钉较传统髂骨螺钉反而表现的更晚。关于经第2骶椎骶髂螺钉固定后交界性后凸/交界性失败的预防,国外学者Mummaneni等[45]提出经皮微创置入经第2骶椎骶髂螺钉减少了对脊柱后部的破坏,可以降低交界性后凸的发生率。此外,国际上有很多研究报道了经第2骶椎骶髂螺钉经皮置入取得的良好治疗效果[19-20]。"

| [1] Lin JD, Tan LA, Wei C, et al. The posterior superior iliac spine and sacral laminar slope: key anatomical landmarks for freehand S2-alar-iliac screw placement. J Neurosurg Spine. 2018;29(4): 429-434. [2] O’Brien JR, Yu W, Kaufman BE, et al. Biomechanical evaluation of S2 alar-iliac screws: effect of length and quad-cortical purchase as compared with iliac fixation. Spine (Phila Pa 1976). 2013;38(20): E1250-1255. [3] Sutterlin CE 3rd, Field A, Ferrara LA, et al. Range of motion, sacral screw and rod strain in long posterior spinal constructs: a biomechanical comparison between S2 alar iliac screws with traditional fixation strategies. J Spine Surg. 2016;2(4):266-276. [4] Burns CB, Dua K, Trasolini NA, et al. Biomechanical Comparison of Spinopelvic Fixation Constructs: Iliac Screw Versus S2-Alar-Iliac Screw. Spine Deform. 2016;4(1):10-15. [5] Hoernschemeyer DG, Pashuck TD, Pfeiffer FM. Analysis of the s2 alar-iliac screw as compared with the traditional iliac screw: does it increase stability with sacroiliac fixation of the spine? Spine J. 2017; 17(6):875-879. [6] Jain A, Hassanzadeh H, Strike SA, et al. Pelvic Fixation in Adult and Pediatric Spine Surgery: Historical Perspective, Indications, and Techniques: AAOS Exhibit Selection. J Bone Joint Surg Am. 2015; 97(18):1521-1528. [7] 张楠威,于滨生.经S2骶髂螺钉技术在脊柱骨盆稳定性重建中应用的研究进展[J].中国修复重建外科杂志,2018,32(6):764-768.[8] Moshirfar A, Rand FF, Sponseller PD, et al. Pelvic fixation in spine surgery. Historical overview, indications, biomechanical relevance, and current techniques. J Bone Joint Surg Am. 2005;87 Suppl 2: 89-106. [9] Schwend RM, Sluyters R, Najdzionek J. The pylon concept of pelvic anchorage for spinal instrumentation in the human cadaver. Spine (Phila Pa 1976). 2003;28(6):542-547. [10] 项泱,谭军,任甜甜,等.髂骨螺钉置入技术研究进展[J].现代实用医学, 2016, 28(10):1261-1264.[11] Lombardi JM, Shillingford JN, Lenke LG, et al. Sacropelvic Fixation: When, Why, How? Neurosurg Clin N Am. 2018;29(3): 389-397. [12] 刘臻,李劼,赵志慧,等.重度神经肌源性脊柱侧凸伴骨盆倾斜三种内固定模式的比较研究[J].中华骨科杂志,2018,38(4):193-203.[13] Mazur MD, Ravindra VM, Dailey AT, et al. Rigid Posterior Lumbopelvic Fixation without Formal Debridement for Pyogenic Vertebral Diskitis and Osteomyelitis Involving the Lumbosacral Junction: Technical Report. Front Surg. 2015;2:47. [14] 王孝宾,王冰,李晶,等.经骶2髂骨螺钉内固定在腰骶段结核稳定性重建中的应用[J].中国脊柱脊髓杂志,2017,27(5):392-398.[15] 谢雁春,项良碧,刘军,等.经皮骶2髂骨三皮质螺钉治疗老年无神经症状下腰椎椎间盘炎的近期疗效分析[J].介入放射学杂志,2018,27(1): 53-57.[16] Yamada K, Higashi T, Kaneko K, et al. Optimal trajectory and insertion accuracy of sacral alar iliac screws. Acta Orthop Traumatol Turc. 2017; 51(4):313-318. [17] Abdul-Jabbar A, Yilmaz E, Iwanaga J, et al. Neurovascular Relationships of S2AI Screw Placement: Anatomic Study. World Neurosurg. 2018;116:e108-e112. [18] Ray WZ, Ravindra VM, Schmidt MH, et al. Stereotactic navigation with the O-arm for placement of S-2 alar iliac screws in pelvic lumbar fixation. J Neurosurg Spine. 2013;18(5):490-495. [19] Martin CT, Witham TF, Kebaish KM. Sacropelvic fixation: two case reports of a new percutaneous technique. Spine (Phila Pa 1976). 