Chinese Journal of Tissue Engineering Research ›› 2018, Vol. 22 ›› Issue (23): 3703-3709.doi: 10.3969/j.issn.2095-4344.0244
Previous Articles Next Articles
Effects of aspirin discontinuation on the risk of cardiovascular and cerebrovascular events and lower limb venousthrombosis and bleeding in the perioperative period of cervical surgery
Zhang Cheng-gui1, Wang Guo-dong1, Sun Jian-min1, Liu Le2
- 1Department of Spine Surgery, Shandong Provincial Hospital, Shandong University, Jinan 250013, Shandong Province, China; 2Department of Orthopedics, the 148 Hospital of Chinese PLA, Zibo 255300, Shandong Province, China
-
Online:2018-08-18Published:2018-08-18 -
Contact:Sun Jian-min, M.D., Chief physician, Department of Spine Surgery, Shandong Provincial Hospital, Shandong University, Jinan 250013, Shandong Province, China -
About author:Zhang Cheng-gui, Master candidate, Department of Spine Surgery, Shandong Provincial Hospital, Shandong University, Jinan 250013, Shandong Province, China -
Supported by:the Shandong Province Science and Technology Development Project, No. 2012GSF11815
CLC Number:
Cite this article
Zhang Cheng-gui, Wang Guo-dong, Sun Jian-min, Liu Le. Effects of aspirin discontinuation on the risk of cardiovascular and cerebrovascular events and lower limb venousthrombosis and bleeding in the perioperative period of cervical surgery[J]. Chinese Journal of Tissue Engineering Research, 2018, 22(23): 3703-3709.
share this article
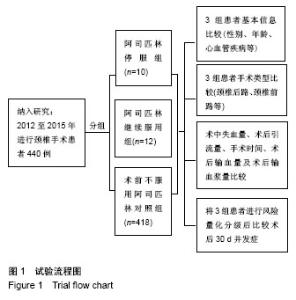
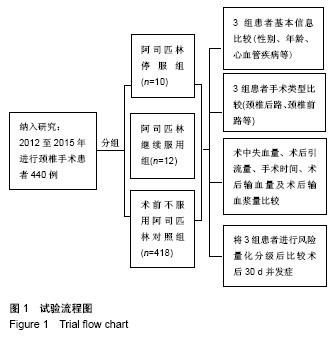
2.1 参与者数量分析 纳入研究的440例患者均进入结果数据分析。 2.2 试验流程图 见图1。"

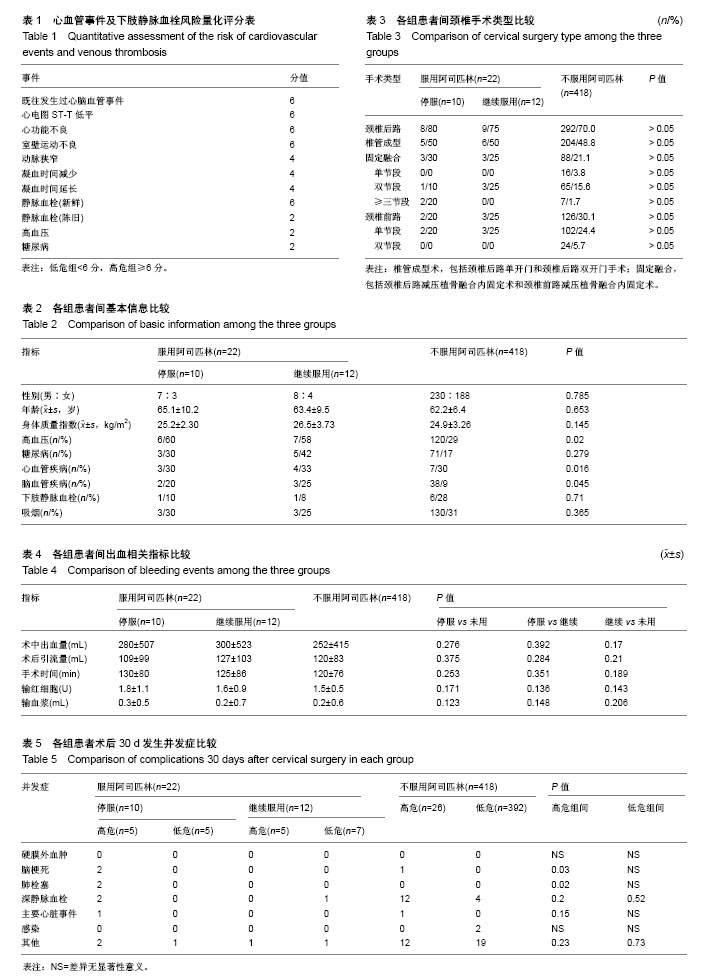
2.3 各组患者临床资料比较 2.3.1 患者基本状况比较 见表2。阿司匹林停服组、继续服用组、未用组3组平均年龄分别为(65.1±10.2)岁,(63.4±9.5)岁,(62.2±6.4)岁,3组之间差异无显著性意义(P=0.653);3组间高血压病的比例分别为60%(6/10),58%(7/12),29%(120/418),3组之间差异有显著性意义(P=0.020);3组间心血管疾病的比例分别为30%(3/10),33%(4/12),7%(30/418),3组之间差异有显著性意义(P=0.016);3组间脑血管疾病的比例分别为20%(2/10),25%(3/12),9%(38/418),3组之间差异有显著性意义(P=0.045);3组间糖尿病的比例分别为30%(3/10),42%(5/12),17%(71/418),3组之间差异无显著性意义(P=0.279);此外3组之间在性别(P=0.785)、身体质量指数(P=0.145)、下肢静脉血栓(P=0.71)、吸烟(P=0.365)等方面差异也无显著性意义。 2.3.2 患者手术方式类型比较 见表3。3组患者行颈椎手术治疗的方式包括颈椎后路和颈椎前路,后路术式分为椎管成形术(颈椎后路单开门减压内固定术或颈椎后路双开门减压内固定术)、颈椎后路减压植骨融合内固定术(单节段、双节段、三节段),前路术式为颈椎前路减压植骨融合内固定术(单节段、双节段)。3组患者在手术方式上差异无显著性意义,3组患者采用的手术方式情况基本一致。 2.3.3 患者出血事件比较 见表4。阿司匹林停服组、继续服用组、未用组3组患者术中出血量分别为(280±507),(300±523)和(251±41) mL,3组之间比较差异无显著性意义(P > 0.05);3组患者引流量分别为(109±99),(127±103)和(120±83) mL,3组之间比较差异无显著性意义(P > 0.05);3组患者手术时间分别为(130±80),(125±85)和(120±76) min,3组之间比较差异无显著性意义(P > 0.05);3组患者术后输红细胞分别为(1.8±1.1),(1.6±0.9)和(1.5±0.5) U,3组之间比较差异无显著性意义(P > 0.05);3组患者术后输血浆量分别为(0.3±0.5),(0.2±0.7)和(0.2±0.6) U,3组之间比较差异无显著性意义(P > 0.05);3组患者在术中出血量、术后引流量及术后输红细胞或血浆量等方面没有显著差异。 2.3.4 术后30 d发生的并发症比较 见表5。将3组患者根据心血管事件及下肢静脉血栓风险量化评分表分为高危组和低危组,停服阿司匹林组(10例)中高危组5例、低危组5例,继续服用阿司匹林组(12例)中高危组5例、低危组7例,不服用阿司匹林组(418例)中高危组26例、低危组392例。 停服阿司匹林高危组中有2例患者发生脑梗死,均为老年男性患者,且均患有冠心病,1例先后置入2个心脏支架,另1例先后置入3个心脏支架,均在手术前7 d停用阿司匹林,仔细询问病史既往并没有脑梗死发作征象,术后颅脑CT示多发梗死灶形成,脑梗死怀疑为停药后引起心脏支架血栓形成脱落后所致。既往1例不服用阿司匹林高危组中有1例患者发生脑梗死,患者术后出现不明原因言语不清、双上肢肌力降至0级、双下肢肌力降至0级,行颅脑CT示多发脑缺血、脑梗死、脑萎缩。均转至神经内科进行系统治疗。 停服阿司匹林高危组中有2例患者发生肺栓塞,均为老年女性,1例既往有高血压病、冠心病,术前7 d停用阿司匹林,术后凌晨3点疼痛难忍,发现其右小腿肿胀,急查凝血五项示:D-二聚体4.82 mg/L,给予速碧林4 100 U皮下注射,于凌晨5:30分突然出现意识丧失,呼之不应,心电监测示室颤,积极抢救1 h无效后死亡。分析死亡原因为下肢深静脉血栓脱落导致肺栓塞后引起呼吸骤停。另1例患者为2个心脏支架置入者,考虑为停药后引起心脏支架血栓形成脱落后所致。 停服阿司匹林高危组较未停服阿司匹林组及不用阿司匹林组更容易引起脑梗死(P=0.03)、肺栓塞(P=0.02)的发生,而在发生硬膜外血肿、深静脉血栓及感染方面无明显差异。 "