2011;36(9):E618-621. [20] Funao H, Kebaish KM, Isogai N, et al. Utilization of a Technique of Percutaneous S2 Alar-Iliac Fixation in Immunocompromised Patients with Spondylodiscitis. World Neurosurg. 2017;97:757. e11-757. e18. [21] Hu X, Lieberman IH. Robotic-guided sacro-pelvic fixation using S2 alar-iliac screws: feasibility and accuracy. Eur Spine J. 2017; 26(3): 720-725. [22] Laratta JL, Shillingford JN, Lombardi JM, et al. Accuracy of S2 Alar-Iliac Screw Placement Under Robotic Guidance. Spine Deform. 2018;6(2):130-136. [23] 马宇龙,赵永辉,罗浩天,等.个体化导航模板辅助第2骶椎髂骨螺钉置钉的临床应用[J].中华创伤骨科杂志, 2018,20(4):329-333.[24] Park YS, Hyun SJ, Park JH, et al. Radiographic and Clinical Results of Freehand S2 Alar-Iliac Screw Placement for Spinopelvic Fixation: An Analysis of 45 Consecutive Screws. Clin Spine Surg. 2017;30(7): E877-E882. [25] Fang T, Russo GS, Schroeder GD, et al. The Accurate Free-hand Placement of S2 Alar Iliac (S2AI) Screw. Clin Spine Surg. 2018 Mar 16. doi:10.1097/BSD. 0000000000000623. [Epub ahead of print][26] Shillingford JN, Laratta JL, Tan LA, et al. The Free-Hand Technique for S2-Alar-Iliac Screw Placement: A Safe and Effective Method for Sacropelvic Fixation in Adult Spinal Deformity. J Bone Joint Surg Am. 2018;100(4):334-342. [27] Ishida W, Elder BD, Holmes C, et al. S2-Alar-Iliac Screws are Associated with Lower Rate of Symptomatic Screw Prominence than Iliac Screws: Radiographic Analysis of Minimal Distance from Screw Head to Skin. World Neurosurg. 2016;93:253-260.[28] Ilyas H, Place H, Puryear A. A Comparison of Early Clinical and Radiographic Complications of Iliac Screw Fixation Versus S2 Alar Iliac (S2AI) Fixation in the Adult and Pediatric Populations. J Spinal Disord Tech. 2015;28(4):E199-205. [29] 谢雁春,王丹妮,吴骏,等.骶2髂骨三皮质螺钉和髂骨螺钉的临床并发症比较[J].局解手术学杂志,2017,26(6):415-418.[30] Smith EJ, Kyhos J, Dolitsky R, et al. S2 Alar Iliac Fixation in Long Segment Constructs, a Two- to Five-Year Follow-up. Spine Deform. 2018;6(1):72-78. [31] Kebaish KM. Sacropelvic fixation: techniques and complications. Spine (Phila Pa 1976). 2010;35(25):2245-2251. [32] Jain A, Kebaish KM, Sponseller PD. Sacral-Alar-Iliac Fixation in Pediatric Deformity: Radiographic Outcomes and Complications. Spine Deform. 2016;4(3):225-229. [33] Guler UO, Cetin E, Yaman O, et al. Sacropelvic fixation in adult spinal deformity (ASD); a very high rate of mechanical failure. Eur Spine J. 2015;24(5):1085-1091. [34] O'Brien JR, Yu WD, Bhatnagar R, et al. An anatomic study of the S2 iliac technique for lumbopelvic screw placement. Spine (Phila Pa 1976). 2009;34(12):E439-442. [35] Mazur MD, Mahan MA, Shah LM, et al. Fate of S2-Alar-Iliac Screws After 12-Month Minimum Radiographic Follow-up: Preliminary Results. Neurosurgery. 2017;80(1):67-72. [36] Elder BD, Ishida W, Lo SL, et al. Use of S2-Alar-iliac Screws Associated With Less Complications Than Iliac Screws in Adult Lumbosacropelvic Fixation. Spine (Phila Pa 1976). 2017;42(3): E142-E149. [37] 刘臻,曾昌淳,赵志慧,等.经第2骶椎骶髂螺钉与髂骨螺钉技术治疗成人退变性脊柱侧后凸的矫形疗效比较[J].中华外科杂志, 2018,56(2): 139-146.[38] Xu R, Ebraheim NA, Douglas K, et al. The projection of the lateral sacral mass on the outer table of the posterior ilium. Spine (Phila Pa 1976). 