| [1] Gerstein NS, Schulman PM, Gerstein WH, et al. Should more patients continue aspirin therapy perioperatively?: clinical impact of aspirin withdrawal syndrome. Ann Surg. 2012; 255(5):811-819.[2] Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324(7329):71-86.[3] Park HJ, Kwon KY, Woo JH. Comparison of blood loss according to use of aspirin in lumbar fusion patients. Eur Spine J. 2014;23(8):1777-1782.[4] Ferrari E, Benhamou M, Cerboni P, et al. Coronary syndromes following aspirin withdrawal: a special risk for late stent thrombosis. J Am Coll Cardiol. 2005;45(3):456-459.[5] Oscarsson A, Gupta A, Fredrikson M, et al. To continue or discontinue aspirin in the perioperative period: a randomized, controlled clinical trial. Br J Anaesth. 2010; 104(3):305-312.[6] Meade T, Wilkes H, Kelleher C, et al. Thrombosis prevention trial: randomised trial of low-intensity oral anticoagulation with warfarin and low-dose aspirin in the primary prevention of ischaemic heart disease in men at increased risk. The Medical Research Council's General Practice Research Framework. Lancet. 1998;351(9098): 233-241.[7] Godwin J. Collaborative overview of randomised trials of antiplatelet therapy--I: Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. Antiplatelet Trialists' Collaboration. BMJ. 1994;308(6921):81-106.[8] Hansson L, Zanchetti A, Carruthers SG, et al. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet. 1998;351(9118):1755-1762.[9] De Gaetano G, Collaborative Group of the Primary Prevention Project. Low-dose aspirin and vitamin E in people at cardiovascular risk: a randomised trial in general practice. Collaborative Group of the Primary Prevention Project. Lancet. 2001;357(9250):89-95.[10] Antithrombotic Trialists' (ATT) Collaboration, Baigent C, Blackwell L, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009;373(9678):1849-1860. [11] Berger JS, Roncaglioni MC, Avanzini F, et al. Aspirin for the primary prevention of cardiovascular events in women and men: a sex-specific meta-analysis of randomized controlled trials. JAMA. 2006;295(3):306-313.[12] Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005;352(13):1293-1304.[13] Hayden M, Pignone M, Phillips C, et al. Aspirin for the primary prevention of cardiovascular events: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;136(2):161-172.[14] Steering Committee of the Physicians' Health Study Research Group. Final report on the aspirin component of the ongoing Physicians' Health Study. N Engl J Med. 1989;321(3): 129-135.[15] Peto R, Gray R, Collins R, et al. Randomised trial of prophylactic daily aspirin in British male doctors. Br Med J (Clin Res Ed). 1988;296(6618):313-316.[16] Madan GA, Madan SG, Madan G, et al. Minor oral surgery without stopping daily low-dose aspirin therapy: a study of 51 patients. J Oral Maxillofac Surg. 2005;63(9):1262-1265.[17] Ferraris VA, Ferraris SP, Joseph O, et al. Aspirin and postoperative bleeding after coronary artery bypass grafting. Ann Surg. 2002;235(6):820-827.[18] Gibbs NM, Weightman WM, Thackray NM, et al. The effects of recent aspirin ingestion on platelet function in cardiac surgical patients. J Cardiothorac Vasc Anesth. 2001;15(1): 55-59.[19] Ferraris VA, Ferraris SP, Lough FC, et al. Preoperative aspirin ingestion increases operative blood loss after coronary artery bypass grafting. Ann Thorac Surg. 1988;45(1):71-74.[20] Assia EI, Raskin T, Kaiserman I, et al. Effect of aspirin intake on bleeding during cataract surgery. J Cataract Refract Surg. 1998;24(9):1243-1246.[21] Merriman E, Bell W, Long DM. Surgical postoperative bleeding associated with aspirin ingestion. Report of two cases. J Neurosurg. 1979;50(5):682-684.[22] Soleman J, Baumgarten P, Perrig WN, et al. Non-instrumented extradural lumbar spine surgery under low-dose acetylsalicylic acid: a comparative risk analysis study. Eur Spine J. 2016;25(3):732-739.[23] Mantz J, Samama CM, Tubach F, et al. Impact of preoperative maintenance or interruption of aspirin on thrombotic and bleeding events after elective non-cardiac surgery: the multicentre, randomized, blinded, placebo-controlled, STRATAGEM trial. Br J Anaesth. 2011;107(6):899-910.[24] Burdess A, Nimmo AF, Garden OJ, et al. Randomized controlled trial of dual antiplatelet therapy in patients undergoing surgery for critical limb ischemia. Ann Surg. 2010;252(1):37-42.[25] Giannarini G, Mogorovich A, Valent F, et al. Continuing or discontinuing low-dose aspirin before transrectal prostate biopsy: results of a prospective randomized trial. Urology. 2007;70(3):501-505.[26] Herget EJ, Saliken JC, Donnelly BJ, et al. Transrectal ultrasound-guided biopsy of the prostate: relation between ASA use and bleeding complications. Can Assoc Radiol J. 1999;50(3):173-176.[27] Maan Z, Cutting CW, Patel U, et al. Morbidity of transrectal ultrasonography-guided prostate biopsies in patients after the continued use of low-dose aspirin. BJU Int. 2003;91(9): 798-800.[28] Halliwell OT, Yadegafar G, Lane C, et al. Transrectal ultrasound-guided biopsy of the prostate: aspirin increases the incidence of minor bleeding complications. Clin Radiol. 2008;63(5):557-561.[29] Ferraris VA, Swanson E. Aspirin usage and perioperative blood loss in patients undergoing unexpected operations. Surg Gynecol Obstet. 1983;156(4):439-442.[30] Grubitzsch H, Wollert HG, Eckel L. Emergency coronary artery bypass grafting: does excessive preoperative anticoagulation increase bleeding complications and transfusion requirements. Cardiovasc Surg. 2001;9(5): 510-516.