1996;21(7):790-794; discussion 795. [39] Ishida W, Elder BD, Holmes C, et al. Comparison Between S2-Alar-Iliac Screw Fixation and Iliac Screw Fixation in Adult Deformity Surgery: Reoperation Rates and Spinopelvic Parameters. Global Spine J. 2017;7(7):672-680. [40] Montero CS, Meneses DA, Alvarado F, et al. Outcomes and complications of S2 alar iliac fixation technique in patients with neuromuscular scoliosis: experience in a third level pediatric hospital. J Spine Surg. 2017;3(4):519-524. [41] Tsuchiya K, Bridwell KH, Kuklo TR, et al. Minimum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine (Phila Pa 1976). 2006;31(3):303-308. [42] O?Shaughnessy BA, Lenke LG, Bridwell KH, et al. Should symptomatic iliac screws be electively removed in adult spinal deformity patients fused to the sacrum? Spine (Phila Pa 1976). 2012;37(13):1175-1181. [43] Chang TL, Sponseller PD, Kebaish KM, et al. Low profile pelvic fixation: anatomic parameters for sacral alar-iliac fixation versus traditional iliac fixation. Spine (Phila Pa 1976). 2009; 34(5):436-440. [44] Yagi M, Akilah KB, Boachie-Adjei O. Incidence, risk factors and classification of proximal junctional kyphosis: surgical outcomes review of adult idiopathic scoliosis. Spine (Phila Pa 1976). 2011;36(1):E60-68. [45] Mummaneni PV, Park P, Fu KM, et al. Does Minimally Invasive Percutaneous Posterior Instrumentation Reduce Risk of Proximal Junctional Kyphosis in Adult Spinal Deformity Surgery? A Propensity-Matched Cohort Analysis. Neurosurgery. 2016; 78(1):101-108. [46] Mazur MD, Ravindra VM, Schmidt MH, et al. Unplanned reoperation after lumbopelvic fixation with S-2 alar-iliac screws or iliac bolts. J Neurosurg Spine. 2015;23(1):67-76. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [3] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [4] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [5] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [6] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [7] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [8] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [9] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [10] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [11] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [12] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| [13] | Mo Jianling, He Shaoru, Feng Bowen, Jian Minqiao, Zhang Xiaohui, Liu Caisheng, Liang Yijing, Liu Yumei, Chen Liang, Zhou Haiyu, Liu Yanhui. Forming prevascularized cell sheets and the expression of angiogenesis-related factors [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3479-3486. |
| [14] | Liu Chang, Li Datong, Liu Yuan, Kong Lingbo, Guo Rui, Yang Lixue, Hao Dingjun, He Baorong. Poor efficacy after vertebral augmentation surgery of acute symptomatic thoracolumbar osteoporotic compression fracture: relationship with bone cement, bone mineral density, and adjacent fractures [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3510-3516. |
| [15] | Liu Liyong, Zhou Lei. Research and development status and development trend of hydrogel in tissue engineering based on patent information [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3527-3533. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||