[31] Sun JC, Crowther MA, Warkentin TE, et al. Should aspirin be discontinued before coronary artery bypass surgery. Circulation. 2005;112(7):e85-90.[32] Srinivasan AK, Grayson AD, Pullan DM, et al. Effect of preoperative aspirin use in off-pump coronary artery bypass operations. Ann Thorac Surg. 2003;76(1):41-45.[33] Tuman KJ, McCarthy RJ, O'Connor CJ, et al. Aspirin does not increase allogeneic blood transfusion in reoperative coronary artery surgery. Anesth Analg. 1996;83(6):1178-1184.[34] Park JH, Ahn Y, Choi BS, et al. Antithrombotic effects of aspirin on 1- or 2-level lumbar spinal fusion surgery: a comparison between 2 groups discontinuing aspirin use before and after 7 days prior to surgery. Spine (Phila Pa 1976). 2013;38(18):1561-1565.[35] Cuellar JM, Petrizzo A, Vaswani R, et al. Does aspirin administration increase perioperative morbidity in patients with cardiac stents undergoing spinal surgery. Spine (Phila Pa 1976). 2015;40(9):629-635.[36] Kang SB, Cho KJ, Moon KH, et al. Does low-dose aspirin increase blood loss after spinal fusion surgery. Spine J. 2011; 11(4):303-307.[37] Zhang C, Wang G, Liu X, et al. Safety of continuing aspirin therapy during spinal surgery: A systematic review and meta-analysis. Medicine (Baltimore). 2017;96(46):e8603.[38] Goes R, Muskens IS, Smith TR, et al. Risk of aspirin continuation in spinal surgery: a systematic review and meta-analysis. Spine J. 2017;17(12):1939-1946.[39] Burger W, Chemnitius JM, Kneissl GD, et al. Low-dose aspirin for secondary cardiovascular prevention - cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation - review and meta-analysis. J Intern Med. 2005;257(5):399-414.[40] Devereaux PJ, Goldman L, Cook DJ, et al. Perioperative cardiac events in patients undergoing noncardiac surgery: a review of the magnitude of the problem, the pathophysiology of the events and methods to estimate and communicate risk. CMAJ. 2005;173(6):627-634. |
| [1] | Zhang Tongtong, Wang Zhonghua, Wen Jie, Song Yuxin, Liu Lin. Application of three-dimensional printing model in surgical resection and reconstruction of cervical tumor [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(9): 1335-1339. |
| [2] | Zeng Yanhua, Hao Yanlei. In vitro culture and purification of Schwann cells: a systematic review [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(7): 1135-1141. |
| [3] | Xu Dongzi, Zhang Ting, Ouyang Zhaolian. The global competitive situation of cardiac tissue engineering based on patent analysis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(5): 807-812. |
| [4] | Wu Zijian, Hu Zhaoduan, Xie Youqiong, Wang Feng, Li Jia, Li Bocun, Cai Guowei, Peng Rui. Three-dimensional printing technology and bone tissue engineering research: literature metrology and visual analysis of research hotspots [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 564-569. |
| [5] | Chang Wenliao, Zhao Jie, Sun Xiaoliang, Wang Kun, Wu Guofeng, Zhou Jian, Li Shuxiang, Sun Han. Material selection, theoretical design and biomimetic function of artificial periosteum [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 600-606. |
| [6] | Liu Fei, Cui Yutao, Liu He. Advantages and problems of local antibiotic delivery system in the treatment of osteomyelitis [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 614-620. |
| [7] | Li Xiaozhuang, Duan Hao, Wang Weizhou, Tang Zhihong, Wang Yanghao, He Fei. Application of bone tissue engineering materials in the treatment of bone defect diseases in vivo [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 626-631. |
| [8] | Zhang Zhenkun, Li Zhe, Li Ya, Wang Yingying, Wang Yaping, Zhou Xinkui, Ma Shanshan, Guan Fangxia. Application of alginate based hydrogels/dressings in wound healing: sustained, dynamic and sequential release [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 638-643. |
| [9] | Chen Jiana, Qiu Yanling, Nie Minhai, Liu Xuqian. Tissue engineering scaffolds in repairing oral and maxillofacial soft tissue defects [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(4): 644-650. |
| [10] | Xing Hao, Zhang Yonghong, Wang Dong. Advantages and disadvantages of repairing large-segment bone defect [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(3): 426-430. |
| [11] | Chen Siqi, Xian Debin, Xu Rongsheng, Qin Zhongjie, Zhang Lei, Xia Delin. Effects of bone marrow mesenchymal stem cells and human umbilical vein endothelial cells combined with hydroxyapatite-tricalcium phosphate scaffolds on early angiogenesis in skull defect repair in rats [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3458-3465. |
| [12] | Wang Hao, Chen Mingxue, Li Junkang, Luo Xujiang, Peng Liqing, Li Huo, Huang Bo, Tian Guangzhao, Liu Shuyun, Sui Xiang, Huang Jingxiang, Guo Quanyi, Lu Xiaobo. Decellularized porcine skin matrix for tissue-engineered meniscus scaffold [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3473-3478. |
| [13] | Mo Jianling, He Shaoru, Feng Bowen, Jian Minqiao, Zhang Xiaohui, Liu Caisheng, Liang Yijing, Liu Yumei, Chen Liang, Zhou Haiyu, Liu Yanhui. Forming prevascularized cell sheets and the expression of angiogenesis-related factors [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3479-3486. |
| [14] | Liu Chang, Li Datong, Liu Yuan, Kong Lingbo, Guo Rui, Yang Lixue, Hao Dingjun, He Baorong. Poor efficacy after vertebral augmentation surgery of acute symptomatic thoracolumbar osteoporotic compression fracture: relationship with bone cement, bone mineral density, and adjacent fractures [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3510-3516. |
| [15] | Liu Liyong, Zhou Lei. Research and development status and development trend of hydrogel in tissue engineering based on patent information [J]. Chinese Journal of Tissue Engineering Research, 2021, 25(22): 3527-3533. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||